Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
2002019
The Effect of Inhaled Budesonide on Symptoms, Lung Function, and Cold Air and Methacholine Responsiveness in 2- to 5-year–old Asthmatic Children KIM GJERUM NIELSEN and HANS BISGAARD
Department of Pediatrics, Copenhagen University Hospital, Rigshospitalet, Copenhagen, Denmark
We hypothesized that measurement of lung function (LF) and
single readings may occasionally be obtained, poor repeatabil-
bronchial hyperresponsiveness (BHR) could serve as supplemental
ity prevents the use of conventional methods for measuring
tools in evaluating the efficacy of treatment with inhaled cortico-
lung function (9, 10). Recently, we successfully adapted the
steroids in asthmatic children aged 2 to 5 yr. We studied 38 chil-
measurement of specific airway resistance (sRaw) by whole-
dren (mean age: 53 mo; range: 35 to 71 mo) with moderately se-
body plethysmography; resistance measured with the inter-
vere asthma in a single-center, randomized, double-blind, parallel-
rupter technique (Rint); and resistance and reactance at 5 Hz
group, placebo-controlled study involving 8 wk of treatment.
(Rrs5, Xrs5) as measured with the impulse oscillation (IOS)
Budesonide (BUD) 400 g twice daily was administered via a pres-
technique for use in awake children aged 2 yr and older (11–
surized metered-dose inhaler and metal spacer device. Symptom
13). These methods require no active cooperation by the
scores (SSc) and use of short-acting 2-agonist were monitored
young child, are well accepted by the child, and are more sen-
with diary cards. LF in awake children was measured as the specific
sitive than spirometry for detecting the response to methacho-
airway resistance (sRaw), using whole-body plethysmography; as resistance by the interrupter technique (Rint); and as resistance and reactance at 5 Hz (Rrs5, Xrs5) by the impulse oscillation tech-
Bronchial hyperresponsiveness (BHR) is an essential fea-
nique. Cold air challenge (CACh) and methacholine challenge
ture of the pathophysiology and clinical manifestation of
(MCh) were used to assess BHR. Children in the BUD group experi-
childhood asthma (14), and is related to disease control. Bron-
enced significantly fewer night- and daytime symptoms (p Ͻ 0.05)
choconstriction induced by hyperventilation of cold, dry air is
and more symptom-free days (p Ͻ 0.05), but not nights (p ϭ
commonly found in asthmatic adults and children, and can be
0.07), than children in the placebo group. Daytime (p Ͻ 0.05) but
used to assess BHR (15–21). The challenge with cold, dry air
not nighttime (p ϭ 0.09) use of rescue medication and asthma ex-
has two main attractive features: the reaction probably reflects
acerbation rates (3.7 versus 9.3 exacerbations/yr) (p ϭ 0.006)
the pathophysiology of asthma better than does pharmaco-
were both in favor of BUD. LF measured with the Rint technique,
logic bronchoprovocation with histamine or methacholine
Rrs5, and Xrs5 were significantly improved by BUD. BHR as mea-
(22), and the method is simple to perform and standardize
sured by CACh improved significantly with BUD, whereas no im-
even in children as young as 2 yr of age (23). We recently re-
provement was found on MCh. In conclusion, inhaled BUD at a
ported a sensitivity of 68% and a specificity of 93% using
total dose of 800 g daily significantly improved SSc, asthma exac-
sRaw and cold air challenge (CACh) in asthmatic children
erbation rates, lung function, and BHR as assessed by CACh in
from 2- to 5-yr old (23). Furthermore, we recently used this
asthmatic children aged 2 to 5 yr.
model to document clinically relevant bronchoprotection bythe leukotriene receptor antagonist montelukast (24).
Asthma is the most common chronic disease of young children
The aim of the present study was to evaluate the effect of
(1), and presents a considerable burden to the child, the fam-
budesonide (BUD) on symptoms, lung function (as measured
ily, and society because of its high prevalence and lack of good
through SRaw, Rint, Rrs5, and Xrs5), and BHR to CACh and
control with treatment. Diagnosis of asthma is ambiguous, ow-
methacholine challenge (MCh), with a view to evaluating
ing to the lack of objective measurements. The poor control of
whether these objective measures could serve as additional
asthma in young children is partly due to a lack of validated
tools in the study of symptomatic asthmatic children aged 2 to
objective methods for studying lung function and bronchial re-
activity in young children, which hampers both disease moni-toring and studies of pharmacotherapy.
The efficacy of inhaled corticosteroids (ICS) in young pre-
school children was first documented in our earlier study mon-
Patients
itoring symptom score (SSc) and use of rescue treatment (2).
Asthmatic children aged 2 to 5 yr from our outpatient clinic were eli-
Subsequent supportive trials have also been limited to such
gible for the study. The diagnosis of asthma was made empirically on
health outcomes (3–8), since objective measurements have not
the basis of recurrent asthma symptoms, clinical improvement with
regular ICS therapy, and relapse during interruption of treatment.
Young children under 6 yr of age can rarely perform the
Only patients fully cooperating in all lung function test procedures
maneuvers needed for lung function measurements, such as
and with CACh were considered for inclusion in the run-in period of
forced expiration, which require active cooperation. Although
the study. Asthma symptoms, use of rescue medication, and distur-bance of parents’ sleep were registered in a diary during the run-in pe-riod. Patients with a daily SSc of at least 4 (not including scoring ofparents’ sleep disturbance) on at least seven of 14 consecutive days
(Received in original form on February 7, 2000 and in revised form May 31, 2000)
Study Design
Correspondence and requests for reprints should be addressed to Hans Bisgaard,Professor of Paediatrics, Copenhagen University Hospital, Rigshospitalet, DK-
The study was a single-center, double-blind, parallel-group, random-
2100 Copenhagen, Denmark. E-mail: Bisgaard@RH.DK
ized, placebo-controlled trial. Patients who fulfilled the inclusion cri-
Am J Respir Crit Care Med Vol 162. pp 1500–1506, 2000
teria at Visit 1 entered an observational run-in period in which regular
Internet address: www.atsjournals.org
treatment was stopped and terbutaline as required was the only medi-
Nielsen and Bisgaard: Budesonide in Young Asthmatic Children
cation allowed. The run-in period lasted from 2 wk to a maximum of
Rint. Rint is based on the assumption of a simple relationship be-
8 wk, in which asthma symptoms, use of rescue medication, and distur-
tween mouth pressure at the end of interruption of airflow and the
bance of parents’ sleep were registered in a diary. Scoring during peri-
airflow after reopening of a shutter valve mounted on the pneumo-
ods with respiratory infections was suspended. Patients were excluded
tachograph. At every second inspiratory phase, inspiration of 50 ml of
if they received inhaled steroids or were hospitalized for asthma during
air activated the shutter for 80 ms. Mouth pressure was measured dur-
the run-in period. At randomization, both a CACh challenge test and
ing the last 5 ms of the interruption. Flow was measured over a 70-ms
an MCh test were performed within 72 h. Treatment medication and a
period after reopening of the shutter. The mean value of five consecu-
new diary card, identical to the one used during the run-in period,
tive measurements was used as the result.
were delivered after the last of the two challenge tests. Subjects were
Xrs5 and Rrs5. Xrs5 and Rrs5 were measured with the IOS tech-
scheduled for a visit after 4 wk of treatment. At this visit, diary cards
nique. Rectangular impulses were generated mechanically by a loud-
were checked, old medication was returned and new medication was
speaker and were applied to the respiratory system through the
delivered, and baseline lung function was measured. After 8 wk of
mouthpiece of the pneumotachograph. The resulting pressure and
treatment, CACh and MCh were repeated.
volume signals were analyzed for amplitude and phase difference to
The local ethics committee (KF-02-179/96) and the national health
determine the Xrs and Rrs of the respiratory system. Thirty seconds
authorities of Denmark approved the study. Written informed con-
of undisturbed measurements were used as the results (11, 12).
sent was obtained from parents or guardians of the subjects. CACh. Cold, dry air was generated by a respiratory heat exchange
system (RHES; Erich Jaeger). Methods and equipment used for the
Randomization and Treatment
CACh have previously been described in detail (23). The CACh wasdone as a single-step, 4-min, isocapnic hyperventilation test. We used
Subjects were randomly assigned to receive either two puffs of BUD
cold, dry air at Ϫ15Њ C, mixed with 5% CO . The subject breathed
200 g twice daily (total daily dose of 800 g budesonide) or two puffs
through a face mask fitted with a mouthpiece, which effectively se-
twice daily of placebo from a pressurized metered-dose inhaler
cured mouth breathing and prevented inhalation of room air. The rate
(pMDI) via a metal spacer (Nebuchamber, AstraZeneca, Lund, Swe-
of ventilation was 1 L/min/kg body weight. The subject was motivated
den). The randomization was computer generated in balanced blocks
to hyperventilate by competing with a computer-animated balloon,
which reflected the ventilation rate (23).
Inhaled 2-agonist, delivered via the pMDI and spacer, was used
The response to hyperventilation of cold, dry air was recorded at
as rescue medication throughout the study. In the case of moderate
4 min after the end of the challenge.
asthma attacks, one puff of formoterol 12 g twice daily, delivered
Methacholine challenge test. The MCh test was done as a multistep
from a pMDI and spacer, and/or a 3-d oral course of prednisolone at
challenge with a dosimetric method. Isotonic methacholine chloride so-
1 mg/kg body weight twice daily, was allowed at the discretion of the
lution was nebulized with a Wright nebulizer (Clement Clarke, Essex,
investigator. No other antiasthma medication was allowed. All short-
UK) that delivered aerosol into an aerosol box that prevented entrain-
and long-acting 2-agonists were stopped at 6 and 24 h, respectively,
ment of air (25). Methacholine was inhaled by tidal breathing from the
before baseline lung function measurement and bronchial provocation.
aerosol box through a face mask and mouthpiece. At each step of thechallenge the subject inhaled 200 ml of the aerosol per kilogram of
Assessments
body weight. Doubling concentrations of methacholine, from 0.0625 to
Diary cards. Diary cards were constructed according to the method
a maximum of 64 mg/ml, were used. Increasing doses were inhaled until
described in our previous study (7). Symptoms were scored on a scale
sRaw increased by 50%, the maximum methacholine dose of 64 mg/ml
of 0 to 3 (with a score of 0 indicating no symptoms and 1, 2, and 3 indi-
was reached, clinical airway obstruction was apparent, the subject com-
cating mild, moderate, and severe symptoms, respectively) by one of
plained of discomfort, or transcutaneous oxygen pressure (TcO ), which
the subject’s parents in three symptom domains (wheezing, cough,
was monitored continuously during provocation, exhibited a decrease
and shortness of breath), in addition to scoring for use of relief medi-
of у 3 kPa. The heated (44Њ C) transcutaneous pressure electrode was
cation for daytime symptoms and for nighttime symptoms individu-
placed on the middle part of the flexor side of the lower arm. Duplicate
ally. Furthermore, exercise-induced asthma symptoms during the day-
measurements of Rint were made 2 min after provocation at each step
time and parents’ sleep disturbance caused by subjects’ asthma during
until Rint had increased by 10% or more from baseline. At that point,
the night were scored on a scale of 0 to 3.
sRaw, Rrs5, or Xrs5 were measured in that sequence. Pulmonary function testing. Pulmonary function testing was done
The response to a challenge was measured at 3 to 5 min after the
with a Master Screen unit, version 4.22 (Erich Jaeger GmbH, Würzburg,
Germany). Flow and volume were measured with a heated pressure-screen–type pneumotachograph with a resistance of 0.036 kPa
The equipment was calibrated daily. The methods and equipment
Data Analysis
used for pulmonary function testing have previously been described
Study variables. Primary outcome measures were SSc and need for
rescue medication. Secondary outcome measures were changes in
The children used a face mask (Astratech No. 2; ASTRA, Denmark)
lung function and change in response to CACh and MCh during the
fitted with a flexible, noncompressible mouthpiece that supported the
cheeks and provided stable access to the airways via the mouth (11).
All variables from the diary cards were summarized for each pa-
Measurements were made during tidal breathing. Readings from
tient as a run-in mean and a treatment-period mean, after excluding
duplicate measurements made with each method were used as base-
the first 14 d of the treatment period. Total nighttime and daytime
line values before bronchial provocation tests. The sequence of mea-
asthma symptoms were summarized by first adding the scores for
surements was Rint, Xrs5, Rrs5, and sRaw. The same observer made
each subsymptom and then averaging the scores over the treatment
measurements at baseline and after bronchial provocation tests.
periods. Total 24-h asthma symptoms were summarized by adding the
The subjects did not have clinical respiratory symptoms on the
nighttime and daytime mean scores. Identical periods and data were
used for calculation of symptom-free days. sRaw. sRaw was measured in a constant-volume, whole-body
An asthma exacerbation was defined as at least two consecutive
plethysmograph as the relationship between simultaneous variations
24-h periods with symptoms of wheezing and the need for at least 3
in respiratory flow and maximum changes in plethysmographic pres-
puffs of rescue treatment. The exacerbation was considered ongoing
sure during inspiration and expiration (11). sRaw was calculated from
as long as the two conditions were fulfilled, although for computa-
the S-shaped resistance loops presented graphically by the computer
tional use, exacerbations experienced by a particular subject were
connected with the plethysmograph. Compensation for body temper-
separated by periods of 5 d from the last previous day of exacerbation.
ature, barometric pressure, and water vapor-saturated (BTPS) condi-
The means of duplicate measurements of sRaw, Rint, Xrs5, and
tions was done electronically (13). The respiratory rate was 30 to 45
Rrs5 defined the baseline at each visit. Effect on lung function after
breaths/min. When needed, an adult accompanied the subject during
treatment was calculated as the average lung function after 4 wk and 8 wk
testing (11, 13). The median value of five sequential measurements of
as a percent of lung function at baseline.
Predicted values based on height (in centimeters) for the lung
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
function variables were based on a previous study of healthy controls
withdrawn prior to randomization, 50 because their SSc did
(26). Response to CACh was quantified as the percent change from
not fulfil the criteria and two because of withdrawal of consent
baseline. Thus, the formula used in calculating the response to CACh
prompted by increasing symptoms after stopping of regular
was 100 ؒ (post-CACh value Ϫ baseline value)/(baseline value). The
treatment. One patient randomized into the study had asthma
result of the MCh challenge was expressed as PCx, the provocative
exacerbations during most of the treatment period due to lack
concentration producing a change of 50% in SRaw, 30% in Rint and
of compliance and was therefore withdrawn before analysis of
Rrs5, 80% in Xrs5, and 15% in TcO (25). PCx was found through lin-
ear interpolation on a logarithmic scale. If x% change was not found
the study data. Thirty-eight asthmatic children (22 boys and 16
after the last dose step, PCx was estimated by one-step linear extrapo-
girls; mean age 53 mo [range: 35 to 71 mo]), were analyzed as
lation, using the last two previous values. If x% change was found af-
an intention-to-treat population. Baseline characteristics (Ta-
ter the first dose step, PCx was estimated by linear interpolation on
ble 1), including height, atopic disposition, relevant allergy, ex-
the linear scale between 0 and the first MCh concentration used.
posure to passive smoking, SSc, use of rescue medication, and
Statistical considerations. An analysis of variance model was ap-
lung function were comparable in the treatment and placebo
plied to compare BUD and placebo, using run-in mean SSc and base-
groups. The mean (range) duration of a history of recurrent
line lung function values as covariates. Ninety-five percent confidence
asthma symptoms was 18 mo (range: 4 to 56 mo). Twenty-one
intervals (CIs) were constructed for the differences with and without
(55%) subjects had a first-degree relative with atopic disease,
treatment. When analyzing asthma SSc, sleep disturbance, use of res-cue medication, response to CA challenge, and change in lung func-
and 18 (47%) were exposed to passive smoking at home.
tion, we used additive models that gave arithmetic means. When ana-
Twenty-two (58%) subjects had other manifestations of atopy
lyzing lung function tests in measured units or PCx from the MCh
(atopic dermatitis and/or rhinitis). All 39 randomized subjects
challenge, we used multiplicative models giving geometric means,
were given skin prick tests or had assays of specific serum-IgE
which were used to calculate treatment differences as ratios. The dif-
antibody to the 10 inhalant allergens most common in Scandi-
ferent subsymptoms were analyzed with a multivariate analysis of vari-
navia, and 15 of the 39 (39%) had at least one positive test rel-
ance model, using each of the variables and baseline values as covari-
Until the start of the run-in period, 33 (87%) of the subjects
Asthma exacerbation rates were compared for treatment versus
were undergoing treatment with ICS, consisting of BUD at 100
placebo with Poisson’s distribution, assuming equal exacerbation rates
to 1,200 g/d (mean: 440 g/d) delivered via a metered-dose
for all patients within a treatment group. The numbers of patients ineach treatment group experiencing at least one asthma exacerbation
inhaler with a metal spacer (Nebuchamber), or fluticasone at
during the treatment period were compared through Fisher’s exact
50 to 250 g/d (mean: 133 g/d) delivered via a metered dose
inhaler with a plastic spacer (Babyhaler, GlaxoWellcome,
From experience with a previous study using the same diary cards
Brøndby, Denmark). Short acting 2-agonists delivered via a
(7), we estimated that a difference of 0.6 between the treatment and
metered dose inhaler and spacer device were given as rescue
placebo groups in total asthma SSc and score for use of rescue medi-
medication. Four subjects were not treated with ICS: two were
cation would be detected with 80% power with 22 patients in each
treated only with a short-acting 2-agonist as required, one
with a long-acting  -agonist as required, and one with sodium
All statistical tests were two sided, and values of p Ͻ 5% were con-
cromoglycate. The mean (range) duration of the run-in period,
between the cessation of ICS therapy and qualification for ran-domization into the study, was 27 d (range: 14 to 56 d). SSc and Rescue Medication Use Patients
A statistically significant difference between BUD and pla-
A total of 91 patients were recruited for the study, and 39 were
cebo was found for nighttime asthma symptoms (p ϭ 0.01),
randomized to treatment or placebo. Fifty-two patients were
and a tendency toward a difference was found for daytime
BASELINE CHARACTERISTICS, USE OF RESCUE MEDICATION* AND TOTAL SYMPTOM SCORE DURING RUN-IN, AND BASELINE LUNG FUNCTION IN BUDESONIDE AND PLACEBO GROUP AT RANDOMIZATION Definition of abbreviations: F ϭ female; M ϭ male; Rint ϭ resistance by the interrupter technique; Rrs5 ϭ airway resistance at 5 Hz by the
impulse oscillation technique; SRaw ϭ specific airway resistance; Xrs5 ϭ airway reactance at 5 Hz by the impulse oscillation technique.
Nielsen and Bisgaard: Budesonide in Young Asthmatic Children
which was significant (p ϭ 0.01). We found a total of 12 exacer-bations in the BUD group and 29 in the placebo group, givingexacerbation rates of 3.7/yr versus 9.3/yr for BUD and placebo,respectively (p ϭ 0.006). Nine of 19 (47%) subjects in the BUDgroup and 14 of 19 (74%) subjects in the placebo group (p ϭ0.18) experienced at least one asthma exacerbation. Lung Function Measurements
Baseline lung function measured as sRaw and Rint at the dayof randomization was 116% (95% CI: 106 to 126) and 119%(95% CI: 110 to 128), respectively, of the predicted lung func-tion values in relation to the height of the subjects (26) (i.e.,the subjects showed significantly increased airway resistanceat baseline) (Table 1). Baseline measurements of Xrs5 andRrs5 did not differ from the reference values.
Lung function was significantly improved with BUD (Table
2). The difference between BUD and placebo was reflected byRint (p ϭ 0.01), Rrs5 (p ϭ 0.01), and Xrs5 (p ϭ 0.001) at theendpoint after 8 wk of treatment, and by the average lungfunction through Visits 3 and 4. As shown in Table 2, Rint,Xrs5, and Rrs5 improved during active treatment and deterio-rated during administration of placebo. Xrs5 and Rrs5 re-flected this improvement by Visit 3. No treatment effect wasreflected by SRaw (p ϭ 0.35) (Table 2).
Responsiveness to CA challenge measured with each study
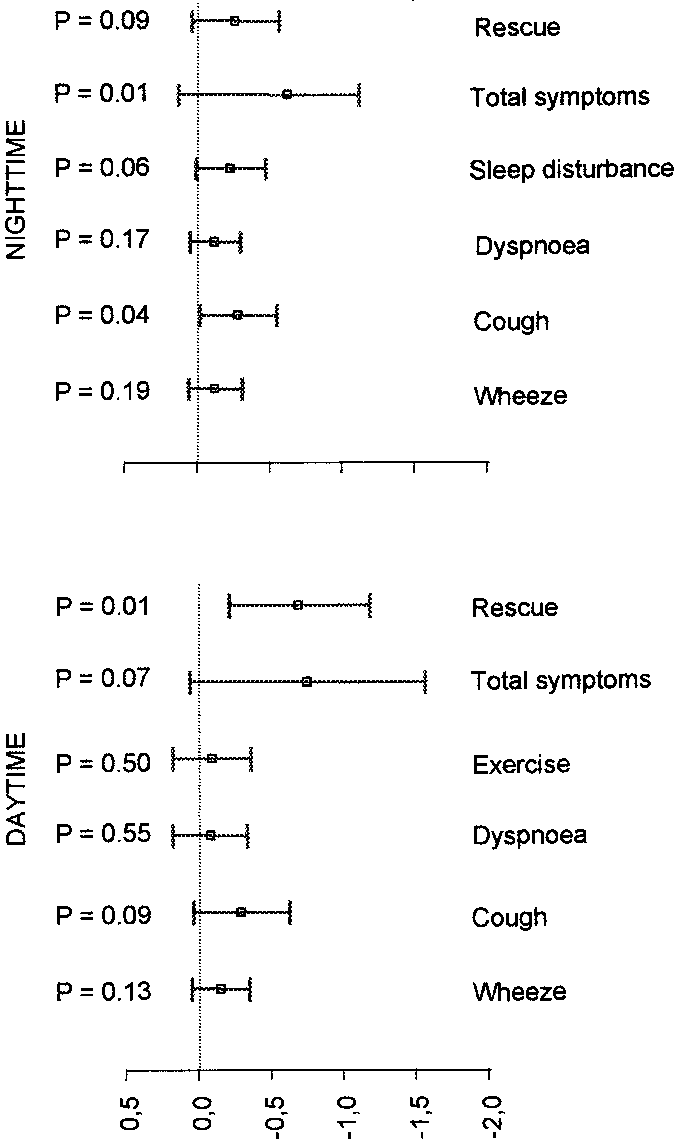
Figure 1. Effect on subsymptom scores, total symptom score, and day-
method at different visits is shown as the mean percentage
time and nighttime use of rescue medication of treatment with budes-
change from baseline (95% CI) in Figure 3. BUD significantly
onide in contrast to placebo. Adjusted mean (95% CI) differences
reduced responsiveness to CA challenge after 8 wk of treat-
(BUD–PLAC) between changes from run in period to completion of
ment. This was reflected in measurements of SRaw (p Ͻ 0.001),
budesonide treatment and placebo periods are shown.
Rint (p ϭ 0.01), Rrs5 (p ϭ 0.01), and Xrs5 (p ϭ 0.07). Figure 3shows the decrease in responsiveness in all parameters during
asthma symptoms (p ϭ 0.07) (Figure 1). The combined 24-h
BUD treatment and the reverse effect during placebo adminis-
SSc was significantly in favor of BUD (p ϭ 0.03).
tration. At the final CA challenge, 11 of 19 patients in the BUD
All subsymptom scores were reduced during treatment,
group, versus three of 19 subjects in the placebo group, reached
more so in the BUD than in the placebo group. Nighttime
normal responsiveness (defined as a change of
cough was significantly reduced with active treatment (p ϭ
subject [w]) (23) measured in terms of sRaw (p 0.02).
0.04). Borderline significance was found for a reduction in
Methacholine Challenge Response
daytime cough (p ϭ 0.09) and disturbance of parents’ sleep (p ϭ0.06) with treatment, but no other subsymptoms were signifi-
There was no statistically significant difference between BUD
and placebo in any of the parameters used in the study, al-
BUD significantly reduced daytime use of rescue medica-
though a trend in favor of BUD treatment was seen in SRaw
tion (p ϭ 0.01), but not its nighttime use (p ϭ 0.09) (Figure 1).
measurements (p 0.11). The provocative concentration of
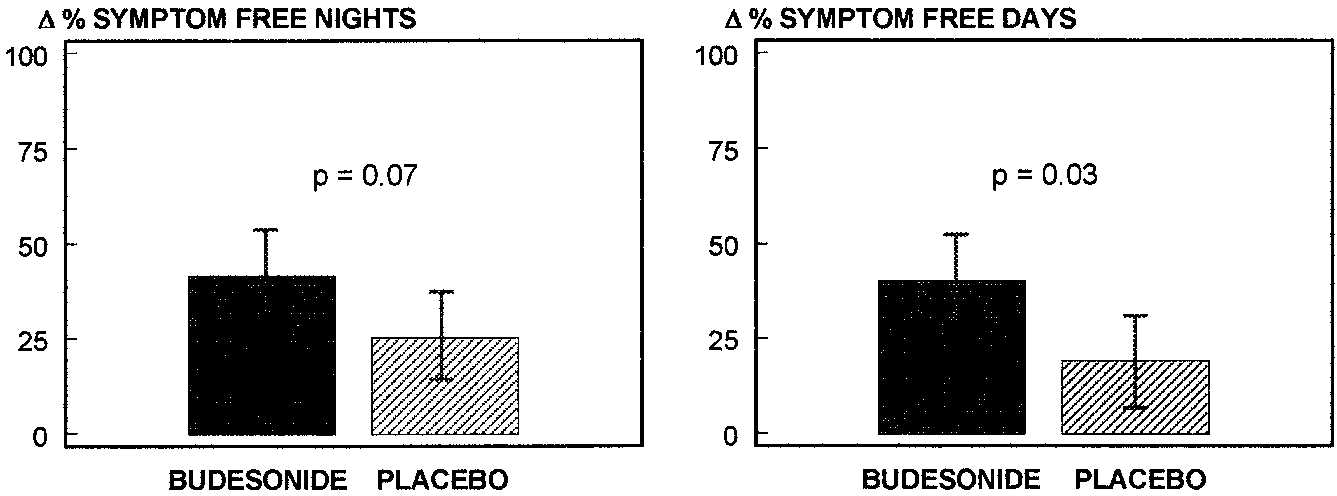
The change with BUD and the difference between BUD
MCh eliciting a 50% increase in SRaw could be computed by
and placebo in asthma-symptom–free days and nights are
interpolation for all curves except two. Considerably more of
shown in Figure 2. There was a significant difference in the
the PCx values for Rint, Xrs5, Rrs5, and TcO had to be esti-
change in percentage of symptom-free days (p ϭ 0.03) and to-
tal 24-h symptom-free periods (p ϭ 0.01), and a tendency to-
DISCUSSION
ward a difference in symptom-free nights (p ϭ 0.07).
The percentage of days with asthma exacerbations was
This is the first report of the efficacy of ICS in asthmatic chil-
4.9% in the BUD group versus 19.4% in the placebo group,
dren aged 2 to 5 yr to be based on objective measurements of
Figure 2. Increase in percentage of symptom-free nights and days after treatment with budesonide and placebo administration.
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
EFFECT ON LUNG FUNCTION OF TREATMENT WITH BUDESONIDE AND PLACEBO Definition of abbreviations: CI ϭ confidence interval; Rint ϭ resistance by the interrupter technique; Rrs ϭ airway resistance at 5 Hz by the impulse oscillation technique; sRaw ϭ
specific airway resistance; Xrs5 ϭ airway reactance at 5 Hz by the impulse oscillation technique.
Mean (95% CI) baseline values at randomization (0 wk), after 8 wk of treatment, and average (geometric mean, 95% CI) baseline lung function during treatment period (Total Pe-
lung function and bronchial responsiveness. The study was ex-
exacerbation rate, and use of rescue medication (2–8), and all
plorative, evaluating objective measures together with con-
have shown an effect of ICS against moderate to severe persis-
ventional measures of symptoms as primary outcomes of
tent asthma symptoms. However, none of these studies used
asthma disease activity. The effect of 400 g BUD twice daily,
any objective parameters in children under 6 yr old. In a study
delivered via a pMDI with a metal spacer device, was docu-
of infants aged 5 to 18 mo with recurrent wheezing (27), lung
mented by improvement in SSc, reduced consumption of res-
function as measured with the rapid thoracoabdominal com-
cue medication, reduced asthma exacerbation rates, and in-
pression technique, and bronchial responsiveness assessed
creased numbers of days and nights without symptoms, as
with histamine challenge, were used as objective measures in
found in previous studies (2–8). In addition to this expected
parallel with subjective measures. ICS was found to signifi-
treatment effect, the disease control with BUD was reflected
cantly improve bronchial responsiveness, but failed to show an
in measures of lung function and responsiveness to CACh.
effect on baseline lung function or SSc, possibly because of a
The design of the present study was biased by regression
toward the mean, since randomization took place immediately
Ninety-one patients, of whom 90% were receiving regular
after a period of significant symptom scoring. This was re-
inhaled steroid treatment, were screened for our study and
flected by the pronounced placebo effect, and the study results
stopped their steroid treatment during the run-in period.
should therefore be interpreted in the light of these unfavor-
Thirty-nine patients qualified for randomization. One reason
able odds, strengthening the conclusions of the study. Also,
for noneligibility may have been that some of the patients did
the small sample size of only 38 patients hampered the power
not have asthma. Alternatively, some would still have been
to uncover treatment differences in some subsymptoms, SRaw,
protected at 8 wk after treatment interruption, and some had
only mild asthma. Therefore, the final study group in the
Previous studies of effect of ICS on asthma in young chil-
present study consisted of asthmatic children carefully se-
dren have focused solely on subjective parameters such as SSc,
lected on the basis of a history of recurrent asthmatic epi-
Figure 3. Change (%) in measures of lung function (sRaw, Rint, Xrs5, and Rrs5) in response to CA chal- lenge at randomization (0 W) and after 8 wk of treat- ment with budesonide or placebo (8 W). Mean (95% CI).
Nielsen and Bisgaard: Budesonide in Young Asthmatic Children
sodes, need for current antiasthmatic therapy, and relapse of
by CA challenge is used to titrate the steroid dose may pro-
asthma symptoms during interruption of treatment. From the
vide an improvement in the long-term management of asthma
very high percentages of days (95%) and nights (78%) with
symptoms during the run-in period, it may be concluded that
MCh has been extensively studied in children, and with
these patients represented a group of children with moderate
success in children as young as 2 to 5 yr of age, showing satis-
to severe asthma. Their baseline lung function showed signifi-
factory repeatability (11, 12). However, this method is time
cantly increased airway resistance as compared with that of
consuming and probably does not reflect the pathophysiology
healthy controls (26), which is in agreement with our previous
of asthma to the same extent as does CACh (22). In the
findings in a random group of young asthmatic children (28)
present study we found no effect of BUD on responsiveness to
and in selected groups of young asthmatic children (23, 24).
MCh, in contrast to the effect found on CACh. Inadequate du-
The dose of BUD given in the study was 400 g twice daily,
ration of treatment may explain the lack of effect on MCh re-
which is above the pediatric dose range recommended as effi-
sponsiveness. Furthermore, it has been suggested that ICS
cacious in young children with moderate to severe persistent
may provide greater protection against constrictor stimuli that
asthma symptoms, and is probably on the flat part of the dose–
act indirectly, such as CA, than those that act directly, such as
response curve. The present study was explorative, and the
MCh. It has also been found that in asthmatic children, the air-
high dose of BUD was chosen with a view toward not over-
way reactivities induced by cold, dry air and methacholine
looking any possible effect on lung function and BHR. Impor-
challenge have no significant relationship (33).
tantly, despite the high dosage of BUD, it was not possible to
The present study found a concordant treatment response
eliminate asthma symptoms in all of the children in the study.
to BUD in both subjective parameters and objective parame-
Whole-body plethysmography (sRaw), the interrupter
ters such as lung function and bronchial responsiveness in
technique (Rint), and impulse oscillometry (Rrs5 and Xrs5)
young asthmatic children. This suggests that measurement of
are convenient methods for measuring lung function in young
these objective parameters could be implemented and applied
children (11). Furthermore, the CACh test as a provocative
in future studies of the clinical management of asthma in
stimulus and measurement of sRaw to quantify the bronchial
young children. Furthermore, a dose–response study of ICS
response can be used to disclose BHR in awake, young chil-
on symptoms, lung function, and BHR in a larger number of
dren, and to distinguish asthmatic and healthy children (23). In
the present study we demonstrated long-term improvement in
In conclusion, inhaled BUD at a total dose of 800 g daily
baseline lung function, attributed to treatment, as measured
significantly improved SSc, asthma exacerbation rates, lung
by the interrupter technique and impulse oscillation tech-
function, and BHR as assessed by CA challenge in young asth-
nique. Whole-body plethysmography seemed less sensitive in
detecting long-term changes in baseline lung function.
Hyperventilation with cold, dry air has been shown to be a
References
potent stimulus to bronchoconstriction in asthma, and has been
1. Martinez, F. D., A. L. Wright, L. M. Taussig, C. J. Holberg, and M. Ha-
applied in several studies both in adults and school children
lonen, W. J. Morgan. 1995. Asthma and wheezing in the first six years
(15–21). We used the single-step method for CA challenge,
of life. N. Engl. J. Med. 332:133–138.
since multistep protocols are more time consuming and iden-
2. Bisgaard, H., S. L. Munck, J. P. Nielsen, W. Petersen, and S. V. Ohlsson.
tify the same subjects as hyperresponsive (21, 22). The CA
1990. Inhaled budesonide for treatment of recurrent wheezing in early
challenge test is simple to perform and standardize even in
childhood. Lancet 336:649–651.
children as young as 2 yr of age, and imposes no discomfort on
3. Ilangovan, P., S. Pedersen, S. Godfrey, K. Nikander, N. Noviski, and
J. O. Warner. 1993. Treatment of severe steroid dependent preschool
the child (23). We recently reported a sensitivity of 68% and a
asthma with nebulised budesonide suspension. Arch. Dis. Child. 68:
specificity of 93% for measurement of SRaw and CA chal-
lenge testing in a group of 2- to 5-yr–old asthmatic children
4. Connett, G. J., C. Warde, E. Wooler, and W. Lenney. 1993. Use of bu-
and a group of healthy children (23).
desonide in severe asthmatics aged 1–3 years. Arch. Dis. Child. 69:
The present study is the first to demonstrate an effect of
BUD on the bronchial responsiveness to CA challenge associ-
5. de Blic, J., C. Delacourt, M. Le Bourgeois, B. Mahut, J. Ostinelli, C.
Caswell, and P. Scheinmann. 1996. Efficacy of nebulized budesonide
ated with improvement in symptom control in young children.
in treatment of severe infantile asthma: a double-blind study. J. Al-
Hyperventilation of cold, dry air is believed to cause airway
lergy Clin. Immunol. 98:14–20.
narrowing through the release of leukotrienes (24, 29) and
6. Baker, J. W., M. Mellon, J. Wald, M. Welch, M. Cruz-Rivera, and K.
other mediators, and the level of responsiveness is hypothe-
Walton-Bowen. 1999. A multiple-dosing, placebo-controlled study of
sized to reflect the degree of airway inflammation (22). We re-
budesonide inhalation suspension given once or twice daily for treat-
cently reported clinically relevant bronchoprotection against
ment of persistent asthma in young children and infants. Pediatrics103:414–421.
BHR provided by the leukotriene receptor antagonist mon-
7. Bisgaard, H., J. Gillies, M. Groenewald, and C. Maden. 1999. The effect
telukast as quantified by CA challenge and SRaw measure-
of inhaled fluticasone propionate in the treatment of young asthmatic
ments in young asthmatic children (24). Previous studies of
children: a dose comparison study. Am. J. Respir. Crit. Care Med. 160:
adults (30, 31) have shown an effect of ICS on bronchocon-
striction induced by cold, dry air. In the present study, respon-
8. Kemp, J. P., D. P. Skoner, S. J. Szefler, K. Walton-Bowen, M. Cruz-Riv-
siveness improved in the group receiving active medication
era , and J. A. Smith. 1999. Once-daily budesonide inhalation suspen-sion for the treatment of persistent asthma in infants and young chil-
and deteriorated in the placebo group, probably reflecting an
dren. Ann. Allergy Asthma Immunol. 83:231–239.
effect of BUD on the underlying inflammation during treat-
9. Sly, P., and C. F. Robertson. 1990. A review of pulmonary function test-
ment and loss of disease control when treatment was stopped.
ing in children. J. Asthma 27:137–147.
Four children showed little or no change in responsiveness
10. Kanengiser, S., and A. J. Dozor. 1994. Forced expiratory manoeuvres in
with BUD. All other children in the BUD group improved in
children aged 3 to 5 years. Pediatr. Pulmonol. 18:144–149.
11. Bisgaard, H., and B. Klug. 1995. Lung function measurement in awake
young children. Eur. Respir. J. 8:2067–2075.
The importance of tailoring the dose of inhaled steroids to
12. Klug, B., and H. Bisgaard. 1996. Measurement of lung function in awake
the degree of BHR was recently emphasized by Sont and co-
2–4-year-old asthmatic children during methacholine challenge and acute
workers (32). A treatment strategy in which BHR as reflected
asthma. Pediatr. Pulmonol. 21:290–300.
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
13. Klug, B., and H. Bisgaard. 1996. Measurement of the specific airway re-
triene receptor antagonist in 3–5 year old children. Am. J. Respir. Crit.
sistance by plethysmography in young children accompanied by an
adult. Eur. Respir. J. 10:1599–1605.
25. Klug, B., and H. Bisgaard. 1997. Repeatability of methacholine chal-
14. Warner, J. O., and C. K. Naspitz. 1998. Third international pediatric con-
lenges in 2- to 4-year-old children with asthma, using a new technique
sensus statement on the management of childhood asthma. Interna-
for quantitative delivery of aerosol. Pediatr. Pulmonol. 23:278–286.
tional Pediatric Asthma Consensus Group. Pediatr. Pulmonol. 25:1–17.
26. Klug, B., and H. Bisgaard. 1998. Specific airway resistance, interrupter
15. Deal, C. E., E. R. McFadden, R. H. Ingram, F. J. Breslin, and J. J. Jae-
resistance and respiratory impedance in healthy children aged 2–7
ger. 1980. Airway responsiveness to cold air and hyperpnea in normal
years. Pediatr. Pulmonol. 25:322–331.
subjects and in those with hay fever and asthma. Am. Rev. Respir. Dis.
27. Stick, S. M., P. R. Burton, J. B. Clough, M. Cox, P. N. LeSouëf, and P. D.
Sly. 1995. The effects of inhaled beclomethasone dipropionate on lung
16. McLaughlin, J., and A. J. Dozor. 1983. Cold air inhalation challenge in
function and histamine responsiveness in recurrently wheezy infants.
the diagnosis of asthma in children. Pediatrics 72:503–509. Arch. Dis. Child. 73:327–332.
17. Tal, A., H. Pasterkamp, C. Serrette, F. Leahy, and V. Chernick. 1984.
28. Klug, B., and H. Bisgaard. 1999. Lung function and short-term outcome
Response to cold air hyperventilation in normal and in asthmatic chil-
in young asthmatic children. Eur. Respir. J. 14:1185–1189.
dren. J. Pediatr. 104:516–521.
29. Fischer, A. R., M. A. Rosenberg, M. Roth, M. Loper, S. Jungerwirth,
18. Zach, M. S., G. Polgar, H. Kump, and P. Kroisel. 1984. Cold air chal-
and E. Israel. 1997. Effect of a novel 5-lipoxygenase activating protein
lenge of airway hyperreactivity in children: practical application and
inhibitor, BAYx 1005, on asthma induced by cold dry air. Thorax
theoretical aspects. Pediatr. Res. 18:469–478.
19. Zach, M. S., and G. Polgar. 1987. Cold air challenge of airway hyperreac-
30. Vathenen, A. S., A. J. Knox, A. Wiesniewski, and A. E. Tattersfield.
tivity in children: dose-response interrelation with a reaction plateau.
1991. Effect of inhaled budesonide on bronchial reactivity to hista-
J. Allergy Clin. Immunol. 80:9–17.
mine, exercise, and eucapnic dry air hyperventilation in patients with
20. Reisman, J., L. Mappa, F. de Benedictis, J. McLaughlin, and H. Levison.
1987. Cold air challenge in children with asthma. Pediatr. Pulmonol. 3:
31. Claussen, M., and V. Sill. 1993. Influence on non-specific bronchial hy-
perreactivity to cold air hyperventilation and carbachol by nedocromil
21. Modl, M., E. Eber, B. Steinbrugger, E. Weinhandl, and M. S. Zach. 1995.
and budesonide. Pneumologie. 47:209–214.
Comparing methods for assessing bronchial responsiveness in chil-
32. Sont, J. K., L. N. A. Willems, E. H. Bel, J. H. J. M. van Krieken, J. P.
dren: single step cold air challenge, multiple step cold air challenge,
Vandenbroucke, P. J. Sterk, and the AMPUL Study Group. 1999.
and histamine provocation. Eur. Respir. J. 8:1742–1747.
Clinical control and histopathological outcome of asthma when using
22. Zach, M. S. 1995. Cold dry air challenge for measuring bronchial respon-
airway hyperresponsiveness as additional guide to long-term treat-
siveness—where do we stand? Pediatr. Pulmonol. 19:323–325.
ment. Am. J. Respir. Crit. Care Med. 159:1043–1051.
23. Nielsen, K. G., and H. Bisgaard. 2000. Lung function response to cold air
33. de Benedictis, F. M., J. C. Canny, B. MacLusky, and H. Levison. 1995.
challenge in asthmatic and healthy children aged 2 to 5 years. Am. J.
Comparison of airway reactivity induced by cold air and methacholine
Respir. Crit. Care Med. 161:1805–1809.
challenges in asthmatic children. Pediatr. Pulmonol. 19:326–329.
24. Bisgaard, H., and K. G. Nielsen. 2000. Bronchoprotection from leuko-
(c) Graham P. Oxtoby 2007/2008 Journal of the British Herpetological Society 2008 THE OCCURRENCE OF PSITTACOSIS IN THE EMERALD TREE BOA ( CORALLUS CANINUS ) OF SOUTH AMERICA GRAHAM P. OXTOBY [Abstract] Corallus caninus – the emerald tree boa of South America – is renowned for the many difficulties it may present whilst kept in captivity. The problems which may o
Product Information A PRODUCT OF THE VALVOLINE COMPANY A DIVISION OF ASHLAND INC. Valvoline Dipperstick Valvoline Dipperstick Grease is very adhesive to metal surfaces, resists water washing and prevents rust and corrosion. The product possesses excellent wear-resisting properties and contains graphite which makes it suitable for working in damp, or even wet conditions. It with
 Nielsen and Bisgaard: Budesonide in Young Asthmatic Children
which was significant (p ϭ 0.01). We found a total of 12 exacer-bations in the BUD group and 29 in the placebo group, givingexacerbation rates of 3.7/yr versus 9.3/yr for BUD and placebo,respectively (p ϭ 0.006). Nine of 19 (47%) subjects in the BUDgroup and 14 of 19 (74%) subjects in the placebo group (p ϭ0.18) experienced at least one asthma exacerbation.
Nielsen and Bisgaard: Budesonide in Young Asthmatic Children
which was significant (p ϭ 0.01). We found a total of 12 exacer-bations in the BUD group and 29 in the placebo group, givingexacerbation rates of 3.7/yr versus 9.3/yr for BUD and placebo,respectively (p ϭ 0.006). Nine of 19 (47%) subjects in the BUDgroup and 14 of 19 (74%) subjects in the placebo group (p ϭ0.18) experienced at least one asthma exacerbation.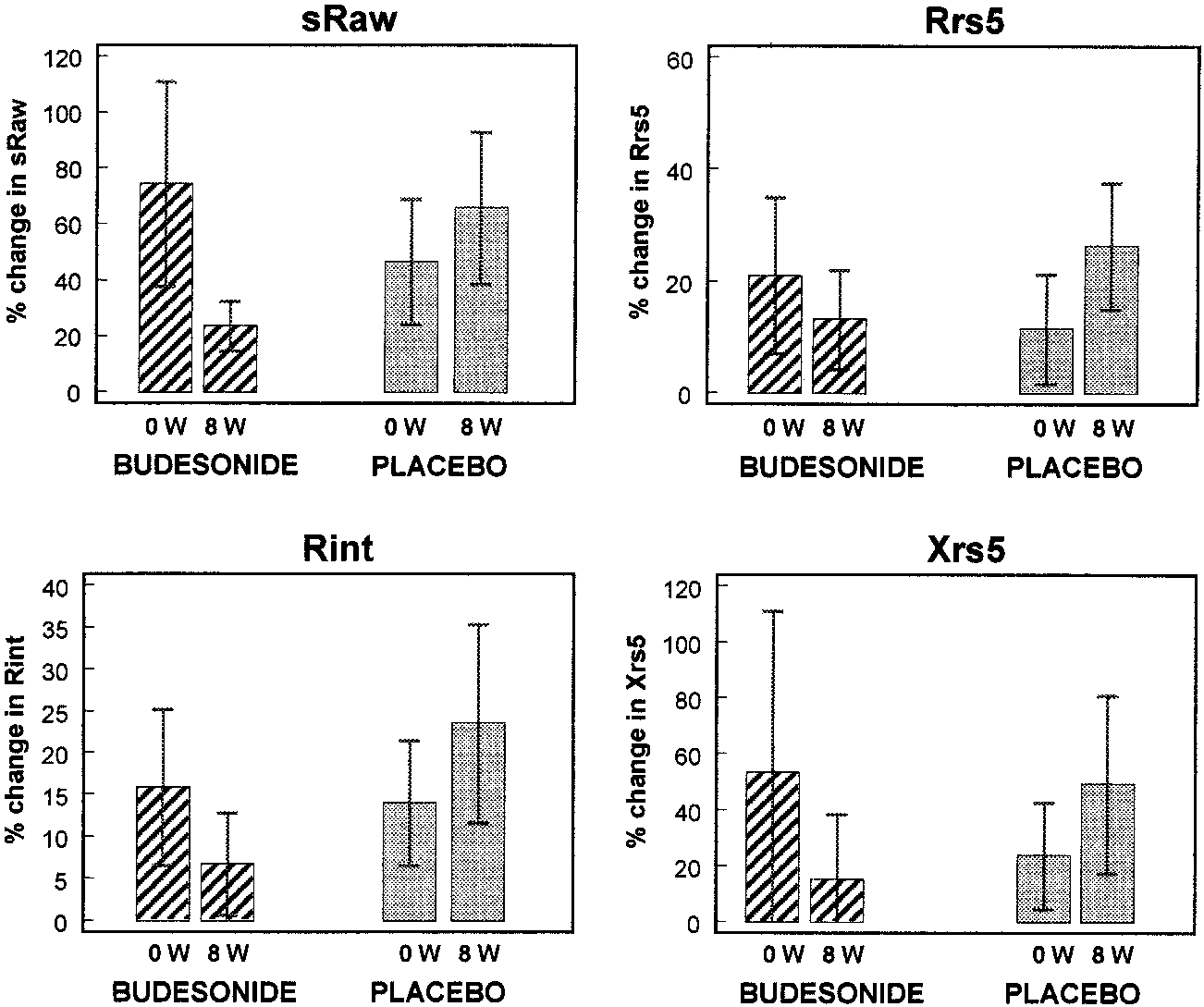 AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
EFFECT ON LUNG FUNCTION OF TREATMENT WITH BUDESONIDE AND PLACEBO
AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
EFFECT ON LUNG FUNCTION OF TREATMENT WITH BUDESONIDE AND PLACEBO