Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Microsoft word - txa_clin_prot_12-05-2010.doc
Perioperative Cardiac Surgical Tranexamic acid (TXA) Administration‡
Department of Anesthesiology and Perioperative Medicine
Regimen #1: Normal Renal Function
TXA 30 mg/kg load over 20 min (comes as [20 mg/mL])7
TXA 2 mg/kg load to CPB prime TXA 16 mg/kg/hr continuously4
Regimen #2: Renal Insufficiency (Cr > 2.0)
TXA 30 mg/kg load over 20 min (comes as [20 mg/mL]) 7 No load to CPB prime TXA 8 mg/kg/hr continuously4
Dose after heparinization
Regimen #3: Dialysis dependent TXA 30 mg/kg load over 20 min (comes as [20 mg/mL]) 7 No load to the CPB prime No infusion
†Clinical protocols are based on the best and most recent available data and are expected to be followed by all CASECAG staff unless there is a compelling clinical reason not to, or new data becomes available that suggests an alternate treatment protocol. Standardizing our approach to some of our practices is expected to reduce drug errors in the clinical environment and increase work flow for the trainees. ‡Administration of TXA to cardiac surgical patients is considered a Class IA (I=Benefit>>>Risk, treatment should be performed, A=Strongest evidence supporting treatment based multiple prospective trials and/or meta-analyses) recommendation to reduce the total number of patients who require blood transfusion and reduce the amount of blood loss after cardiac operations. (Ferraris et al.) 1: The safety of TXA for OPCAB is not well established and therefore its use should be avoided in this circumstance. OPCAB surgery has been shown to be associated with a hypercoaguable state postoperatively and without the anticoagulation effects of CPB its use may put the patient at risk for early graft closure or other thromboembolic complications. (Kon et al, Desai et al.) If TXA is being considered for a non-cardiac surgical procedure which is expected to involve heavy bleeding (e.g., trauma or redo orthopedic spine surgery) then it may be permissible to electively and prophylactically administer TXA if the patient is known to not have severe peripheral vascular disease or a thrombophilia. (Verma et al., Berenholtz et al.) 2: A screening for hypercoaguable states should be a regular part of each patient’s review of systems (e.g., query whether the patient has ever had a DVT or pulmonary embolus). If the patient is known to possess any of the following conditions prophylactic administration of TXA may not be safe and it is not recommended. Rescue administration of TXA to severely hemorrhaging patients with any of these diagnoses is left to the discretion of the clinicians providing care.
Heparin Induced Thrombocytopenia and Thrombotic Syndrome (HITTS)
Factor V Leiden Mutation Protein C Deficiency or Resistance
Anti-phospholipid antibody syndrome (APS)
3: Pre-sternotomy administration of TXA is probably optimal to prevent the fibrinolysis that accompanies surgical trauma, inflammation and the institution of CPB. The efficacy of pre-sternotomy administration of TXA is supported by multiple prospective clinical trials. If the patient is known to possess severe occlusive coronary disease, a low flow state (i.e. cardiogenic shock) or an active coronary thrombus the Amicar should not be administered until the patient has been fully heparinzed for CPB (i.e., ACT > 400 seconds). In the absence of severe vascular disease or an active coronary thrombus in an unheparinized patient it is optimal to administer the TXA following induction but prior to sternotomy. 4: Note 90% of IV administered TXA is excreted unchanged in the urine and higher levels of TXA are associated with a greater incidence of seizures. The incidence of seizure may be higher in individuals with a pre-existing seizure disorder. 5: If deep hypothermic circulatory arrest (DHCA) is planned then the TXA infusion should be temporarily paused while there is no systemic blood circulation (i.e. during DHCA). This will prevent a local accumulation of the TXA at the point where the drug is entering the vascular system. Failure to stop the TXA during DHCA can result in a large thrombus formation local to the exit port on the catheter that the drug is infusing from.
6: Rescue TXA is a term that refers to the administration of TXA after the surgical procedure, or the majority of it, has already been completed and no TXA was administered prophylactically at the start of the procedure. In this case if the patient is bleeding and other relevant clinical factors such as hypothermia, coagulopathy, thrombocytopenia and heparin rebound have been addressed then it may be helpful to administer TXA if the patient is thought to be at risk for fibrinolysis and its associated increased hemorrhage. A Thromboelastograph (TEG) can establish the presence of fibrinolysis in approximately 30 minutes. If there is no detectable fibrinolysis by the TEG then administration of TXA would not be expected to help greatly with the bleeding. Conversely, not all patients with measurable fibrinolysis will demonstrate excessive hemorrhage. 7. Drug delivery: TXA is most safely administered using a volumetric pump. Outlined below is an example of how to deliver the TXA in Drug Delivery Mode.
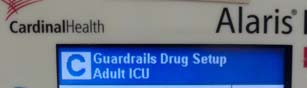
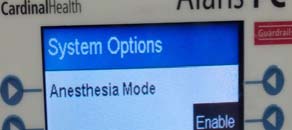
Step 1: Choose the appropriate channel on Alaris pump and press the OPTIONS button and select Anesthesia Mode if the pump in not already in Anesthesia Mode.
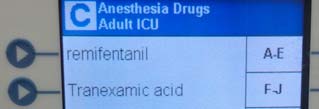
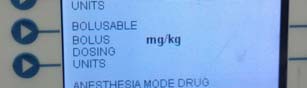
Step 2: Select Enable under Anesthesia Mode
Step 3: Select Tranexamic acid
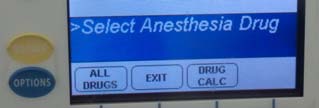
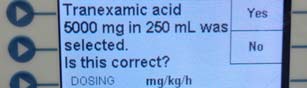
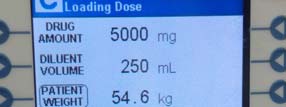
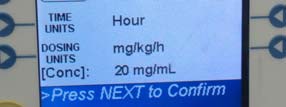
Step 4: Select Yes to confirm TXA concentration of
Step 5: Confirm patient weight and drug concentration
References: Ferraris VA, Ferraris SP, Saha SP, et al. Perioperative Blood Transfusion and Blood Conservation in Cardiac Surgery: The Society of Thoracic Surgeons and The Society of Cardiovascular Anesthesiologists Clinical Practice Guideline. Ann Thorac Surg 2007;83:S27-86 Kon ZN, Kwon MH, Kallam S, et al. Off-pump coronary artery bypass leads to a regional hypercoagulable state not detectable using systemic markers. Innovations Phila Pa 2006;1:232–8 Desai PH, Kurian D, Thirumavalavan N, et al. A Randomized Clinical Trial Investigating the Relationship Between Aprotinin and Hypercoagulabilityin Off-Pump Coronary Surgery. Anesth Analg 2009;109:1387-1394
Verma K, Errico TJ, Vaz KM, Lonner BS. A prospective, randomized, double-blinded single-site control study
comparing blood loss prevention of tranexamic acid (TXA) to epsilon aminocaproic acid (EACA) for corrective spinal surgery. BMC Surg 2010;10:13
Berenholtz SM, Pham JC, Garrett-Mayer E, et al. Effect of epsilon aminocaproic acid on red-cell transfusion
requirements in major spinal surgery. Spine 2009, 34(19):2096-103.
Rolf HOFFMANN TrichoScan: combining epiluminescence microscopy with digital image analysis for the measurement of hair growth in vivo Hair loss or hair thinning is a common complaint in clinical dermatology,and patients seeking advice for hair loss are not necessarily bald. Also theeffects of treatment attempts are hard to measure. Consequently, there is aneed for a sensitive tool to monit
FLOWERDALE ESTATE ALPACAS Health & Husbandry Herd Health & Management The nature of a llama/alpaca herd health program has been markedly influenced by variables including owner’s background, numbers of animals, purpose of animals, geographical location, economics and, quite understandably, the background and species orientation of the veterinarian involved. In the following


 Perioperative Cardiac Surgical Tranexamic acid (TXA) Administration‡
Perioperative Cardiac Surgical Tranexamic acid (TXA) Administration‡ 
 6: Rescue TXA is a term that refers to the administration of TXA after the surgical procedure, or the majority of it, has already been completed and no TXA was administered prophylactically at the start of the procedure. In this case if the patient is bleeding and other relevant clinical factors such as hypothermia, coagulopathy, thrombocytopenia and heparin rebound have been addressed then it may be helpful to administer TXA if the patient is thought to be at risk for fibrinolysis and its associated increased hemorrhage. A Thromboelastograph (TEG) can establish the presence of fibrinolysis in approximately 30 minutes. If there is no detectable fibrinolysis by the TEG then administration of TXA would not be expected to help greatly with the bleeding. Conversely, not all patients with measurable fibrinolysis will demonstrate excessive hemorrhage. 7. Drug delivery: TXA is most safely administered using a volumetric pump. Outlined below is an example of how to deliver the TXA in Drug Delivery Mode.
Step 1: Choose the appropriate channel on Alaris pump
6: Rescue TXA is a term that refers to the administration of TXA after the surgical procedure, or the majority of it, has already been completed and no TXA was administered prophylactically at the start of the procedure. In this case if the patient is bleeding and other relevant clinical factors such as hypothermia, coagulopathy, thrombocytopenia and heparin rebound have been addressed then it may be helpful to administer TXA if the patient is thought to be at risk for fibrinolysis and its associated increased hemorrhage. A Thromboelastograph (TEG) can establish the presence of fibrinolysis in approximately 30 minutes. If there is no detectable fibrinolysis by the TEG then administration of TXA would not be expected to help greatly with the bleeding. Conversely, not all patients with measurable fibrinolysis will demonstrate excessive hemorrhage. 7. Drug delivery: TXA is most safely administered using a volumetric pump. Outlined below is an example of how to deliver the TXA in Drug Delivery Mode.
Step 1: Choose the appropriate channel on Alaris pump