Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Adv-262b_1 tipin
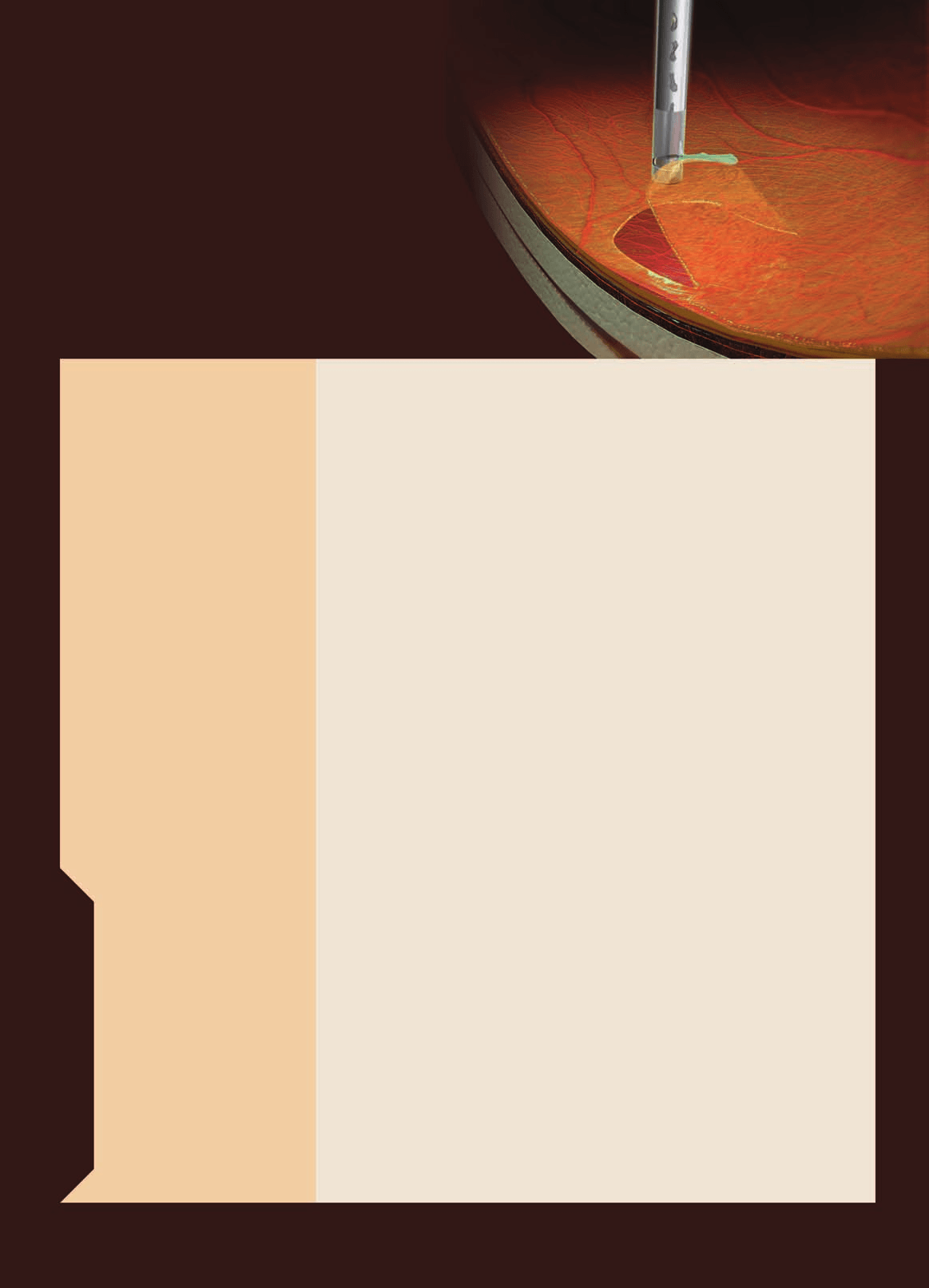
July 2006 • Supplement to Ophthalmology Times INNOVATIVE TECHNOLOGIES IN VITREORETINAL Highlights from a roundtable discussion held at the 2006 World Ophthalmology Congress in São Paulo, Brazil, on February 20, 2006 MODERATOR George A. Williams, MD OVER THE PAST 5 YEARS, VITRECTOMY the rate of complications. The increased
technology has undergone a revolution. Clinical Professor of Biomedical SciencesDr. Rizzo: In Italy, I have coordinated an PARTICIPANTS
standard vitrectomy (800 cpm). Duringthis study, patients affected by various vit-
Periklis Brazitikos, MD
surgeon to focus on the patient’s eye as
Assistant Professor of Ophthalmology
flow with the pedal. Recently, a group of
vitrectomy. Results from our study showed
Michel Farah, MD
met to discuss 3D technology and its ele-
reduces surgical time, consumption of bal-
ments. The specialists also offered their
opinions on high-speed cutting in various
surgical approaches. Highlights from that
the high-speed cutter does not require the
use of scissors or forceps to dissect mem-
Dr. Williams: What are the primary advantages of high-speed cutting? Dr. Farah: We have all had an opportunity
orifice pressure variation that occurs with
Hugo Quiroz-Mercado, MD
to use this technology for some time, and
we used a cutting rate of 400 to 500 cuts
per minute (cpm). At the time, we didn’t
Stanislao Rizzo, MD
control of the vitrectomy. It has greatly
less fluctuation in pressure, and a greater
fluidic stability. At the same flow rate,
Eye Surgery DepartmentUO Chirurgia OftalmicaOspedale Santa ChiaraAziende Ospedaliero-
The views and opinions expressed in this supplement are those of the participants and do not necessarily reflect the
views and opinions of Advanstar Communications Inc, publisher of Ophthalmology Times.
Funded and produced with the assistance of
high-speed cutting reduces iatrogenic tractions and increases
relating to retinal damage were more common. The surgeon
vitreous chamber stability, allowing the surgeon to approach
is also more independent with this technology, because it is
no longer necessary to ask a nurse to change the parameters. In our hospital, we find that using 3D technology to dissect
Dr. Williams: Have the high-speed cutters enabled you to
fibrotic tissue close to the retina surface reduces the risk of
approach tissue differently than you could in the past? retinal damage. In certain cases of proliferative diabetic Dr. Farah: Yes, without a doubt. We can use the high-speed
retinopathy, we could perform segmentation without the
cutters much closer to the retina, and we can remove
need of scissors. It’s amazing how close to the retina you can
fibrovascular tissues. With this technology, we have to enter,
use high-speed cutting without causing a tear.
leave, and reenter the eye much less frequently, and we have
Dr. Rizzo: With high-speed cutters, I use the stalk-chop
fewer complications at the entry site. High-speed cutting also
technique and approach dense membranes directly with a
speeds up the surgery. With the right technique, we can use
vitrectomy probe, using minimal flow, a cut rate of 2500 cpm,
this technology to remove tissue that’s connected to the
vacuum of 0-40 mmHg, and infusion of 60 cc. Moreover, in
retina. There is a learning curve associated with it, but the
the presence of dense hemovitreous or clots, my core vitrec-
tomy is quicker. The 3D technology enables me to control allparameters by using the foot pedal. Dr. Williams: How do you use this technology in the IT’S AMAZING HOW CLOSE TO THE management of retinal detachment patients under- RETINA YOU CAN USE HIGH-SPEED going primary vitrectomy? CUTTING WITHOUT CAUSING A TEAR. Dr. Brazitikos: In cases of detached retinas, the use of high- HUGO QUIROZ-MERCADO, MD
speed cutting produces less motion of the retina. We canapproach this tissue more closely and safely remove the
Dr. Williams: That learning curve is important. We now
peripheral vitreous. Before high-speed cutting was avail-
have a much better understanding of what we’re doing in
able, I used a lot of perfluorocarbon liquid (PCL) in many
surgery. In the past, we often focused our attention on the
cases of primary vitrectomy for retinal detachment to over-
suction and numbers on a gauge. In reality, we’re trying to
come the motion of the peripheral retina while trying to
manage flow. There are numerous ways to do that. We now
remove the vitreous. Today when we do primary vitrectomy
have technologies that allow us to control flow, vacuum,
with high-speed cutting, I almost never use perfluoro-N-
and cutting rates simultaneously. By affecting the duty
octane or other PCLs. I also find it much easier to teach
cycle, we can titrate nicely and precisely control our cut-
residents to perform safer removal of the peripheral vitre-
Dr. Rizzo: During vitrectomy, we work in a complex environ- Dr. Williams: What are the ramifications of using a low
ment with varying viscosity, dealing with substances, such as
cut rate? When compared with a high cut rate, why is
vitreous, blood, BSS®, and attached and detached retina,
a low cut rate advantageous for very thick tissue, such
with different densities. Using the high-speed cutters, I can
as a lens?
manage these tissues without worrying about the sudden
Dr. Quiroz-Mercado: Generally, I use a low cut rate for lens
increase in the aspirating flow that occurs when aspirating
removal. Its advantages relate to the deformability of the tis-
BSS® after a dense material. This is important because most
sue that you’re cutting. When you have very solid tissuelike
vitrectomy machines use a modified venturi pump that doesn’t
lens material, you need more time for the port to be open so
allow direct control of flow, which is dependent on the den-
sity of aspirated material and the cutting rate. In contrast,using a peristaltic pump with constant pedal depression
Dr. Rizzo: I only use a low cutting rate for a lens fragment or
decreases the gradient of pressure when aspirating less vis-
a soft dislocated/subluxated lens (such as in patients younger
cous material with the same flow. High-speed cutting can
than 45 years with Marfan syndrome or following trauma). In
reduce the difference in aspiration flow due to fluid viscosity,
other cases, I perform combo anterior phaco to preserve the
thus enhancing the safety of a venturi pump.
posterior capsula. For a dislocated lens with a hardnessgreater than 2+, I use endophaco. Based on the unproven
Dr. Williams: How do you use 3D technology and high- speed cutters in your diabetic population?
theory that reduced cutting rates allow tissue to enter theport between cutting cycles, many surgeons recommend low
Dr. Quiroz-Mercado: We saw a dramatic change on the learn-
cutting rates to remove membranes and lens material. I
ing curve of our fellows with the introduction of the 3D
believe that using low cutting rates increases the likehood of
technology. In the past, when we only had linear aspiration
fluid surge following elastic deformation through the port as
and did not have the high cut rate we have now, accidents
Dr. Williams: How do you use the VGFI® technology?
I’m about to do the procedure, but over the main vessel that Iam going to cut. Then I use scissors. If I have trouble doing a
Dr. Quiroz-Mercado: This is a very interesting system. With it,
perfect retinotomy, I do a vitrectomy, using very low aspiration
we have the ability to control intraocular pressure (IOP),
and a high rate to ensure good control of the tissue removal.
mainly in cases where we must manage bleeding.
Dr. Rizzo: I use a 20-gauge high-speed vitrectomy cutter, Dr. Rizzo: Whenever possible, I use VGFI® technology. In
because it reduces surgical time. I prefer to avoid the use of
my experience, it plays a more crucial role in small-gauge
25-gauge technology in severe PVR, as it results in a pro-
longed vitrectomy. Currently, the 25-gauge tools are too
Dr. Williams: Would it be of any value if we could meas-
challenging and time-consuming to use to perform complete
ure the absolute pressure in real time? Dr. Farah: I believe so, because you are never absolutely sure Dr. Williams: After you complete a retinotomy, do you
if there is any leakage or other variable that may influence the
typically remove the anterior vitreous base and ante-
IOP. Sometimes we think we have done a great job, with good
rior retinal flap?
perfusion of nerve, and then we have some atrophy after the
Dr. Farah: Yes, I do. Although when I do the retinotomy, I try
surgery. This may indicate that somehow, for a certain period
to do as much as peripherally as I possibly can. I prefer to par-
of time during surgery, we lost perfect control of the eye.
tially remove the anterior retina. I don’t think it matters if
Dr. Rizzo: It would be great. At present, we only know the
there is just a small, thin layer of anterior retina remaining.
value set on the machine, so we can have a leak or a delay in
Dr. Rizzo: Yes, I do as well.
equalizing the pressure inside the eye with the set value. Thepossibility of measuring the absolute pressure in real time is
Dr. Quiroz-Mercado: You can start removing the membrane
also crucial for small-gauge vitrectomy.
either from the periphery or from the posterior pole. I preferto start from the posterior pole, injecting PCL and pulling the
Dr. Williams: At what pressure do you typically prefer
membrane with the forceps. When I reach the peripheral
to operate?
retina, I perform relaxing retinotomy if the retina does not
Dr. Farah: Usually, 30 mmHg. I use 60 or 70 mmHg when I
reattach. In such cases, I must identify and remove mem-
branes either on the surface of or under the retina. Dr. Rizzo: I also typically use 30 mmHg and 60 or 70 mmHg Dr. Williams: Do you find that you are now doing fewer buckles in your PVR patients with this technology? Dr. Williams: That’s a good point. We have the ability to raise Dr. Quiroz-Mercado: For most PVR cases, I recommend using
the pressure in anticipation of bleeding. We’re all familiar
a buckle. In severe cases, it may not be necessary.
with the difficulty that can accompany a large hemorrhage. Dr. Brazitikos: I try to start with a 25-gauge system in PVR
Many times, removing those clots can be more difficult than
cases, and I can withdraw mature membranes with 25-gauge
performing the initial dissection was. An experienced surgeon
forceps. I am also trying to start the membrane removal from the
can anticipate bleeding and raise the pressure, even for
posterior pole. I gradually inject PCL and see if there is some
extended periods of time while completing the dissection,
residual traction. I ask the assistant to put some pressure on the
and then slowly lower it again. That approach lets the sur-
sclera, and we see if we can balance this residual traction.
geon identify specific bleeders. Then he or she can have alaser or diathermy ready to go.
Dr. Rizzo: No, I don’t. If I have to treat PVR, I usually associ- ate a broad, encircling 4- to 7-mm band with 20-gauge Dr. Brazitikos: It is necessary to know exactly what the pres-
sure in the eye is. With the VGFI® system, we seem to beusing less and less unnecessary diathermy today. And once
Dr. Williams: Do you tend to diathermize the major
the dissection has been completed, we can lower the pres-
vessels first?
sure gradually. If we see some bleeding, we do somediathermy precisely on these bleeding sites.
Dr. Brazitikos: Not always. Because you may have some hemostasis, and some of these vessels will not always bleed. Dr. Williams: Have you used this technology in severe
Some bleed, and some do not. Sometimes you end up doing
cases of proliferative vitreoretinopathy (PVR)?
more diathermy than is necessary. If you have some bleedingafter posterior capsule opacification, you can easily target
Dr. Farah: I don’t usually use the 25-gauge system for PVR
these vessels and do some diathermy.
cases. I am more likely to use the 20-gauge system in thosepatients. I like to have more instrumentation available, and I
Dr. Rizzo: When I perform a posterior retinotomy, yes, I do.
find that it’s faster and safer to use the 20-gauge system. When
For a peripheral retinotomy, I don’t. When dealing with a
I do a retinectomy, I do diathermy first, not over the area where
fibrovascular stalk, I prefer to avoid bleeding by using high
infusion-pressure values or exerting mechanical compression
movement, and our ability to control that flow gives us preci-
on the vessel with the tip of a blunt tool.
sion. This surgical equipment is so much easier to use thanwhat we had in the past. As our instruments continually
Dr. Williams: Are any of the staining techniques useful
improve, it becomes more difficult for us as surgeons to com-
prehend their true capabilities. If a surgeon doesn’t take the
Dr. Brazitikos: I sometimes try staining to visualize some
time to learn what this new equipment can do, he or she will
membranes that we cannot always see. In my experience,
this enables us to see more membranes. I don’t know why. Dr. Quiroz-Mercado: I’ve noticed that young surgeons under-
But I don’t think staining is useful in all cases.
stand 3D well and take advantage of its technology. Some
Dr. Quiroz-Mercado: I often do staining of the vitreous as well as
surgeons who are more familiar with the linear technology do
staining of membranes like the internal limiting membrane
not accept 3D until they have a good understanding of it and
(ILM). To visualize the vitreous, I prefer triamcinolone, which
have practiced using it several times. Then they can see its
helps us see the vitreous cortex at the periphery and posterior
advantages, which include safe cutting, retina stabilization,
pole. In some cases, such as with highly myopic eyes, the use of
triamcinolone is fundamental for observing vitreous remnants in
Dr. Brazitikos: It is much easier to realize these advantages
the macula in the presence of staphyloma. To stain ILM, I use
when you are actually doing vitrectomy rather than talking or
trypan blue. If it is not well visualized, I use indocyanine green
reading about it. Apparently, the third dimension of 3D con-
(ICG). In rare cases I use triamcinolone to visualize the ILM.
trol is flow. It is safer to start with high-speed cutting andlower vacuum. With this parameter setting, you can have lessflow during surgery. This is safer when you first enter the eye
WITH THE VGFI® SYSTEM,
and start working close to the retina. When you are doinghigh-speed cutting and the vitreous flow in the port is low, or
WE SEEM TO BE USING LESS AND LESS
the vitrectomy is taking too long, you step on the pedal and
UNNECESSARY DIATHERMY TODAY.
increase vacuum while decreasing the cut rate. This adjust-
PERIKLIS BRAZITIKOS, MD
ment will give you more flow, so you can remove the vitreousfaster. I find that this interplay between high- and low-speedcutting enables you to finish surgery faster and safer. Dr. Rizzo: I find that chromovitrectomy is. I routinely instill tri- amcinolone to highlight the vitreous gel and the posterior hyaloid Dr. Williams: The take-home message seems to be that the
membrane at the periphery and at the posterior pole. I also stain
surgeon is in control and can adjust these parameters to suit
epiretinal membranes with trypan blue and ILM using ICG.
a specific case. It’s an interesting approach. Why is the flowlow with high cutting rates? With a high cutting rate, the port
Dr. Williams: How does the foot pedal work? What set- tings do you use?
is open for a shorter period of time. I believe that the conceptis called aperture limited flow. Basically, this means that at
Dr. Farah: I start with a high cutting rate and low vacuum, so
higher cutting rates, the length of time the port remains open
I can maintain low flow. Pressing down on the pedal lowers
is shorter than the time it is at lower cutting rates. This pro-
the cutting rate and raises the vacuum. I believe this is a safer
vides a second control of the flow. We can adjust the vacuum,
position. I usually start with 50 mmHg of vacuum, so I have
which obviously affects flow, and we can also control the
more time before it starts to increase when I press the pedal.
length of time that the cutting port is actually open. These
Using the pedal reminds me of driving my car. When I am in
a riskier situation, close to the retina, I take my foot off thepedal. It’s not the speed of the car that I’m reducing but the
risk. How does taking my foot off the pedal lower the risk? I
High-speed cutting provides surgeons with enhanced control of
know that it decreases the aspiration and increases the cut-
the vitrectomy and fewer complications. Surgeons can use the
ting speed, and that, in turn, lowers the risk.
high-speed cutters much closer to the retina. 3D technology grants
Dr. Williams: So it’s intuitive? Just as when you let up on
the surgeon more independence, as he or she can change param-
the accelerator of a car, you are more in control?
eters by stepping on a foot pedal. This feature also allows surgeonsto manage flow simultaneously with the vacuum and cutting rates. Dr. Farah: Yes, it’s similar to using the accelerator on a car.
Other surgical benefits include lower flow when working close to
When I take the pressure off the accelerator, I’m in a much
the retina and higher flow for faster core vitrectomy. Further, the
3D technology enables surgeons to concentrate on the patient’seye rather than on gauges and settings. Dr. Williams: As we discussed earlier, we need to understand that cutting and vacuum are interchangeable parameters that
Accurus is a registered trademark of Alcon Manufacturing LTD.
control flow, and that’s what we do. Flow drives vitreous
VGFI is a registered trademark of Alcon, Inc.
THE EMERGING ROLE OF INTEGRATED MARKETING IN THE PHARMACEUTICAL INDUSTRY AN EXAMINATION OF DIRECT-TO-CONSUMER PRESCRIPTION DRUG COMMUNICATIONS As prescription drug manufacturers increasingly target consumers through integrated marketing com-munications strategies, questions of ethics inevitably arise. Anne Gibson explores the role pharma-ceutical companies’ direct-to-consumer IMC campai
LH-ELISA KAPD1289 DIAsource ImmunoAssays S.A. - Rue du Bosquet, 2 - B-1348 Louvain-la-Neuve - Belgium KAPD1289 IN VITRO DIAGNOSTIC USE DIAsource ImmunoAssays SA - Rue du Bosquet 2, B-1348 Louvain-la-Neuve, Belgium - Tel: +32 10 84 99 11 - Fax : +32 10 84 99 90 INTRODUCTION Intended Use The DIAsource LH ELISA Kit is an enzyme immunoassay for the quantitative
 July 2006 • Supplement to Ophthalmology Times
July 2006 • Supplement to Ophthalmology Times high-speed cutting reduces iatrogenic tractions and increases
relating to retinal damage were more common. The surgeon
vitreous chamber stability, allowing the surgeon to approach
is also more independent with this technology, because it is
no longer necessary to ask a nurse to change the parameters.
high-speed cutting reduces iatrogenic tractions and increases
relating to retinal damage were more common. The surgeon
vitreous chamber stability, allowing the surgeon to approach
is also more independent with this technology, because it is
no longer necessary to ask a nurse to change the parameters. Dr. Williams: How do you use the VGFI® technology?
Dr. Williams: How do you use the VGFI® technology?  infusion-pressure values or exerting mechanical compression
movement, and our ability to control that flow gives us preci-
on the vessel with the tip of a blunt tool.
infusion-pressure values or exerting mechanical compression
movement, and our ability to control that flow gives us preci-
on the vessel with the tip of a blunt tool.