Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
The thyroid nodule
The new england journal of medicine
This Journal feature begins with a case vignette highlighting a common clinical problem. Evidence supporting various strategies is then presented, followed by a review of formal guidelines, when they exist. The article ends with the author’s clinical recommendations.A 42-year-old woman presents with a palpable mass on the left side of her neck. She has no neck pain and no symptoms of thyroid dysfunction. Physical examination re- veals a solitary, mobile thyroid nodule, 2 cm by 3 cm, without lymphadenopathy. The patient has no family history of thyroid disease and no history of external irradiation. Which investigations should be performed? Assuming that the nodule is benign, which, if any, treatment should be recommended?
In the United States, 4 to 7 percent of the adult population have a palpable thyroid nod-
ule.1 However, only 1 of 20 clinically identified nodules is malignant. This corresponds
pital, Odense, Denmark. Address reprintrequests to Dr. Hegedüs at the Depart-
to approximately 2 to 4 per 100,000 people per year, constituting only 1 percent of all
cancers and 0.5 percent of all cancer deaths.2 Nodules are more common in women
and increase in frequency with age and with decreasing iodine intake. The prevalence
Odense, Denmark, or at laszlo.hegedus@ouh.fyns-amt.dk.
is much greater with the inclusion of nodules that are detected by ultrasonography or atautopsy. By the latter assessment, approximately 50 percent of 60-year-old persons
Copyright 2004 Massachusetts Medical Society.
The clinical spectrum ranges from the incidental, asymptomatic, small, solitary
nodule, in which the exclusion of cancer is the major concern, to the large, partly in-trathoracic nodule that causes pressure symptoms, for which treatment is warrantedregardless of cause.3 The most common diagnoses and their approximate distribu-tions are colloid nodules, cysts, and thyroiditis (in 80 percent of cases); benign follicu-lar neoplasms (in 10 to 15 percent); and thyroid carcinoma (in 5 percent).
The management of a solitary thyroid nodule remains controversial.3-5 This review
will focus on the management of a solitary thyroid nodule that is detected on physicalexamination, regardless of the finding of additional nodules by radionuclide scanningor ultrasonography, since such a finding does not alter the risk of cancer.3
s t r a t e g i e s a n d e v i d e n c e
h i s t o r y a n d p h y s i c a l e x a m i n a t i o n
The history and physical examination remain the diagnostic cornerstones in evaluatingthe patient with a thyroid nodule and may be suggestive of thyroid carcinoma (Table 1). However, a minority of patients with malignant nodules have suggestive findings, whichoften also occur in patients with benign thyroid disorders. There is also substantialvariation among practitioners in evaluating nodules,2,6 a finding that may explain whyan increasing number of thyroid specialists use imaging as part of the evaluation.4,5
The risk of thyroid cancer seems nearly as high in incidental nodules (<10 mm), the
majority of which escape detection by palpation, as in larger nodules.7 However, thevast majority of these microcarcinomas do not grow during long-term follow-up and
The New England Journal of Medicine as published by New England Journal of Medicine.
Downloaded from www.nejm.org on August 2, 2010. For personal use only. No other uses without permission.
Copyright 2004 Massachusetts Medical Society. All rights reserved.
do not cause clinically significant thyroid cancer.8The fact that ultrasonography detects nodules
Table 1. Clinical Findings Suggesting the Diagnosis of Thyroid Carcinoma in a Euthyroid Patient with a Solitary Nodule, According to the Degree
(a third of which are more than 20 mm in diame-
of Suspicion.
ter) in up to 50 percent of patients with a normalneck examination underscores the low specificity
High suspicion
and sensitivity of clinical examination.9 When two
Family history of medullary thyroid carcinoma or multiple endocrine neoplasiaRapid tumor growth, especially during levothyroxine therapy
or more risk factors that indicate a high clinical
suspicion are present, the likelihood of cancer ap-
Fixation of the nodule to adjacent structures
proaches 100 percent.10 In such cases, biopsy is
still useful to guide the type of surgery1,2 (Fig. 1).
Regional lymphadenopathyDistant metastases
l a b o r a t o r y i n v e s t i g a t i o n s Moderate suspicion
Because clinical examination is not sensitive for
Age of either <20 years or >70 years
identifying thyroid dysfunction,6 laboratory evalu-
ation of thyroid function is routinely warranted.
The only biochemical test routinely needed is mea-
A nodule >4 cm in diameter or partially cystic
surement of the serum thyrotropin level. If this level
Symptoms of compression, including dysphagia, dysphonia, hoarseness,
is subnormal, levels of free thyroxine or free triiodo-thyronine should be measured to document thepresence and degree of hyperthyroidism. Approxi-mately 10 percent of patients with a solitary nodule nearly always benign, whereas a nonfunctioninghave a suppressed level of serum thyrotropin, which nodule, constituting approximately 90 percent ofsuggests a benign hyperfunctioning nodule.2 If the nodules, has a 5 percent risk of being malignant. serum thyrotropin concentration is elevated, a se- Thus, in the patient with a suppressed level of serumrum antithyroperoxidase antibody level should be thyrotropin, radionuclide confirmation of a func-obtained to confirm Hashimoto’s thyroiditis. How- tioning nodule may obviate the need for biopsy. ever, the finding of an elevated level does not obvi- A scan can also indicate whether a clinically solitaryate the need for a fine-needle aspiration biopsy, nodule is a dominant nodule in an otherwise multi-since the practitioner must rule out a coexisting nodular gland and can reveal substernal extensioncancer, including lymphoma, which accounts for of the thyroid. A scan can be performed with io-only 5 percent of thyroid cancers but is associated dine-123, iodine-131, or technetium-99m–labeledwith Hashimoto’s thyroiditis.11 Nearly all patients pertechnetate. Iodine isotopes, which are bothwith thyroid cancer are euthyroid.1
trapped and bound organically in the thyroid, are
If a patient has a family history of medullary thy- preferred, since 3 to 8 percent of nodules that ap-
roid cancer or multiple endocrine neoplasia type 2, pear functioning on pertechnetate scanning maya basal serum calcitonin level should be obtained; appear nonfunctioning on radioiodine scanning,an elevated level suggests medullary thyroid can- and a few of those nodules may be thyroid can-cer. Before surgery is performed, investigation for cers.13 A scan cannot be used to measure the size ofprimary hyperparathyroidism and pheochromocy- a nodule accurately. toma should be carried out. Serum calcitonin is notroutinely measured in patients who have no sug- Ultrasonographygestive family history, since medullary carcinoma Ultrasonography can accurately detect nonpalpa-is present in only about 1 of 250 patients with a thy- ble nodules, estimate the size of the nodule and theroid nodule.12
volume of the goiter, and differentiate simple cysts,which have a low risk of being malignant, from
i m a g i n g o f t h e t h y r o i d n o d u l e
solid nodules or from mixed cystic and solid nod-
ules, which have a 5 percent risk of being malig-
Radionuclide scanning, which is performed much nant (Fig. 3). Ultrasonography also provides guid-more commonly in Europe than in the United ance for diagnostic procedures (e.g., fine-needleStates,3-5 may be used to identify whether a nodule aspiration biopsy) as well as therapeutic proceduresis functioning (Fig. 2). A functioning nodule, with (e.g., cyst aspiration, ethanol injection, or laseror without suppression of extranodular uptake, is therapy) and facilitates the monitoring of the ef-
The New England Journal of Medicine as published by New England Journal of Medicine.
Downloaded from www.nejm.org on August 2, 2010. For personal use only. No other uses without permission.
Copyright 2004 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
levothyroxine therapy,ethanol injection, and
Figure 1. Algorithm for the Cost-Effective Evaluation and Treatment of a Clinically Detectable Solitary Thyroid Nodule.
In the case of a strong clinical suspicion of cancer, surgery is recommended, regardless of the results of fine-needle aspiration biopsy (FNAB). In the case of a suppressed level of serum thyrotropin, thyroid scintigraphy should be performed, since a functioning nodule almost invariably rules out cancer. In the case of a nondiagnostic FNAB, a repeated biopsy yields a satisfactory aspirate in 50 percent of cases. If ultrasonogra-phy reveals additional nodules that are more than 10 mm in diameter, FNAB could be performed on one other nodule, in addition to the one that is clinically detectable. The therapeutic options shown cover both solid and cystic nodules. In the case of a recurrent cyst, the possibilities of treatment are repeated FNAB, surgery, and ethanol injection. I do not recommend levothyroxine therapy for the thyroid nodule.
The New England Journal of Medicine as published by New England Journal of Medicine.
Downloaded from www.nejm.org on August 2, 2010. For personal use only. No other uses without permission.
Copyright 2004 Massachusetts Medical Society. All rights reserved.
Figure 2. Scintigram of a Solitary Functioning Nodule in the Right Thyroid Lobe.
Scintigraphy that was performed with the use of techne-tium-99m–labeled pertechnetate shows suppression of extranodular uptake in thyroid tissue. Figure 3. Cross-Sectional Ultrasonogram Showing a Solid, Hypoechoic Nodule (Dark Gray) in the Right Thyroid Lobe.
fects of treatment.9 In one study, among patients who had been referred for evaluation of a palpable thyroid abnormality, ultrasonography altered the guishing benign from malignant nodules, but its clinical management in two thirds of cases,14 use is limited by cost and accessibility16 and it can- mainly by identifying nodules that were smaller not replace biopsy. than 1 cm (which were not considered to require further evaluation) in 20 percent of the patients and fine-needle aspiration biopsy by discovering additional nodules (which required Independent of morphology, fine-needle aspiration biopsy) in 24 percent of the patients. Characteris- provides the most direct and specific information tics revealed by ultrasonography — such as hypo- about a thyroid nodule. It is performed on an outpa- echogenicity, microcalcifications, irregular mar- tient basis,1,4,5 is relatively inexpensive, and is easy gins, increased nodular flow visualized by Doppler, to learn. Complications are rare and primarily in- and, especially, the evidence of invasion or regional volve local discomfort. The use of anticoagulants or lymphadenopathy — are associated with an in- salicylates does not preclude biopsy. In centers with creased risk of cancer; however, sonographic find- experience in fine-needle aspiration, the use of this ings cannot reliably distinguish between benign technique has been estimated to reduce the number and cancerous lesions.9
of thyroidectomies by approximately 50 percent, toroughly double the surgical confirmation of carci-
noma, and to reduce the overall cost of medical care
Computed tomography (CT) and magnetic reso- by 25 percent,17 as compared with surgery per-nance imaging also cannot reliably differentiate be- formed on the basis of clinical findings alone. tween malignant and benign nodules. These tests
Fine-needle aspiration has diagnostically useful
are rarely indicated in the evaluation of a nodule. An results in about 80 percent of cases,18 typically withexception is in the diagnosis and evaluation of sub- two to four passes of the needle. The number ofsternal goiters, since these imaging techniques can cases in which sufficient samples are obtained in-assess the extent of the goiter more precisely than creases if aspiration is guided by ultrasonography,can other techniques and can evaluate tracheal com- especially in nodules that are partly cystic, and re-pression.3,15 Evaluation of glucose metabolism by peated biopsy reduces by half the rate of insufficientpositron-emission tomography using fludeoxyglu- samples (to about 10 percent).19,20 The diagnosticcose (fluorodeoxyglucose) F 18 may help in distin- accuracy of fine-needle aspiration depends on the
The New England Journal of Medicine as published by New England Journal of Medicine.
Downloaded from www.nejm.org on August 2, 2010. For personal use only. No other uses without permission.
Copyright 2004 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
way in which suspicious lesions are handled. View- levothyroxine-treated patients than in patients whoing them as “positive” increases sensitivity (rate of had no treatment. 27 The likelihood of such shrink-false negative results, 1 percent), but decreases spec- age is greater when serum thyrotropin is suppressedificity.21 If fine-needle aspiration reveals a follicular to a level below 0.1 mU per liter than it is when theneoplasm (which occurs in approximately 15 per- level is below 0.3 mU.27-29 In a five-year, random-cent of nodules, of which only 20 percent turn out ized trial, suppression to below 0.1 mU per literto be malignant), radionuclide scanning should be significantly reduced the frequency with which newperformed.1-3 If such scanning shows a function- nodules developed (i.e., 8 percent of patients whoing nodule with or without complete suppression were treated with levothyroxine as compared withof the rest of the thyroid, surgery can be avoided, 29 percent of untreated patients).29 However, ther-since the risk of cancer is negligible.17 In a cystic le- apy with levothyroxine to reduce thyrotropin levelssion or one that is a mixture of cystic and solid below 0.1 mU per liter is associated with an in-components, fine-needle aspiration of a possible creased risk of atrial fibrillation, other cardiac ab-solid component should be performed, since the normalities,30,31 and reduced bone density.32 Re-risk of cancer is the same as that for a solid nonfunc- growth of nodules occurs after cessation of therapy. tioning nodule.2,20,21 With the exception of calci- Levothyroxine has no effect on the recurrence oftonin immunostaining for medullary carcinoma, thyroid cysts after aspiration.33there are no reliable immunohistologic or molec-ular tests for distinguishing between benign and Surgerymalignant nodules.3
The main indications for surgery are clinical or cy-tologic features suggestive of cancer or symptoms
t r e a t m e n t o f t h e s o l i t a r y t h y r o i d n o d u l e
The natural history of solitary thyroid nodules is ogy suggests a benign lesion, hemithyroidectomypoorly understood, mainly because nodules that are is generally preferred.4,5,18 Postoperative adminis-suspicious for cancer, cause pressure, or prompt tration of levothyroxine is indicated only in cases ofreports of cosmetic problems are rarely left un- hypothyroidism.34 When surgery is performed by atreated. With this reservation, it seems that the ma- specialist, the incidence of complications is lowjority of benign nonfunctioning nodules grow, par- (i.e., postoperative hypoparathyroidism in 1 per-ticularly those that are solid.22-24 In one study, 89 cent of cases and injuries to the recurrent laryngealpercent of nodules that were followed for five years nerve in about 1 percent), but the complication rateincreased by 15 percent or more in volume.24 The is higher for less experienced surgeons and thoseannual rate of evolution of a solitary functioning without special training.35nodule into a hyperfunctioning nodule is as high as6 percent; the risk is positively related to the size of Radioiodinethe nodule and negatively related to the serum thy- Radioiodine is an option for treatment of a func-rotropin level.25,26 There is controversy as to wheth- tioning nodule, with or without biochemical hyper-er a solitary nodule should be treated and, if so, thyroidism. It is contraindicated in pregnant andhow.4,5 Table 2 summarizes the advantages and breast-feeding women. Normalization of the resultsdisadvantages of potential treatment options. Fig- of thyroid radionuclide scanning and the serumure 1 shows a management algorithm.
thyrotropin level (often referred to as a “cure”) isachieved in 75 percent of patients, and thyroid vol-
ume is reduced an average of 40 percent, after a
Treatment with levothyroxine at a dose sufficient to single dose of iodine-131 aiming at a level of 100keep the serum thyrotropin at a level below 0.3 mU Gy, independent of pretreatment thyroid func-per liter has been suggested as a way to prevent tion.36,37 The main side effect is hypothyroidism,growth of an apparently benign nodule. However, which occurs in approximately 10 percent of pa-this approach has clear limitations. A recent meta- tients within five years after treatment and increas-analysis showed no significant difference in the size es in frequency over time. This risk is unrelated toof nodules after 6 to 12 months of suppressive ther- dose but is greater in patients with thyroid peroxi-apy with levothyroxine, as compared with no treat- dase antibodies and with iodine uptake in extra-ment, although the size of the nodules decreased nodular thyroid tissue.36,37 Most nodules do not dis-by more than 50 percent in a larger proportion of appear after radioiodine therapy but may become
The New England Journal of Medicine as published by New England Journal of Medicine.
Downloaded from www.nejm.org on August 2, 2010. For personal use only. No other uses without permission.
Copyright 2004 Massachusetts Medical Society. All rights reserved.
Table 2. Treatment of the Single Nonmalignant Thyroid Nodule. Treatment Type Advantages Disadvantages
Nodule ablation, complete relief of symptoms,
Need for hospitalization, high cost, risks associated with surgery,
vocal-cord paralysis (approximately 1% of patients), hypoparathy-roidism (<1%), hypothyroidism (approximately 1%*)
No need for hospitalization, low cost, may slow
Low efficacy, need for lifelong treatment, regrowth of nodule after ces-
sation of treatment, cardiac tachyarrhythmias, reduced bone den-
sity, not feasible when thyrotropin level is suppressed
No need for hospitalization, low cost, few sub-
Use of contraceptives needed in fertile women, only gradual reduction
jective side effects, nodule reduced by 40%
of the nodule, hypothyroidism within 5 yr (10% of patients), risk of
No need for hospitalization, relatively low cost,
Limited experience with treatment, decreasing efficacy with increasing
no hypothyroidism, nodule reduced by 45%
nodule size, success dependent on operator’s skill, painful (reduc-
ing compliance), risk of thyrotoxicosis and vocal-cord paralysis (approximately 1–2%), seepage of ethanol,‡ interpretation of cyto-logic and histologic findings impeded in treated nodules
* This risk applies only to the case of hemithyroidectomy. † This treatment is used only for the functioning thyroid nodule. ‡ Side effects due to the seepage of ethanol outside the nodule, which are rare (occurring in about 1 percent of patients), comprise nerve dam-
age, perinodular or periglandular fibrosis jeopardizing subsequent surgery, thrombosis of the jugular vein, and neck hematomas.
§ Laser therapy is still experimental, and experience with it is limited. The advantages are the same as those of ethanol injection, but side effects
are probably more limited because the higher degree of control with laser therapy limits the risk of extranodular damage.
harder on palpation and may reveal unusual cyto- cally benign, a single ethanol injection has beenlogic features as a result of irradiation. Thyroid shown to reduce the volume of nodules by approx-function should be checked regularly during the imately 50 percent.3,23 Additional ethanol injectionsfirst year and yearly thereafter in order to detect hy- have only a limited effect.41,42 Recently, data frompothyroidism. Nodules are unlikely to grow after a preliminary study suggested that the use of laserradioiodine therapy, but if growth occurs, a biopsy photocoagulation may be as effective as ethanol in-may be warranted.
jection, with fewer adverse effects.43 However, con-trolled trials are needed.
In thyroid cysts, the recurrence rate after aspira-
A number of studies have suggested a benefit of ul- tion is high. Tetracycline, a sclerosing agent, had notrasonographically guided ethanol injection in the effect in a randomized study.44 Uncontrolled stud-treatment of benign functioning and nonfunction- ies have suggested that ethanol injection may pre-ing solid thyroid nodules as well as cystic nod- vent the recurrence of cysts.39,40 A recent random-ules.38-40 The mechanism of effect involves coagu- ized, double-blind study45 involving a six-monthlative necrosis and small-vessel thrombosis. The follow-up period reported that 21 of 33 patientsprocedure requires prior documentation of benign (64 percent) who were treated with ethanol werecytology, skill, and experience3,9; drawbacks in- cured after one session, as compared with 6 of 33clude local pain and a potential risk of serious side patients (18 percent) who were treated with saline. effects (Table 2). There are few data from con-trolled trials to support this approach.
Available data suggest that multiple injections
of ethanol (a median of four) can achieve a complete There are no data from studies comparing the out-cure (i.e., a normalization of results of radionuclide come and cost-effectiveness of various strategies ofscanning and serum thyrotropin measures) in two evaluating a nodule (e.g., using radionuclide imag-thirds of patients with hyperfunctioning nodules ing and ultrasonographic guidance for fine-needleand three quarters of patients with functioning aspiration). There are also insufficient data compar-nodules without hyperthyroidism.38,39 In solid non- ing the outcome (including quality of life) of variousfunctioning nodules that are solitary and cytologi- management approaches in the absence of cancer.
The New England Journal of Medicine as published by New England Journal of Medicine.
Downloaded from www.nejm.org on August 2, 2010. For personal use only. No other uses without permission.
Copyright 2004 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
p r o f e s s i o n a l s o c i e t i e s
Clinical-practice guidelines were published in For the patient who presents with a nodule, as in1996 by the American Thyroid Association1 (www. the case described in the vignette, the main con-thyroid.org/professionals/publications/guidelines.
cern is to exclude the possibility of thyroid cancer,
html) and the American Association of Clinical even though the vast majority of nodules are be-Endocrinologists46 (www.aace.com/clin/guidelines/ nign (Fig. 1). The initial evaluation should includethyroid_nodules.pdf ). The recommendations of measurement of the serum thyrotropin level and aboth organizations correspond with those provid- fine-needle aspiration, preferably guided by ultra-ed here. Radionuclide scanning is not routinely rec- sonography. If the patient has a family history ofommended, but it is advocated in the case of a sup- medullary thyroid carcinoma or multiple endo-pressed level of serum thyrotropin or the finding of crine neoplasia type 2, the serum calcitonin levelfollicular neoplasia with the use of fine-needle as- should also be checked. If the thyrotropin level ispiration. Thyroid ultrasonography is recommend- suppressed, radionuclide scanning should be per-ed to guide fine-needle aspiration, especially in formed. In patients less than 20 years old, and innodules that are small and incidental or are partly the case of a high clinical suspicion for cancer (e.g.,cystic or from which primary fine-needle aspiration follicular neoplasia as diagnosed by fine-needle as-has yielded insufficient material. Fine-needle biop- piration and a nonfunctioning nodule revealed onsy of all possibly malignant nodules (which are not scanning), the patient should be offered hemithy-defined in the guidelines) is advocated. If the cytol- roidectomy regardless of the results of fine-needleogy is benign, repeated biopsy is seldom indicated. aspiration.
In the case of a benign nodule, periodic lifelong
In the case of a functioning benign nodule,
follow-up every 6 to 24 months (including mea- iodine-131 is generally the therapy of choice, in-surement of serum thyrotropin levels, neck palpa- dependent of concomitant hyperthyroidism. Fortion, and fine-needle aspiration in case of growth nonfunctioning cystic nodules, aspiration and eth-or other suspicious signs) is recommended. For a anol injection therapy may be considered, and etha-functioning benign nodule, iodine-131 is consid- nol injection or laser therapy if the nodules are solid,ered the treatment of choice, with surgery as an al- but data to support the use of these therapies areternative, especially if the nodule is very large or limited. My usual approach after documenting be-partly cystic or if the patient is young; treatment is nign cytology is to follow the patient yearly withmore strongly recommended if the serum thyro- neck palpation and measurement of the serum thy-tropin level is decreased or overt hyperthyroidism rotropin level, with repeated ultrasonography andis present, because of adverse effects on bone and fine-needle aspiration if there is evidence of growththe cardiovascular system. For a nonfunctional be- of the nodule. I do not recommend levothyroxinenign nodule, there is no clear recommendation on therapy to shrink or prevent growth of benign nod-the use of levothyroxine, although this therapy is ules because of the drug’s low efficacy and poten-considered contraindicated when the serum thyro- tial side effects. tropin level is suppressed, in patients more than
Dr. Hegedüs reports having received grants from the Agnes and
60 years old, and in postmenopausal women. If le- Knut Mørk Foundation, the Novo Nordisk Foundation, and the A.P.
vothyroxine therapy is used, regular reassessment
I am indebted to Dr. Steen J. Bonnema and Dr. Finn N. Benned-
(the interval is not defined in the guidelines) is bæk for their helpful comments. recommended, with monitoring of serum thyro-tropin levels, which should be subnormal butmeasurable. The guidelines do not address etha-nol injection and laser therapy. r e f e r e n c e s
Bennedbæk FN, Perrild H, Hegedüs L.
al. Treatment guidelines for patients with
Diagnosis and treatment of the solitary thy-
thyroid nodules and well-differentiated thy-
Hegedüs L, Bonnema SJ, Bennedbæk FN.
roid nodule: results of a European survey.
Management of simple nodular goiter: cur-
Clin Endocrinol (Oxf ) 1999;50:357-63.
rent status and future perspectives. Endocr
ment of the solitary thyroid nodule: results
The New England Journal of Medicine as published by New England Journal of Medicine.
Downloaded from www.nejm.org on August 2, 2010. For personal use only. No other uses without permission.
Copyright 2004 Massachusetts Medical Society. All rights reserved.
racy of conventional vs. sonography-guided
routine thyroxine treatment to hinder post-
fine-needle aspiration biopsy of thyroid nod-
operative recurrence of nontoxic goiter jus-
tified? J Clin Endocrinol Metab 1999;84:756-
ling SG, Hansen JM. Observer variation in
20. Gharib H, Goellner JR. Fine-needle aspi-
the clinical and laboratory evaluation of
ration biopsy of the thyroid: an appraisal. 35. Songun I, Kievit J, Wobbes T, Peerde-
patients with thyroid dysfunction and goi-
man A, van de Velde CJ. Extent of thyroidec-
21. Hamburger JI. Diagnosis of thyroid nod-
tomy in nodular thyroid disease. Eur J Surg
Papini E, Guglielmi R, Bianchini A, et al.
ules by fine needle biopsy: use and abuse.
Risk of malignancy in nonpalpable thyroid
J Clin Endocrinol Metab 1994;79:335-9. 36. Ferrari C, Reschini E, Paracchi A. Treat-
nodules: predictive value of ultrasound and
22. Kuma K, Matsuzuka F, Kobayashi A, et
color-Doppler features. J Clin Endocrinol
al. Outcome of long standing solitary thy-
a review. Eur J Endocrinol 1996;135:383-90.
roid nodules. World J Surg 1992;16:583-7. 37. Nygaard B, Hegedüs L, Nielsen KG,
Ito Y, Uruno T, Nakano K, et al. An obser-
23. Bennedbæk FN, Nielsen LK, Hegedüs L.
Ulriksen P, Hansen JM. Long-term effect of
vation trial without surgical treatment in
Effect of percutaneous ethanol injection ther-
radioactive iodine on thyroid function and
patients with papillary microcarcinoma of
apy vs. suppressive doses of L-thyroxine on
size in patients with solitary autonomously
benign solitary solid cold thyroid nodules: a
functioning toxic thyroid nodules. Clin Endo-
randomised trial. J Clin Endocrinol Metab
38. Lippi F, Ferrari C, Manetti L, et al. Treat- 24. Alexander EK, Hurwitz S, Heering JP, et 10. Hamming JF, Goslings BM, van Steenis
al. Natural history of benign solid and cystic
thyroid nodules. Ann Intern Med 2003;138:
results of an Italian multicenter study. J Clin
van de Velde CJ. The value of fine-needle
aspiration biopsy in patients with nodular
25. Hamburger JI. Evolution of toxicity in 39. Bennedbæk FN, Karstrup S, Hegedüs L.
thyroid disease divided into groups of suspi-
solitary nontoxic autonomously functioning
Percutaneous ethanol injection therapy in
the treatment of thyroid and parathyroid dis-
grounds. Arch Intern Med 1990;150:113-6.
eases. Eur J Endocrinol 1997;136:240-50.
[Erratum, Arch Intern Med 1990;150:1088.]
26. Sandrock D, Olbricht T, Emrich D, Ben- 40. Verde G, Papini E, Pacella CM, et al. 11. Pasieka JL. Hashimoto’s disease and thy-
ker G, Reinwein D. Long-term follow-up in
roid lymphoma: role of the surgeon. World
patients with autonomous thyroid adenoma.
injection in the treatment of cystic thyroid
Acta Endocrinol (Copenh) 1993;128:51-5. 12. Elisei R, Bottici V, Luchetti F, et al. Impact 27. Castro MR, Caraballo PJ, Morris JC.
of routine measurement of serum calcitonin
Effectiveness of thyroid hormone suppres-
41. Bennedbæk FN, Hegedüs L. Percutane-
on the diagnosis and the outcome of medul-
sive therapy in benign solitary thyroid nod-
ous ethanol injection therapy in benign soli-
lary thyroid cancer: experience in 10,864
ules: a meta-analysis. J Clin Endocrinol Metab
tary solid cold thyroid nodules: a random-
patients with nodular thyroid disorders. J Clin
ised trial comparing one injection with three
28. Zelmanovitz F, Genro S, Gross JL. Sup- 13. Shambaugh GE III, Quinn JL, Oyasu R, 42. Zingrillo M, Collura D, Ghiggi MR, Nir-
Freinkel N. Disparate thyroid imaging: com-
chio V, Trischitta V. Treatment of large cold
bined studies with sodium pertechnetate Tc
benign thyroid nodules not eligible for sur-
99m and radioactive iodine. JAMA 1974;228:
gery with percutaneous ethanol injection.
J Clin Endocrinol Metab 1998;83:3905-7. 14. Marqusee E, Benson CB, Frates MC, et al. 29. Papini E, Petrucci L, Guglielmi R, et al. 43. Døssing H, Bennedbæk FN, Karstrup S,
Usefulness of ultrasonography in the man-
Long-term changes in nodular goiter: a 5-year
Hegedüs L. Benign solitary solid cold thyroid
prospective randomised trial of levothyrox-
nodules: US-guided interstitial laser photo-
ine suppressive therapy for benign cold thy-
coagulation — initial experience. Radiology
15. Jennings A. Evaluation of substernal
roid nodules. J Clin Endocrinol Metab 1998;
44. Hegedüs L, Hansen JM, Karstrup S, 30. Sawin CT, Geller A, Wolf PA, et al. Low
Torp-Pedersen S, Juul N. Tetracycline for scle-
serum thyrotropin concentrations as a risk
rosis of thyroid cysts: a randomized study. 16. Kang KW, Kim S-K, Kang H-S, et al.
factor for atrial fibrillation in older persons.
Prevalence and risk of cancer of focal thy-
45. Bennedbæk FN, Hegedüs L. Treatment
roid incidentaloma identified by 18F-fluo-
31. Surks MI, Ortiz E, Daniels GH, et al.
of recurrent thyroid cysts with ethanol: a ran-
Subclinical thyroid disease: scientific review
domized double-blind controlled trial. J Clin
raphy for metastasis evaluation and cancer
screening in healthy subjects. J Clin Endo-
46. Feld S, Garcia M, Baskin HJ, et al. AACE 32. Uzzan B, Campos J, Cucherat M, Nony
clinical practice guidelines for the diagnosis
17. Mazzaferri EL. Management of a soli-
P, Boissel JP, Perret GY. Effects on bone mass
and management of thyroid nodules. Endocr
tary thyroid nodule. N Engl J Med 1993;328:
mones: a meta-analysis. J Clin Endocrinol
Copyright 2004 Massachusetts Medical Society.18. Burch HB. Evaluation and management
of the solid thyroid nodule. Endocrinol Metab
33. McCowen KD, Reed JW, Fariss BL. The
role of thyroid therapy in patients with thy-
19. Danese D, Sciacchitano S, Farsetti A,
Andreoli M, Pontecorvi A. Diagnostic accu-
34. Hegedüs L, Nygaard B, Hansen JM. Is
The New England Journal of Medicine as published by New England Journal of Medicine.
Downloaded from www.nejm.org on August 2, 2010. For personal use only. No other uses without permission.
Copyright 2004 Massachusetts Medical Society. All rights reserved.
OUR BRAVE NEW PHARMACOLOGICAL WORLD: A VIRTUE ETHICS CRITIQUE Steven D. WeissAugusta State University It’s not difficult to say what’s objectionable about soma in AldousHuxley’s Brave New World : the majority of the blissed-out, mindless deni-zens of this socially and biologically engineered dystopia are obliviousnot only to their own manipulation but also to the fact that their liveshav
Spiagge, immersioni e tartarughe nel nord di Cipro Il nord di Cipro offre al Turista spiagge con acque limpide e cristalline come difficilmente si possono trovare nel mediterraneo. Le sue coste sono variegate: roccia e sabbia si mescolano in un connubio unico. Chilometri e chilometri di spiagge sabbiose nascoste dietro alle dune. Sulla costa est tra Famagosta e Bogaz, troverete un ar
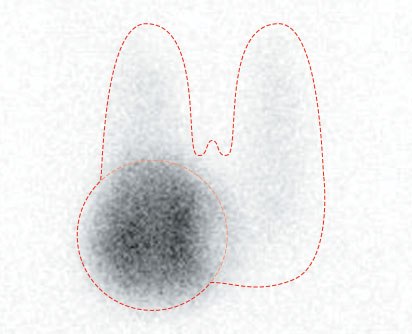
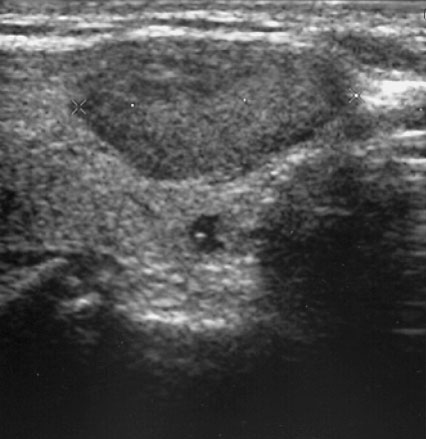 Figure 2. Scintigram of a Solitary Functioning Nodule
Figure 2. Scintigram of a Solitary Functioning Nodule