Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Scientific programme: neurology. in: proceedings of the 49th british equine veterinary association congress, 2010 - birmingham
Thurs H5 v2_Layout 1 17/08/2010 16:00 Page 52
Reprinted in IVIS with the permission of BEVA
Thursday 9th September 2010 Neurology Sponsored by University of Liverpool16.20–16.40 ‘How to’ interpret equine cervical radiographs and other imaging modalities Richard J. Piercy Royal Veterinary College, London, UK.
Plain radiography of the cervical vertebrae can be used to assess
lesions occur between, rather than within, the vertebrae (Hahn et
the likelihood of cervical stenotic myelopathy in horses with spinal
al. 2008). Particularly high quality radiographs are usually required
ataxia (Moore et al. 1994), but accurate assessment requires a
for such measurements, but analysis suggests that this approach
precise lateral radiograph (Rush 1998), ensuring that the ventral
may be helpful in differentiating CSM from other conditions (Van
prominences of the transverse processes are perfectly overlying
Biervliet 2007). Further comparison of both methods in a large
each other. Radiographic obliquity results in indistinct margins of
group of horses is needed based on a gold standard diagnosis
the ventral aspect of the vertebral canal and results in erroneous
established at post mortem examination, since myelography is
values for objective measurements. A thorough understanding of
problematic (see discussion below), although available post
the 3 dimensional anatomy of the cervical vertebrae aids in
mortem material may be skewed towards severely affected horses,
interpretation (Withers et al. 2009).
since these animals may more often be subjected to euthanasia.
Cervical radiographs should be evaluated subjectively and
Plain radiography is often considered sufficient to make a
objectively. Subjective interpretation is based on examining for
presumptive diagnosis of cervical compression without the need
presence of 5 characteristic malformations of the cervical vertebrae
for further tests. In countries where EPM or other conflicting
that include (1) flare of the caudal epiphysis of the vertebral body;
differential diagnoses are possibilities, many clinicians favour
(2) abnormal ossification of the articular processes; (3)
myelography for diagnosis. Unfortunately, for most inter-vertebral
subluxation/misalignment between adjacent vertebrae; (4) extension
sites, myelography results in a high number of false positive and
of the vertebral caudal dorsal lamina and (5) osteoarthritis of the
false negative results (van Biervliet et al. 2004). Myelography
articular processes. Estimating the significance of lesions identified
remains, however, a prerequisite if surgical intervention is
through subjective interpretation can be hard and is based on the
considered a viable option on the basis of severity of signs and
clinician’s experience and interpreting the balance of probability. For
the owner’s wishes and expectations. This is because plain
example, osteoarthritis of (especially the caudal) vertebral articular
standing radiography does not definitively pinpoint the actual site
processes is recognised commonly in normal horses (Whitwell and
of the compressive lesion(s) (Moore et al. 1994). Note that neck
Dyson 1987). Hence recognition of characteristic vertebral
flexion and extension while under anaesthesia are contraindicatedif there is evidence of compression on the initial neutral views.
malformations is considered supportive in diagnosis at best
Ventrodorsal projections may be attempted in small or young
(Papageorges et al. 1987). Oblique radiographs are helpful in certain
animals, especially in the cranial neck and may demonstrate an
circumstances (Withers et al. 2009).
assymetric compressive lesion that might otherwise account for
Objective assessment of vertebral canal diameter is more
some false negative diagnoses in larger horses.
accurate than subjective evaluation of vertebral malformation foridentifying young horses affected by CSM but may lead to false
References
negative diagnoses in older horses (Levine et al. 2007). Both inter-
Hahn, C.N., Handel, I., Green, S.L., Bronsvoort, M.B. and Mayhew, I.G. (2008)
and intra-vertebral measurements are used. The sensitivity and
Assessment of the utility of using intra- and intervertebral minimum sagittal
specificity of the intra-vertebral sagittal ratio method is
diameter ratios in the diagnosis of cervical vertebral malformation in horses. Vet.
approximately 90% for vertebral sites between the third and
Radiol. Ultrasound 49, 1-6.
seventh cervical vertebrae (Moore et al. 1994). In most normal
Levine, J.M., Adam, E., MacKay, R.J., Walker, M.A., Frederick, J.D. and Cohen, N.D.
(2007) Confirmed and presumptive cervical vertebral compressive myelopathy in
horses, the sagittal ratio exceeds 52% from the third to sixth
older horses: a retrospective study (1992-2004). J. vet. intern. Med. 21, 812-819.
cervical vertebrae and 56% at the seventh cervical vertebrae in
Moore, B.R., Reed, S.M., Biller, D.S., Kohn, C.W. and Weisbrode, S.E. (1994) Assessment
horses greater than 320 kg. The positive predictive value of such
of vertebral canal diameter and bony malformations of the cervical part of the spine in horses with cervical stenotic myelopathy. Am. J. vet. Res. 55, 5-13.
measurements is probably higher and the negative predictive value
Papageorges, M., Gavin, P.R., Sande, R.D., Barbee, D.D. and Grant, B.D. (1987)
lower, in ataxic horses from countries where conflicting diagnoses
Radiographic and myelographic examination of the cervical vertebral column in
(such as EPM) are not routinely encountered (i.e. false positives are
306 ataxic horses. Vet. Radiol. 28, 53.
less likely, but false negatives are more likely because the underlying
Rush, B.R. (1998) Spinal radiography and myelography. In: Current Techniques inEquine Surgery and Lameness, 2nd edn., Eds: N.A. White and J.N. Moore, W.B.
prevalence of CSM in ataxic horses is higher). Similarly, the positive
and negative predictive values of objective cervical radiography
Van Biervliet, J. (2007) An evidence-based approach to clinical questions in the practice
measurements in the absence of ataxia (for example during
of equine neurology. Vet. Clin. N. Am.: Equine Pract. 23, 317-328.
prepurchase radiography) have not been evaluated, but false
van Biervliet, J., Scrivani, P.V., Divers, T.J., Erb, H.N., de Lahunta, A. and Nixon, A. (2004)
Evaluation of decision criteria for detection of spinal cord compression based on
positives are likely to be more, and false negatives, less common,
cervical myelography in horses: 38 cases (1981-2001). Equine vet. J. 36, 14-20.
since the prevalence of CSM in this population will be much lower.
Whitwell, K.E. and Dyson, S. (1987) Interpreting radiographs. 8: Equine cervical
Some clinicians advocate use of ratiometric measurements that
vertebrae. Equine vet. J. 19, 8-14.
take into account the distance between adjacent vertebrae (inter-
Withers, J.M., Voute, L.C., Hammond, G. and Lischer, C.J. (2009) Radiographic
anatomy of the articular process joints of the caudal cervical vertebrae in the
vertebral ratios) based on the rationale that most compressive
horse on lateral and oblique projections. Equine vet. J. 41, 895-902.
Proceedings of the 49th British Equine Veterinary Association Congress 2010 - Birmingham, United Kingdom
Thurs H5 v2_Layout 1 17/08/2010 16:00 Page 53
Reprinted in IVIS with the permission of BEVA
Thursday 9th September 2010 16.40–16.50 ‘How to’ inject cervical vertebral facets, using ultrasound guidance Richard Hepburn The Willesley Equine Clinic, B&W Equine Group, Byams Farm, Willesley, Tetbury, Gloucestershire GL8 8QU, UK.
A thorough understanding of cervical vertebral anatomy and the
needle entry will vary greatly with head position. The probe should
ultrasonographic appearance of the cervical vertebral facet joints
be placed inside a sterile glove or probe cover that has been filled
is essential before attempting facet injections. This author
with a small amount of acoustic gel. The horse’s head is then held
recommends Berg et al. (2003), which has excellent images
in a neutral position. An image of the affected joint is obtained,
showing the location and appearance of the cervical facets.
with the joint space positioned centrally within the scan image.
Cervical facet joints are formed from the caudal articular
The depth of the joint should be noted (typically about 4–5 cm).
process of the cranial vertebra and the cranial process of the
The probe is then held in a fixed position, and a 12.5 cm 18 gauge
caudal vertebra. The joint is the most dorso-lateral point of the
spinal needle is inserted approximately 1 cm dorsal to the probe,
vertebra, being approximately 4–6 cm dorsal to the palpable
with its long axis parallel to the long access of the probe, at a
transverse processes, and sits at an angle of approximately 30–40°
downward angle that will cause the needle to cross the centre of
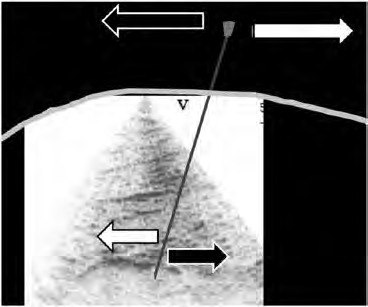
the ultrasound image at the depth of the facet joint. The needle
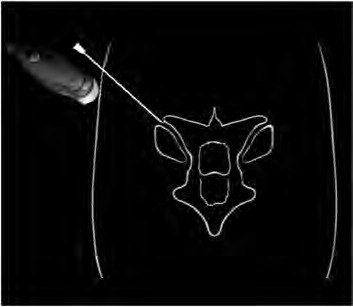
Imaging the facet joints for injection is most effectively
is then advanced towards and into the joint and is seen as a
performed using a micro-convex or phased array probe (6–10
hyperechoic line on the ultrasound screen. Repositioning can be
MHz, 4–8 cm depth), as the small footprint facilitates easy needle
required and can initially be confusing (Fig 2).
placement (Fig 1).
With the standard image right is dorsal and left is ventral.
A 10 cm square area dorsal to the transverse process of the
The skin acts as a pivot: to move the tip of the needle dorsally,
affected vertebra should be clipped with a No. 40 blade. A
the hub should be moved ventrally and vice versa. Alternatively,
standardised approach to the ultrasound image aids interpretation
a biopsy guide can be attached to the probe and the biopsy line
- this author always positions the probe reference dorsal, with the
on the ultrasound machine positioned so it transects the joint;
screen reference to the right, and holds the probe in a transverse
however, if the horse moves excessively during needle placement
orientation. The probe is placed 8–10 cm dorsal to the palpable
the biopsy guide can prevent easy repositioning. Both techniques
transverse process, angled slightly downwards and then moved
are equally accurate, with 89% injections being either intra-
ventrally until the joint margins are imaged. If vertebral body is
articular or intracapsular (Nielsen et al. 2003).
imaged the probe should be moved cranially or caudally to image
The needle will typically enter the joint margin easily, if not
facet neck and then joint. Angling the probe in a slight cranial
raising the head can open the joint space. No attempt should be
direction can aid identification of the joint space. The facet joint
made to advance the needle deeper as dural puncture could
margins are seen as 2 crescent shaped hyperechoic contours which
occur. Synovial fluid will occasionally flow spontaneously or can
cast acoustic shadows, separated by an anechoic joint space. It is
be aspirated. Injection should be easy and if resistance is felt the
often possible to image deeper into the joint space. A reasonable
needle should be rotated or withdrawn 1–2 mm as the tip may
degree of variation in ultrasonographic appearance occurs
be embedded in articular cartilage. Injection should be directly
between horses and between individual facet joints. Small
visualised as hyperechoic sparkling within the joint space. Whilst
osteophytes can often be imaged, as can some lipping of the joint
communication between the left and right facets of a given
margins. Significant changes include proliferation of bone dorsally,
articulation can occur, they should essentially be treated as
multiple osteophytes and widening of the joint space.
separate joints and injected individually. This author uses either
Prior to injection the horse should be sedated (0.01 mg/kg
triamcinolone acetate when injecting 2 facet joints (16 mg max
bwt detomidine and 0.01 mg/kg bwt butorphanol) and
per horse - 8 mg/joint), or methyl-prednisolone acetate when
pretreated with a NSAID (1 mg/kg bwt flunixin meglumine) to
limit muscular discomfort from the procedure. The clipped area
The reader should be aware that an alternative technique
over the affected joint should then be prepared aseptically. The
exists, where the ventral margin of the facet is injected, with the
use of local anaesthetic is typically unrewarding as the location of
needle positioned ventral to the probe, with the joint space
Proceedings of the 49th British Equine Veterinary Association Congress 2010 - Birmingham, United Kingdom
Infl uência do treinamento físico sob parâmetros metabólicos e ósseos de ratos submetidos à administração de dexametasona. José Alexandre Leme 1, José Rodrigo Pauli2,, Daniel Manuel Crespilho1, Ricardo José Gomes3, Eliete Luciano e Maria Alice de 1 UNESP, Rio Claro, Brasil2 UNICAMP, Campinas, São Paulo-Brasil 3 FCELIFUL, Registro, São Paulo-Brasil4 USP, Rio Claro, São Paulo-Bra


 Thurs H5 v2_Layout 1 17/08/2010 16:00 Page 52
Reprinted in IVIS with the permission of BEVA
Thursday 9th September 2010
Thurs H5 v2_Layout 1 17/08/2010 16:00 Page 52
Reprinted in IVIS with the permission of BEVA
Thursday 9th September 2010 

 Thurs H5 v2_Layout 1 17/08/2010 16:00 Page 53
Reprinted in IVIS with the permission of BEVA
Thursday 9th September 2010
Thurs H5 v2_Layout 1 17/08/2010 16:00 Page 53
Reprinted in IVIS with the permission of BEVA
Thursday 9th September 2010