Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Microsoft word - caseemsstandardop procedures.doc
CaseEMS Patient Care Guidelines INTRODUCTION
These protocols represent the consolidation of recommendations for emergency pre-hospital patient care from many local and national sources. They are not intended to be absolute treatment doctrines, but rather guidelines which have sufficient flexibility to meet the complex challenges faced by EMS providers in the field. The assessment information in the General Orders is intended to be considered with all protocols. In addition, the General Medical Assessment should be considered with all medical protocols, the General Trauma Assessment should be considered with all trauma protocols, and the Pediatric Assessment should be considered with all pediatric protocols. These protocols are intended to: 1. Provide a guide to the appropriate emergency medical care procedures to be employed by
EMS personnel while working under the direction of the Medical Director;
2. Provide EMS personnel with a framework for pre-hospital care; 3. Provide the basic framework from which quality improvement programs can be
They are not intended to: 1. Be a statement of the standards of care required in any particular situation, but rather
guidelines with sufficient flexibility to meet the needs of complex emergency medical or trauma situations;
2. Be a teaching manual for EMS personnel; it is assumed that EMS personnel are
appropriately trained and that each person will continue to meet the state’s continuing education requirements for recertification;
3. Interfere with the wishes of the patient or family, or the wishes of the patient's personal
TABLE OF CONTENTS
GENERAL ORDERS. 4 GENERAL MEDICAL ASSESSMENT. 5 MEDICAL EMERGENCIES . 6
Allergic Reaction. 6 Altered Mental Status . 7 Behavioral Emergencies. 8 Bites and Stings - Venomous . 9 Cardiovascular Emergencies. 10 Diabetic Emergencies. 11 Fever . 12 Heat Emergencies . 13 Hypothermia . 14 Local Cold Injuries (Frostbite, Frostnip). 15 Poisoning/Overdose . 16
Ingested Substances . 16 Inhaled Substances . 16 Toxic Injection . 16 Absorbed Substances. 17
Respiratory Emergencies . 18 Seizures . 19
Excessive Vaginal Bleeding. 20 Sexual Assault. 20
Miscarriage - Spontaneous Abortion . 21 Pre-delivery Seizures (Eclampsia/Pre-eclampsia). 21 Emergency Delivery . 22
Complications of Deliveries: Prolapsed Cord . 22 Complications of Deliveries: Breech Birth and/or Limb Presentation . 23 Complications of Deliveries: Meconium Staining . 23
Abdominal Injury. 25 Burns . 26 Chest Injury . 27 Drowning and Near Drowning. 28 External Bleeding and Amputations. 29 Extremity Injury. 30 Head and Spine Injury . 31 Shock . 32
PEDIATRIC ASSESSMENT. 33 APPENDICES GLOSSARY
GENERAL ORDERS
1. Scene Size-up/Assessment
Don appropriate Body Substance Isolation (BSI) prior to patient contact
Always ensure scene safety and request additional help, if needed
C. Look for hazards that may jeopardize the safety of the patient AND the crew
2. Initial Patient Assessment
A. Airway - Breathing – Circulation B.
Identify any existing or potential life-threatening conditions and address immediately
Focused History and Physical Exam - Medical Patients Focused History and Physical Exam- Trauma Patients Detailed Physical Exam A.
Perform a detailed physical examination for additional information
Ongoing Assessment
Repeat and record initial patient assessment, including time
Maintain open airway and monitor breathing for rate and quality
Reassess and record vital signs, include time
G. Repeat focused assessment of patient complaint or injuries H. Check
Communications
Provide a verbal, and if possible, a written report to receiving unit (Cleveland EMS, Cleveland Fire, Cleveland Heights Fire, etc.)
For critical patients, consider giving an update to responding units while they are enroute (e.g., cardiac arrest, respiratory arrest)
C. Hand over care of the patient only to equally or more qualified personnel, and
only if they agree to continue to provide care. If in doubt, call for assistance from the responding EMS unit or Medical Command at University Hospitals
GENERAL MEDICAL ASSESSMENT Initial Patient Assessment Focused History and Physical Exam
A. Get information from family or bystanders for unresponsive patients
B. Determine complaints and assess signs and symptoms
1) Conduct AVPU mental status exam as needed
Perform Ongoing and/or Detailed Assessment as Needed MEDICAL EMERGENCIES ALLERGIC REACTION
1) Not all signs and symptoms are present in every case 2) History – previous exposure; previous experience to exposure; onset of
3) Level of Consciousness – unable to speak; restless; decreased level of
4) Upper Airway – hoarseness; stridor; pharyngeal edema/spasm 5) Lower Airway – tachypnea: hypoventilation: labored-accessory muscle use;
abnormal retractions; prolonged expirations; wheezes; diminished lung sounds
6) Skin – redness; rashes; edema; moisture; itching; urticaria: pallor: cyanotic 7) Vital Signs – tachycardia; hypotension 8) Gastrointestinal – abnormal cramping; nausea/vomiting; diarrhea
1) Ensure that Cleveland EMS/Fire/CHFD has been activated and is en-route. 2) Remove offending agent (e.g., stinger) 3) Clear the airway, provide oxygen and/or ventilatory assistance as necessary
of not done during Initial Patient Assessment
4) For Anaphylaxis/Allergic Reaction with Severe Respiratory Distress
a) Treat for shock, if necessary b) Assist patient with Epinephrine Auto-Injector, if available after consulting
5) Monitor pulse oximetry if available 6) Psychological support
• Life threatening airway/respiratory compromise may develop as the reaction
• Not all signs and symptoms are present in every case. Carefully dispose of used
MEDICAL EMERGENCIES ALTERED MENTAL STATUS
1) Difficulty speaking or following commands 2) Confusion 3) Unresponsiveness
1) Attempt to determine cause (e.g., hypoglycemia, poisoning, post seizure,
2) Provide oxygen and/or ventilatory assistance as necessary, if not done during
3) Check blood glucose (see Diabetic Emergencies, page 11) 4) Monitor pulse oximetry
• Double-check that the scene is secure. Amongst other things, carbon monoxide
and certain chemicals can lead to altered mental status and affect rescuers.
• Remember to consider the possibility of head and/or c-spine trauma.
MEDICAL EMERGENCIES BEHAVIORAL EMERGENCIES CAUTION:
Guarantee your own safety FIRST! If show of force necessary to render care, contact law enforcement and await their arrival prior to proceeding. Assess and treat life-threatening problems only when able to safely.
a) Panic b) Agitation c) Bizarre behavior d) Danger to self or others
a) Depression b) Suicidal gestures c) Mental Status Examination (see Altered Mental Status, page 7)
1) One EMT to assume control of situation 2) Speak in a calm quiet voice, maintain eye contact and move slowly 3) Answer questions honestly 4) Do not leave the patient alone or turn your back
• Never place yourself or your crew in a dangerous situation. • Be alert! Patient behavior may change rapidly and the scene may become
unsafe. Always have a strategy to rapidly exit the scene if necessary.
• If possible, do not stand between the patient and the doorway. The patient may
try to go through you to exit the scene.
MEDICAL EMERGENCIES BITES AND STINGS - VENOMOUS
1) History of bite (spider, snake) or sting (insect, scorpion or marine animal) 2) Pain 3) Redness and/or swelling 4) Weakness and/or dizziness 5) Chills or fever 6) Nausea and vomiting 7) Bite marks or stinger
1) If stinger is present, scrape the sting site to remove the stinger 2) Wash area gently 3) Remove jewelry from the affected limb before swelling begins, if possible 4) For poisonous bites, splint the limb and place below the level of the heart,
5) Observe for development of signs and symptoms of an allergic reaction (see
not pull the stinger. It can lead to further envenomation. Scrape the stinger
not apply constricting bands or tourniquets to bites.
not use venom extraction pumps or attempt to suck out venom.
MEDICAL EMERGENCIES CARDIOVASCULAR EMERGENCIES
1) Chest pain 2) Difficulty breathing 3) Skin changes (pale, sweaty, cyanotic) 4) Anxiety/irritability (feeling of impending doom) 5) Circulatory (irregular pulse, BP, shock, pulselessness) 6) Nausea/vomiting
a) Provide supplemental oxygen and/or ventilatory assistance if needed and
not done during Initial Patient Assessment
b) If the patient’s own physician-prescribed Nitroglycerin is available, assist
patient with self administration of Nitroglycerin, after consulting medical control (1) patient must have systolic BP >100 (2) give every 3-5 minutes (up to a maximum of 3 doses) (3) recheck BP prior to each dose (4) allow patient to achieve safe position of comfort
a) Check respirations and pulse b) Provide supplemental oxygen and/or ventilatory assistance as necessary,
if not done during Initial Patient Assessment
c) If not breathing, insert oral airway and begin rescue breathing using Bag-
d) If pulseless, begin CPR and apply AED (see Resuscitation Appendix)
MEDICAL EMERGENCIES DIABETIC EMERGENCIES
a) Dizziness and headache b) Abnormal, hostile or aggressive behavior c) Fainting, convulsions d) Full rapid pulse e) Skin pale, cold and clammy f) Copious saliva, drooling
a) Dry mouth, and intense thirst b) Abdominal pain and vomiting c) Restlessness d) Weak rapid pulse e) Dry, red, warm skin
1) Check blood glucose using glucometer 2) If glucose is < 80 mg/dL and patient is able to swallow, administer oral
glucose, or substance high in simple sugar (e.g, honey, orange juice with 2-3 tsp of sugar)
3) Provide supplemental oxygen and/or ventilatory assistance as necessary, if
not done during Initial Patient Assessment
• If patient cannot adequately protect airway, do NOT administer anything by
• If patient has a blood glucose > 80 mg/dL, do not administer glucose.
MEDICAL EMERGENCIES
1) Flushed, warm dry skin 2) Restless 3) May have rash or stiff neck 4) Seizures 5) Dehydration, decreased urine output
1) Provide supplemental oxygen and/or ventilatory assistance as necessary, if
not done during Initial Patient Assessment
a) Loosen tight clothing or undress children b) Use tepid water to cool patient
• Consider the use of masks and even full body substance isolation procedures
when handling patients with fever. Diseases such as meningitis and tuberculosis may cause fever and may be spread by respiratory droplets.
MEDICAL EMERGENCIES HEAT EMERGENCIES
1) Muscular cramps 2) Weakness or exhaustion 3) Dizziness or faintness 4) Skin
a) Moist or dry b) Temperature c) Redness
5) Rapid heart rate 6) Altered mental status or unresponsive
1) Patient with moist, normal to cool temperature skin
a) Remove patient from the hot environment and place patient in a cool
environment (e.g., the back of an air-conditioned ambulance)
b) Provide oxygen and/or ventilatory assistance as necessary, if not done
c) Loosen or remove clothing d) Cool patient by fanning e) Place patient in supine position with legs elevated f) If patient is responsive and not nauseated, have patient drink water
a) Remove patient from the hot environment and place patient in a cool
environment (back of an air-conditioned ambulance with air conditioner running on high)
b) Provide supplemental oxygen and/or ventilatory assistance as
necessary, if not done during Initial Patient Assessment
c) Remove clothing d) Apply cool packs to neck, groin, and armpits e) Keep skin wet by applying water by sponge or wet towels f) Fan
MEDICAL EMERGENCIES HYPOTHERMIA
1) Environmental conditions of cold exposure 2) Cool to cold skin temperature 3) Decreased mental and/or motor status 4) Stiff or rigid posture or muscles 5) Shivering may be present or absent 6) Abnormal breathing
a) Early Æ rapid b) Late Æ slow or absent
7) Low to absent blood pressure 8) Slowly responding pupils 9) Inappropriate judgment 10) Complaints of joint or muscle stiffness 11) Skin may be red (early), pale, cyanotic, and/or stiff
1) Remove patient from the cold environment and protect the patient from
2) Remove patient’s wet clothing and wrap the patient in blankets 3) Handle with extreme care 4) Care for shock and provide oxygen 5) For unresponsive patients, assess pulse for 30-45 sec before starting CPR
a) If no pulse, begin CPR (see Resuscitation Appendix) b) Place AED c) Continue efforts to rewarm
(1) Warm blankets (2) Turn up heat high in the patient compartment of the ambulance (3) Do not massage extremities (4) Do not allow patient to remain in, or return to, a cold environment
d) If pulseless and directed by the machine, defibrillate
6) If the patient is alert and responding appropriately, actively rewarm
a) Apply warm blankets b) Place heat packs to groin, axillary, and cervical regions c) Turn up heat high in the patient compartment of the ambulance d) Do not allow patient to have any stimulants (caffeine, chocolate, etc.) e) Do not allow the patient to walk or exert themselves
7) Check and Record Pulse and Vitals, including temperature if possible
• Handle patient gently; ventricular fibrillation may result from rough handling • Efforts at defibrillation may be successful after warming • Patients should be warmed to normal temperatures before stopping resuscitation MEDICAL EMERGENCIES LOCAL COLD INJURIES (FROSTBITE, FROSTNIP)
1) Local injury with clear demarcation 2) Early or superficial injury
a) Blanching of the skin b) Loss of feeling and sensation in the injured area and the skin remains soft c) If rewarmed, tingling sensation
a) White, waxy skin which feels firm to frozen on palpation b) Swelling and/or blisters may be present c) If thawed or partially thawed, the skin may appear flushed with areas of
purple and blanching or mottled and cyanotic
1) Remove patient from the cold environment and protect the patient from
2) Protect the cold injured part from further injury 3) Remove wet or restrictive clothing 4) If early or superficial
a) If the injury is to an extremity, splint and cover the extremity b) Do not rub, massage, or re-expose to the cold
a) Remove jewelry b) Cover with dry clothing or dressings c) Do not rub, massage, apply heat, or rewarm d) Do not allow the patient to walk on the affected extremity
6) Do not allow patient to remain in or return to a cold environment 7) If necessary, gently dry affected area and apply a dry sterile dressing
a) Be sure fingers and toes are separated by sterile dressings
8) Keep area warm and not put any pressure on the site 9) Keep patient at rest and protect the part from refreezing 10) Expect the patient to complain of severe pain
MEDICAL EMERGENCIES POISONING/OVERDOSE
CAUTION: Do not expose yourself to toxic atmospheres or substances without proper
training, PPE and other equipment. If caregiver or patient is exposed consider primary HAZMAT decontamination.
1) History of ingestion 2) Nausea, vomiting, diarrhea, altered mental status, abdominal pain, chemical
burns around the mouth, unusual breath odors
1) Remove pills, tablets or fragments from patient’s mouth if found 2) Provide oxygen and/or ventilatory assistance as necessary, if not done during
1) History of inhalation of toxic substance 2) Difficulty breathing, chest pain, cough, hoarseness, dizziness, headache,
confusion, seizures, altered mental status
1) Provide oxygen and/or ventilatory assistance as necessary, if not done during
Toxic Injection (see also Bites and Stings, page 9)
1) Weakness, dizziness, chills, fever, nausea, vomiting
1) Provide oxygen and/or ventilatory assistance as necessary, if not done during
1) History of exposure 2) Liquid or powder on patient’s skin, burns, itching, irritation, redness
a) Remove contaminated clothing while protecting self from contamination b) If powder present, brush off patient c) Irrigate with copious amounts of water for at least 20 minutes unless the
substance is known to be reactive with water (e.g., alkali metals, alkaline earth metals, anhydrides, certain carbides, hydrides, sodium hydrosulfite)
a) Irrigate with clean water away from unaffected eye for at least 20 minutes
• Be prepared for vomiting, seizures, or further deterioration of the patient • Bring all containers, bottles, labels, etc. of poison agents to receiving facility if
Depending on the substance involved, life threatening airway/respiratory
compromise or shock may develop as the reaction progresses
MEDICAL EMERGENCIES RESPIRATORY EMERGENCIES
1) Anxiousness/restlessness 2) Shortness of breath - air hunger, increased/decreased/absent respirations 3) Skin color changes - cyanosis, pale/clammy, redness/flushing 4) Abnormal airway noises - wheezing, stridor, gurgling, snoring 5) Mechanics of respiration - fatigue due to breathing effort, diaphragmatic
breathing, retractions, irregular breathing pattern
6) Patient position - upright, feet dependent, tripod 7) Drooling, difficulty swallowing, barky cough
1) Remove obstruction if any (see Airway Obstruction Appendix) 2) Provide supplemental oxygen and/or ventilatory assistance as necessary, if
not done during Initial Patient Assessment
3) Allow patient to achieve position of comfort 4) Prepare to manage/assist respirations if patient stops breathing or is unable
to maintain adequate breathing on their own
5) If the patient is wheezing, assist with the administration of inhaler
a) Only if the patient’s own prescribed inhaler is available (not a friend’s or
b) Consult with medical control prior to administration
1) Airway obstruction (see Airway Obstruction Appendix)
a) Use infant/child foreign body airway procedures if complete obstruction b) If incomplete obstruction
(1) Do not agitate patient (2) Allow patient position of comfort (3) Oxygen/limited exam
c) Patient drooling, with difficulty swallowing, or seal bark cough
(1) Assist ventilations as needed (2) Provide supplemental oxygen and/or ventilatory assistance as
necessary, if not done during Initial Patient Assessment
(3) Allow patient to achieve position of comfort (e.g., parent’s lap)
not attempt to visualize the oropharynx of drooling patients, particularly
MEDICAL EMERGENCIES SEIZURES
a) Aura – unusual smell, vision, or taste b) Abnormal twitch c) Dizziness
2) Sudden unresponsiveness 3) Convulsions 4) Loss of bowel and bladder control 5) Postictal state (recovery phase)
a) Confusion, disoriented and possibly combative b) Exhaustion and weakness
1) Maintain airway 2) Provide oxygen and/or ventilatory assistance as necessary, if not done during
3) Suction as needed 4) Prevent injury to the patient 5) Check blood sugar when safe to do so (see Diabetic Emergencies, page 11)
C. Pediatric Considerations - Febrile Seizure, Ingestion
1) Remove heavy or swaddling clothes, keep lightly dressed 2) Maintain airway 3) Provide oxygen and/or ventilatory assistance as necessary, if not done during
4) Suction as needed 5) Collect any open or empty pill containers for transport to the hospital
not place anything in the mouth of a seizing patient, including fingers or
bitesticks. They can lead to airway obstructions.
o Fever / Infections o Poisoning o Low blood sugar (hypoglycemia) o Stroke o Head trauma o Hypoxia (oxygen starvation) o Pre-delivery seizure (eclampsia)
GYNECOLOGICAL EMERGENCIES
1) Provide supplemental oxygen and/or ventilatory assistance as necessary, if
not done during Initial Patient Assessment
2) Treat for shock (see Shock, page 32) 3) Do not examine genitalia unless obvious bleeding requires the application of a
4) If bleeding due to trauma to external genitalia, place appropriate external
1) Provide supplemental oxygen and/or ventilatory assistance as necessary, if
not done during Initial Patient Assessment
2) Follow treatment protocols for victims of trauma 3) Advise patient not to wash, douche, urinate or defecate prior to physician
4) Do not examine genitalia unless obvious bleeding requires the application of a
5) Provide non-judgmental emotional support
• Protect potential crime scene and any evidence as much as possible. OBSTETRICAL EMERGENCIES
1) Cramp-like lower abdominal pain similar to labor 2) Moderate to severe vaginal bleeding, which may be bright or dark red 3) Passage of tissue or blood clots
1) Provide supplemental oxygen and/or ventilatory assistance as necessary, if
not done during Initial Patient Assessment
2) Treat for shock (see Shock, page 32) 3) Place sterile pad over vaginal opening 4) If passed material has any possibility of being viable, or if unsure about
5) Send any passed tissue to the hospital, if possible
Pre-delivery Seizures (Eclampsia/Pre-eclampsia)
a) Hypertension (moderate, above 140 and below 160) b) Edema c) Rapid weight gain
a) Hypertension above 160 systolic b) Headache c) Changes in behavior d) Visual disturbances e) Dyspnea f) Cyanosis
1) Provide supplemental oxygen and/or ventilatory assistance as necessary, if
not done during Initial Patient Assessment
2) Take seizure precautions (see Seizures, page 19) 3) Place patient on left side if possible
1) Date of expected birth 2) Onset of contractions/pain 3) Any bleeding or discharge 4) Number or pregnancies/births 5) Duration and frequency of contractions
B. Signs and Symptoms of Imminent Delivery
1) Perineum bulging or baby crowning 2) Contractions < 2 minutes apart 3) Mother expresses the need to "push" or "bear down"
1) Have mother lie supine with knees drawn up and spread apart 2) Prepare OB kit 3) When the infant's head appears during crowning, place fingers on bony part
of skull and exert very gentle pressure to prevent explosive delivery
4) When head is delivered, suction infant's nose and mouth with bulb syringe 5) Assist delivery of shoulders and body; do not pull on infant 6) When baby is delivered:
a) Wipe blood and mucus from mouth and nose, suction mouth and nose
b) Assure patient airway, stimulate cry by tapping soles of feet c) Do APGAR assessment on infant one minute after delivery (appearance,
pulse, grimace, activity, respiratory effort – see APGAR in Appendix)
d) Wrap infant in warm blanket and place on its side, head slightly lower than
e) Keep infant level with vagina until the cord is cut f) As pulsations cease; double clamp, tie and cut cord between two clamps g) Let placenta deliver normally
• Do not pull on cord. • Place placenta in plastic bag and transport with mother • Massage mother's lower abdomen until firm • Estimate blood loss, treat for shock as necessary • Record time of delivery
COMPLICATIONS OF DELIVERIES: Prolapsed Cord
1) Cord presents through the birth canal before delivery 2) Normally occurs early in labor
1) Provide supplemental oxygen and/or ventilatory assistance as necessary, if
not done during Initial Patient Assessment
2) Position mother in knee chest position or extreme Trendelenburg 3) Insert sterile gloved hand into vagina pushing the presenting part of the fetus
4) Keep pressure on presenting part and monitor pulsations in the cord 5) Continue monitoring pulsations until relieved at the hospital
COMPLICATIONS OF DELIVERIES: Breech Birth and/or Limb Presentation
1) Buttocks or extremities present first during the delivery process
1) Provide supplemental oxygen and/or ventilatory assistance as necessary, if
not done during Initial Patient Assessment
2) Allow delivery to progress spontaneously 3) Support infant's body as it is delivered 4) If head delivers spontaneously, proceed as with normal delivery 5) If head does not deliver within 4-6 minutes:
a) Insert gloved hand into vagina, create an airway for the baby b) Place mother in head down position with pelvis elevated c) Do not remove hand from inside vagina until relieved by hospital staff
COMPLICATIONS OF DELIVERIES: Meconium Staining
1) Greenish or brownish-yellow amniotic fluid rather than clear 2) Discoloration/staining on infant’s face 3) Often indicates possible fetal distress during labor
1) Do not stimulate infant to breath prior to suctioning 2) Suction oropharynx and nasopharynx 3) Maintain infant’s airway
GENERAL TRAUMA ASSESSMENT
A. Ensure scene safety B. Assess for number of patients C. Update responding agencies, if needed, on number and condition of patients as
A. Airway, Breathing, Circulation - establish patient care priorities as soon as
B. Triage multiple patients using START Trauma Triage Procedures (see Appendix)
i) Prioritize Patient Transport in conjunction with other responding agencies
ii) Glasgow Coma Scale (GCS) (see Appendix) iii) Vital Signs iv) Deformities, Contusions, Abrasions, Punctures - Burns, Tenderness,
i) Re-evaluate Initial Patient Assessment Items
(1) Unstable patient a minimum of every 5 minutes (2) Stable patient every 15 minutes
FOR MULTI-SYSTEM/TIME CRITICAL TRAUMA
A. Begin extrication (if necessary) and treatment simultaneously, if possible
1) Immediate manual head and C-spine immobilization 2) Treat life-threatening injuries as they are found
B. Assess for other signs and symptoms, including a rapid survey of head, chest,
C. Notify the responding EMS transport agency of the patient’s condition ASAP
D. Limit on-scene time to 10 minutes, whenever possible
ABDOMINAL INJURY
1) Tender, rigid, or distended abdomen 2) Position (guarding) 3) Signs and symptoms of shock 4) Wounds, bruising
1) Assure patent airway 2) Provide oxygen and/or ventilatory assistance as necessary, if not done during
3) Cover exposed organs with sterile/moist dressing 4) Control bleeding 5) Treat for shock if necessary (see Shock, page 32) 6) Spinal immobilization if necessary 7) Give nothing by mouth 8) Position supine with flexed knees, if no contraindications
• Consider whether a spinal injury may have occurred • Consider pregnancy (see Obstetrical Emergencies, page 21) • Do
not touch or try to replace exposed organs
A. Signs and Symptoms
1) Evaluate depth and area by using Rule of Nines (see Appendix) 2) Carefully evaluate respiratory tract for involvement: singed nasal hair, hoarse
1) Identify source of burning and take appropriate safety precautions 2) Assure patent airway 3) Provide oxygen and/or ventilatory assistance as necessary, if not done during
Initial Patient Assessment a) Continuously reassess respiratory status
4) Remove jewelry and non-adhered clothing as necessary 5) Cover burns with dry sterile dressing 6) Control bleeding 7) Treat for shock (see Shock, page 32)
• Identify source of burning and take appropriate safety precautions for crew and
• Stop the burning process as soon as safely possible • For burns involving chemicals, refer to the Poisoning/Overdose protocol (see
• Burns may be more severe than they first appear
CHEST INJURY
1) Changes in respiratory rate/quality 2) Breath sounds diminished, unequal, or absent 3) Flail chest 4) Use of accessory muscles 5) Distended neck veins (JVD) 6) Shock 7) Wounds, (entrance/exit), bruising 8) Complains of pain with inspiration or expiration
1) Assure patent airway 2) Provide oxygen and/or ventilatory assistance as necessary, if not done during
Initial Patient Assessment a) Continuously reassess respiratory status
3) For an open pneumothorax (sucking chest wound), cover immediately and when
time allows place an occlusive dressing taped only on three sides
4) Control bleeding 5) Treat for shock (see Shock, page 32) 6) Spinal immobilization as necessary
• Consider whether a thoracic spinal injury may exist • If an open pneumothorax patient seems to get worse after placing the occlusive
dressing, REMOVE the dressing immediately
DROWNING AND NEAR DROWNING CAUTION: Always assure the safety of the rescue personnel.
1) Consider length of time in cold water drowning. Any pulseless, non-breathing
patient who has been submerged in cold water should have resuscitation efforts initiated (See Hypothermia, page 14).
1) All drowning and near-drowning patients
a) In-line immobilization and removal from water with a backboard if spine
injury is suspected or the patient is unresponsive
b) If there is no suspected spinal injury, place patient on left side to allow
water, vomitus and secretions to drain from the upper airway
c) Provide supplemental oxygen and/or ventilatory assistance as
necessary, if not done during Initial Patient Assessment
d) If gastric distention interferes with artificial ventilation:
(1) Place patient on their left side, while continuing to protect the c-spine (2) Have suction immediately available (3) Place hand over the epigastric area of the abdomen (4) Apply firm pressure to relieve the distention
2) For pulseless and non-breathing drowning patients, follow the Cardiovascular
• Always be suspicious of spinal injuries in drowning and near-drowning patients. • Be careful to be away from the water and, to the extent possible, dry off the
patient prior to attempting defibrillation. Be particularly careful of crew members or helpers when delivering shocks.
EXTERNAL BLEEDING AND AMPUTATIONS
1) Spurting/steady flowing or oozing blood 2) Bright red or dark blood 3) Separated or displacement of body part or tissue 4) Shock
1) Assure patent airway 2) Provide oxygen and/or ventilatory assistance as necessary, if not done during
a) Direct pressure b) Elevation c) Pressure point d) Splints
4) Apply dressing and bandage 5) Do not remove impaled objects unless impaled in cheek and airway is
compromised by the object a) Secure impaled objects in place
6) Treat for shock if necessary (see Shock, page 32) 7) Amputations
a) Wrap severed body part in dry sterile dressing b) Wrap or bag amputated part in plastic and keep cool, but do not place on ice
c) Be sure that severed part is transported with patient, if possible
• Never use a tourniquet to control bleeding.
EXTREMITY INJURY
1) Exposed bone ends 2) Joints locked in position 3) Loss of feeling or movement 4) Loss of distal pulse 5) Bruising/swelling 6) Pain 7) Shock
1) Assure patent airway 2) Provide oxygen and/or ventilatory assistance as necessary, if not done during
3) Control bleeding 4) If necessary, treat for shock (see Shock, page 32) 5) Mechanically immobilize affected limb
a) Reassess distal pulse/motor/sensory before and after applying splint b) Consider application of cold pack to painful or swollen area c) Consider elevation of extremity d) Place traction splint on isolated femur fractures without knee or hip
HEAD AND SPINE INJURY
1) Cerebrospinal fluid or blood from nose, ears, mouth 2) Decreased Glasgow Coma Scale score (see Appendix) 3) Bruising around eyes, or behind ears 4) Altered mental status 5) Irregular breathing 6) Changes in pulse rate 7) Changes in blood pressure 8) Neurologic disability 9) Loss of bowel or bladder control 10) Unequal pupils with altered mental status 11) Seizures
1) Immediate manual head and C-spine immobilization 2) Assure patent airway 3) Provide oxygen and/or ventilatory assistance as necessary, if not done during
4) Control bleeding 5) If necessary, treat for shock (see Shock, page 32) 6) Apply longboard and collar with minimum possible movement of spine
1) Altered mental status 2) Shallow/rapid breathing 3) Restlessness/anxiety 4) Cyanosis or pale skin color 5) Cool/clammy skin 6) Weak rapid pulse 7) Decreasing blood pressure 8) Nausea/vomiting 9) Dilated pupils 10) Thirst
1) Assure patent airway 2) Provide oxygen and/or ventilatory assistance as necessary, if not done during
Initial Patient Assessment a) Continuously reassess respiratory status
3) Control bleeding 4) Give nothing by mouth 5) Elevate lower extremities, if no contraindications 6) Splint fractures 7) Prevent heat loss
• For anaphylaxis, refer to Allergic Reaction guidelines (see Allergic Reaction,
PEDIATRIC ASSESSMENT 1. Scene Size-up And Initial Patient Assessment
2. Assess ABC’s
a. Airway - Do not hyperextend or hyperflex child’s neck b. Breathing - Check for obstructions c. Circulation - Check capillary refill
3. Focused Assessment And Physical Examination
a. Consider the patient’s developmental stage when assessing signs and
b. Physical exam may be better tolerated if conducted from trunk to head c. Be alert for signs of child abuse and neglect
4. Ongoing Assessment APPENDICES
Albuterol Epinephrine Auto-Injector Nitroglycerin Oral Glucose
OXYGEN DELIVERY PULSE, BLOOD PRESSURE, AND RESPIRATION – NORMALS RESUSCITATION
Airway Obstruction - Foreign Body Cardiopulmonary Resuscitation Automated External Defibrillation
APGAR Scoring Glasgow Coma Scale Rule Of Nines - Estimating Burns
MEDICATION FORMULARY ALBUTEROL
o respiratory distress with wheezing o history of asthma or COPD with the patient’s prescribed inhaler available
o three doses have already been taken by the patient o patient’s own inhaler is not available
o two puffs every 5 minutes o may be repeated in three to five minutes if no relief, not contraindicated,
o dilates the bronchioles by relaxing smooth muscle
o increased heart rate o chest pain, cardiac arrythmias o dizziness o nausea o vomiting o excitability,
MEDICATION FORMULARY EPINEPHRINE AUTO-INJECTOR
o trade: Adrenaline, Epi-Pen, Epi-Pen Jr.
o patient exhibits signs of a severe allergic reaction, including either
o no contraindications when used in a life-threatening situation
o adult: one adult auto-injector (0.3 mg) o infant and child: one infant/child auto-injector (0.15 mg)
o dilates the bronchioles o constricts blood vessels
o increased heart rate o chest pain, cardiac arrythmias, cardiac arrest o pallor o dizziness o chest
o headache o nausea o vomiting o excitability,
MEDICATION FORMULARY NITROGLYCERIN
o generic: Nitroglycerin o trade: Nitrostat, Nitrobid, Nitrolingual Spray
o chest pain, thought to be of cardiac origin
o baseline systolic BP is below 100 mm/Hg o head injury suspected o patient is infant or child o three doses have already been taken by the patient
o one tablet or one spray under the tongue o may be repeated in three to five minutes if no relief, not contraindicated,
o dilates blood vessels o decreases heart workload
o headache o decreased blood pressure o changes in pulse
MEDICATION FORMULARY ORAL GLUCOSE
o generic: Glucose, oral o trade: Glutose, Insta-glucose, etc.
o patient with an altered mental status and a known history of diabetes
o unconsciousness o known diabetic who has not taken insulin for days o unable to swallow
o none when properly administered o may be aspirated by patient without a gag reflex
OXYGEN DELIVERY
A Delivery system of choice for patients with inadequate breathing and patients who are cyanotic, cool clammy,
short of breath, or suffering chest pain, suffering severe injuries, or displaying an altered mental status, or being transported.
B Depends on brand of bag valve mask and provisions for occluding room air inlet. C Should not be used on children under 12 years old.
1. Administration rates by nasal cannulae of over 4 L/min. are uncomfortable. 2. Use humidified oxygen, when possible, on infants, children, suspected respiratory tract burns, and
3. Bag Valve mask is not recommended for use in patients in transport situations. 4. Most hypoxic patients will feel better with an increase in delivered oxygen from 21% to 24%. 5. Pressure cycled ventilators are NOT acceptable alternatives to oxygen therapy. 6. Percentages of delivered oxygen listed above are based on optimal conditions. Altitude, equipment, etc.,
may decrease percentages of delivered oxygen.
1. The above values are based on full bottle (2,000 to 2,200 psi) at 70 degrees F. 2. Allow for pressure drop of 5 psi for every 1 degree drop in temperature below 70 degrees F.
PULSE, BLOOD PRESSURE, AND RESPIRATION - RANGES
TYPICAL ARTERIAL BLOOD PRESSURES (mm/Hg)
Systolic: Patient’s Age + 100 (Up to 150 mmHg) Diastolic: 60 to 90 mmHg
Systolic: Patients Age + 90 (Up to 140 mmHg) Diastolic: 50 to 80 mmHg
Note: The systolic and diastolic values given above may vary up or down from the mean.
NORMAL PULSE RATES (HEART BEATS PER MINUTE)
NORMAL RESPIRATORY RATES (RESPIRATIONS PER MINUTE)
RESUSCITATION AIRWAY OBSTRUCTION - FOREIGN BODY 8 years old 1-8 years old birth to 1 year Ventilations If unable to ventilate, reposition head and reattempt ventilation. If still unsuccessful:Tongue/Jaw lift and Finger Sweep Abdominal Thrusts Not Used Chest Thrusts Not Used Back Blows Not Used Not Used
Continue the above sequence until successful. If patient resumes effective breathing, place in recovery position. If unable to clear airway within one minute, begin transport, continue sequence enroute, and consider ALS rendezvous.
CARDIOPULMONARY RESUSCITATION Duration of Each Ventilation Pulse Check Location Compression Depth 1-rescuer CPR compression to ventilation ratio 2-rescuer CPR compression to ventilation ratio AUTOMATED EXTERNAL DEFIBRILLATION 1. Determine patient unresponsiveness and provide basic life support/CPR. 2. Check pulse. Notify Dispatcher of confirmed full arrest (or appropriate patient
status) and confirm response / ETA of EMS.
3. Initiate cardiopulmonary resuscitation if adequate manpower is available while
automatic external defibrillator (AED) is being readied and applied.
4. Press switch to analyze cardiac rhythm if necessary, and assure all personnel are
5. If shock advised and all bystanders and personnel are clear, discharge AED.
If no shock advised, continue appropriate BLS-CPR for one (1) minute, then re-evaluate patient. Follow prompts from AED
If monitor maintains “no shock advised” status, continue appropriate BLS- CPR for three (3) minutes before re-evaluation. Follow prompts from AED.
6. Check Pulse. 7. If no pulse, press switch to analyze cardiac rhythm if necessary, and assure all
8. If shock advised, discharge AED. 9. Check Pulse. 10. If no pulse, press switch to analyze cardiac rhythm if necessary, and assure all
11. If shock advised, discharge AED. 12. Check pulse. 13. If patient is still pulseless, perform BLS-CPR for one minute, then re-evaluate.
Discharge defibrillator up to three (6) more times.
14. Continue CPR as appropriate and re-advise EMS dispatcher of patient status.
SCORING SYSTEMS APGAR SCORING GLASGOW COMA SCALE
USE THE BEST PATIENT RESPONSE FOR EACH CATEGORY.
Note: Lowest possible score = 3; Highest possible score = 15
RULE OF NINES - ESTIMATING BURNS START TRIAGE
1. RPM method of identifying immediate patients;
• Respirations >30 per minute or absent until head repositioned, or • Radial pulse absent or capillary refill > 2 seconds, or • Can not follow simple commands
• Respirations present and < 30 per minute, and • Radial pulse present, and can follow simple commands
C. Minor (Green) • Anyone that can get up and walk when you instruct them to do so.
D. Deceased (Black) • Anyone not breathing after you open the airway
3. This system is limited to use in the incident where needs exceed resources
4. Frequently reassess patients and perform a more in-depth triage as more rescuers
GLOSSARY
ABORTION - The premature expulsion from the uterus of the embryo or a nonviable
ACCESSORY MUSCLES - Subordinate or dependent muscles, usually referring to
breathing without usual chest wall movement.
ALS - Advanced Life Support. AMBULATE - To walk about. APHASIA - A defect in speaking or comprehending in the normal fashion, caused by
injury or disease in the brain centers regulating speech.
APNEA - Absence of breathing. ASPHYXIA - Suffocation. AUSCULTATION -The technique of listening for and interpreting sounds that occur
within the body, usually with a stethoscope.
BILATERAL - Pertaining to both sides. BLS - Basic Life Support. BM - Bowel Movement. BRACHIAL - Pertaining to the brachial artery in the arm. BREECH BIRTH - A delivery in which the presenting part is the buttocks or foot. BRONCHITIS - Inflammation of the bronchi. BURN - An injury caused by extremes of temperature, electric current, or certain
chemicals. FIRST-DEGREE BURN - A burn affecting only the outer skin layers (red). SECOND-DEGREE BURN - A partial thickness burn penetrating beneath the
superficial skin layers, producing edema and blistering.
THIRD-DEGREE BURN - A full thickness burn, involving all layers of the skin and
underlying tissues as well, having a charred or white, leathery appearance.
CAROTID ARTERY - One of the main arteries of the neck supplying blood to the head. CENTRAL NERVOUS SYSTEM (CNS) - The brain and spinal cord. CEREBROSPINAL FLUID (CSF) - The fluid that bathes the brain and spinal cord. CEREBROVASCULAR ACCIDENT (CVA) - he sudden cessation of circulation to the
region of the brain, caused by thrombus, embolism, or hemorrhage. It is sometimes called a stroke.
CHRONIC OBSTRUCTIVE PULMONARY DISEASE (COPD) - A term comprising
chronic bronchitis, emphysema, and sometimes asthma, illnesses that cause obstructive problems in the lower airways.
COMA - A state of unconsciousness from which the patient cannot be aroused, even by
COMA POSITION - A body position which allows the unconscious patient (non-
traumatic) to breathe without obstruction from oral bleeding or drainage.
CONTRAINDICATION - Any condition which renders a particular line of treatment
CONVULSION - A violent, involuntary contraction or series of contractions of the
voluntary muscles; a "fit," a seizure.
CPR - Cardiopulmonary Resuscitation. CREPITUS - A grating sound heard and a sensation felt when the fractured ends of a
CROWNING - The stage of birth when the presenting part of the baby is visible at the
DECEREBRATE POSTURE - A posture assumed by patients with severe brain
dysfunction, characterized by extension and rotation of the arms and extension of the legs.
DECORTICATE POSTURE - A posture assumed by patients with severe brain
dysfunction, characterized by extension of the legs and flexion of the arms.
DIABETES MELLITUS - A systemic disease affecting many organs, including the
pancreas, whose failure to secrete insulin causes an inability to metabolize carbohydrate and consequent elevations in blood sugar.
DIAPHORESIS - Profuse perspiration. DOA - Dead on Arrival. DYSPNEA - Difficulty in breathing. EDEMA - The condition in which excess fluid accumulates in body tissue, manifested by
EMBOLISM - A mass (embolus, singular; emboli, plural) of solid, liquid or gaseous
material that is carried in the circulation and may lead to occlusion of blood vessels, with resultant infarction and necrosis of tissue supplied by those vessels.
EMPHYSEMA - Infiltration of any tissue by air or gas; a chronic pulmonary disease
caused by distension of the alveoli and destructive changes in the lung.
EMS - Emergency Medical Services. EMT - Emergency Medical Technician. EPIGASTRIUM - The upper central portion of the abdomen within the sternal angle. ETA - Estimated time of arrival. ETIOLOGY - The causative agent of a disease. EVISCERATION - Exposed bowel due to trauma. EXSANGUINATE - To bleed to death. F R - First Responder. FEBRILE - Characterized by fever. FLAIL CHEST - The condition in which several ribs are broken, each in at least two
places, or in which there is sternal fracture or separation of the ribs from the sternum, producing a free or floating segment of the chest wall that moves paradoxically on respiration.
FLEXION - The act of bending. GLASGOW COMA SCALE - A measurement tool used to accurately record the patient's
level of consciousness at regular intervals.
GRAND MAL SEIZURE - A generalized motor seizure.
HEAT CRAMPS - Painful muscle cramps resulting from excessive loss of salt and water
HEAT EXHAUSTION - Excessive loss of water and salt through sweating. It is
characterized by cold, clammy skin and a weak, rapid pulse.
HEAT STROKE - A life-threatening condition caused by a disturbance in the
temperature regulating mechanism. It is characterized by extreme fever, hot and dry skin, bounding pulse, and delirium or coma.
HYPERGLYCEMIA - Abnormally increased concentration of sugar in the blood. HYPERTHERMIA - Abnormally increased body temperature. HYPERVENTILATION - An increased rate and/or depth of respiration. HYPOGLYCEMIA - Abnormally diminished concentration of sugar in the blood. HYPOTHERMIA - Having a body temperature below normal. HYPOVOLEMIA - Abnormally decreased amount of blood and fluids in the body. HYPOXIA - Reduction of oxygen in body tissues below normal levels. INFARCTION - Death (necrosis) of a localized area of tissue caused by the cutting off of
INSUFFICIENCY - The condition of being inadequate to normal performance. INSULIN SHOCK - Severe hypoglycemia caused by excessive insulin dosage with
respect to sugar intake. It may be characterized by bizarre behavior, sweating, tachycardia, or coma.
LAVAGE - To wash out, or irrigate. LETHARGY - condition of drowsiness or indifference. LUNG SOUNDS - Listening for and interpreting sounds that occur within the lungs. MCI - Multiple Casualty Incident. MAST - An abbreviation for Military Anti Shock Trousers. MEDICAL DIRECTOR - Physician responsible for overseeing the medical treatment
MENSTRUATION - The process by which the uterine lining is shed each month by
women between the ages of puberty and menopause.
MISCARRIAGE - A layman's term for an abortion, or the premature expulsion of a
NECROSIS - The death of tissue, usually caused by a cessation of its blood supply. NORMAL SALINE - A solution containing 0.9% sodium chloride. OCCLUSIVE DRESSING - A watertight covering for a wound. O2 - Oxygen. PARADOXICAL RESPIRATION - The situation in which attempts to inhale cause
collapse of a portion of the chest wall instead of expansion. It is seen in flail chest.
PERINEUM - That area of the anatomy bounded anteriorly by the pubic symphysis and
PERIORAL - Around the mouth. PERIORBITAL - Around the eye.
PETIT MAL SEIZURE - A type of epileptic attack seen especially in children,
characterized by momentary loss of awareness without loss of motor tone.
PLACENTA - A vascular organ attached to the uterine wall, supplying oxygen and
nutrients to the fetus; also called the afterbirth.
PNEUMOTHORAX - Air in the pleural cavity. POSTICTAL - Referring to the period after the convulsive state of a seizure. POSTPARTUM - Occurring after childbirth, with reference to the mother. PROLAPSED CORD - A delivery in which the umbilical cord appears at the vaginal
PRONE - Lying flat with the face downward. PROPHYLAXIS - Taking measures to prevent the occurrence of a given disease of
PROTOCOL - A standardized method of treatment. PSYCHOSIS - A mental disorder causing disintegration of personality and loss of
PULMONARY EDEMA - A fluid build-up within the lungs. RESPIRATORY INSUFFICIENCY - A condition which results in inadequate oxygen and
carbon dioxide exchange in the lungs and tissues, due to disease or injury.
SHOCK - An inadequate tissue perfusion, which may be caused by pump failure
(cardiogenic shock), volume loss (hypovolemic shock), vasodilation (neurogenic shock), or any combination of these.
STATUS EPILEPTICUS - The occurrence of two or more seizures without a period of
SUBCUTANEOUS EMPHYSEMA - A condition resulting in the escape of air into the
tissues of the body, especially the chest wall, neck, and face, causing a crackling sensation on palpation of the skin.
SUPINE - Lying flat with the face upward. TACHYCARDIA - A rapid heart rate, over 100 per minute. TENSION PNEUMOTHORAX - The situation in which air enters the pleural space
causing progressive increase in intrapleural pressure, with lung collapse and impairment of circulation.
THROMBUS - A fixed clot that forms inside a blood vessel. TOXIN - A poison manufactured by bacteria or other forms of animal or vegetable life. TRACHEAL DEVIATION - A lateral shift in the position of the trachea so it no longer
TRENDELENBURG POSITION - The position in which a patient is placed on his back
TRIAGE - A system used for categorizing and sorting patients according to the severity
VITAL SIGNS - Pulse, blood pressure, respiration, skin color, and pupils.
Clinical Psychology Review 26 (2006) 17 – 31The empirical status of cognitive-behavioral therapy:Andrew C. Butler a,*, Jason E. Chapman b, Evan M. Forman c, Aaron T. Beck aa University of Pennsylvania and the Beck Institute for Cognitive Therapy and Research, United Statesb Medical University of South Carolina, United StatesReceived 20 September 2004; received in revised form 7 June 2
You may experience fatigue, dizziness or If you have any questions please ask your headaches drink plenty of fluids to relieve Polyps are little growths which arise from the lining of the bowels. Some may progress and change as they grow, therefore removal is necessary to prevent them turning cancerous. Polyp removal is achieved by looping them with a snare and cutting through the lining
 CaseEMS
CaseEMS 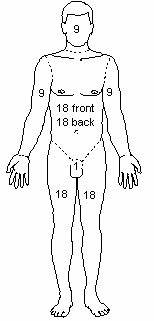
 RULE OF NINES - ESTIMATING BURNS
RULE OF NINES - ESTIMATING BURNS