Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Centadocs.com
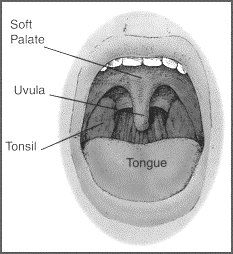
Instructions for parents 317-926-1056 800-283-1056 IMPORTANT: PLEASE READ THESE INSTRUCTIONS BEFORE SURGERY AND AGAIN AFTER SURGERY Why are tonsils and adenoids removed?
Tonsils are in the back of the throat, while adenoids are
higher and behind the nose. The two primary reasons for tonsil and/or adenoid removal are (1) recurrent infection despite antibiotic therapy and (2) difficulty breathing due to enlarged tonsils and/or adenoids. Such obstruction to breathing causes snoring and
disturbed sleep that leads to daytime sleepiness and
behavioral problems in children. In addition, there is evidence that chronic mouth breathing from large tonsils and adenoids can cause problems with facial growth and result in crooked teeth. What should I do before surgery?
• Do not give your child any pain medications except for acetaminophen (Tylenol) for 14 days prior to the
surgery, as aspirin and other pain medications can increase the risk of bleeding. Herbal supplements should also be avoided.
• Your child should not have anything to eat or drink after midnight the day before surgery, or as instructed in your pre-op letter from your doctor. This means nothing—not even water.
• If you have any questions call our office or write them down and bring them with you the day of surgery. • If your child is in school, you should plan on him staying out of school for at least a week following surgery
and possibly longer, depending on how his recovery goes.
What do I need to buy before surgery? Any liquid your child prefers to drink and other foods as suggested below in the section marked DIET. You should also have acetaminophen (Tylenol) and ibuprofen (Advil/Motrin) available. What should I expect and be prepared for after surgery? The rest of this handout will explain what to expect after surgery so that you can prepare for your child’s needs ahead of time. Please keep this information for reference during his recovery. BLEEDING: A slight amount of bleeding can occur—this is usually not serious. The most common times for bleeding to occur are within the first few hours after surgery and at 7-10 days after surgery when the scabs dissolve away from the healing wounds. A small amount of blood streaked in saliva (spit) is not cause for alarm. Have your child sit upright quietly. Cold compresses on the neck may be helpful. If the bleeding persists, or if your child is coughing or vomiting up blood, go directly to the nearest emergency room. Occasionally a return to the operating room to control the bleeding and/or an overnight stay in the hospital will be required. PAIN: It is normal for your child to complain of a very sore throat, which often can last for two weeks. He may also complain of ear, neck, or jaw pain, especially 3-5 days after surgery. This pain is not due to an infection but rather an irritation of the nerves that pass behind the tonsils. We suggest giving acetaminophen (Tylenol) or ibuprofen (Advil/Motrin) every four hours for the first 24 hours after surgery, then as needed thereafter. These can be alternated, if you desire. You will be given a prescription for stronger pain medication with codeine, which can be used as prescribed. However, codeine can cause nausea, vomiting, or constipation, so it should be used only if the Tylenol and ibuprofen are not working. Do not give aspirin or Aspergum for pain relief as it can cause bleeding. Often, the pain is made worse from mouth dryness and from not using the throat muscles. The first swallows in the morning are usually the worst. Try having the child suck on a teaspoon of ice chips (which can be flavored with juice) to stimulate saliva production and increase gentle swallowing. Sugarless chewing gum can also be helpful. This can be helpful throughout the day, before meals, and even at night when pain awakens your child. Prescription pain medicines can make your child sleepy. Once the pain medicine has been given, wait about 30 to 40 minutes, and then strongly encourage your child to drink some fluids before he falls asleep. If he is allowed to go to sleep without drinking, his throat will be very dry and his pain worse when he awakens. Ice packs against the neck are often comforting. FEVER: Fevers after surgery are not unusual. Call us if it is 102°F or higher, or if it doesn’t respond to Tylenol and ibuprofen. DIET: The single most important aspect of your child’s diet is adequate fluid intake. He can have anything he wants to eat—there are no restrictions. It is normal for him to not want to eat or drink, since swallowing is painful. However, it is essential that he have fluids to reduce pain, fever, risk of bleeding, and to promote healing. Frequent small feedings of soft foods or liquids are usually tolerated best. Make an effort to give small amounts every hour during waking hours for the first two days after surgery. Cold slushy liquids such as sherbet, sorbet, Popsicles (whole or crushed up) and slushies are excellent sources of liquid, as they not only hydrate but also soothe. Soft drinks, apple or grape juice, Jell-O, custard, pudding, Gatorade, Pedialyte, and warm (not hot) soup are also good choices. Citrus juices are best avoided, as they may burn. However, if orange juice is the only liquid you can get your child to drink, then he should drink as much as he can tolerate. As his appetite improves, encourage him to eat solid foods. Eating solid foods as soon as possible will help reduce spasm and pain by mobilizing the jaw and throat muscles. How much is enough? Output follows intake. If your child is urinating at least twice a day, he is probably not dehydrated.
However, if not, you may notice these signs of dehydration: dark urine or significantly decreased urination, lack of tears, sunken eyes, and dry skin. If any of these occur, please call. We may need to re-admit your child to the hospital and give some fluids intravenously. However, do not use needles or the hospital as a threat to get your child to drink, as this makes it seem like a place of punishment rather than a place to be helped. Rewards for drinking are often far more effective than threats of punishment. BAD BREATH: Very bad breath is to be expected for the first 7-10 days after surgery. Increased drinking may improve bad breath. As the white, filmy scabs in the throat go away, the breath will improve. VOMITING: Vomiting once or twice after surgery is not unusual and is usually related to the anesthesia or to taking codeine. If your child vomits, wait 30 minutes and then try very small amounts of clear liquids until tolerated. Other liquids and soft foods can be added to the diet once nausea has resolved. If repeated vomiting occurs, call the office. ACTIVITY: Your child will limit his own activity for the first few days. You should encourage him to at least get up and out of bed, if even to rest quietly in another room. Most children stay out of school following surgery for at least a week, but your child may return to school earlier if he feels ready to do so. Avoid running, sports, playing of wind instruments, gym class, or other strenuous activities for two weeks. HELPFUL HINTS: Cover pillow cases with an old towel, since drooling during sleep is common. Snoring may be loud for the first few nights after surgery due to swelling, but will get better as the swelling goes down. Keeping the head elevated is often helpful, as is having a vaporizer or humidifier near the bed. QUESTIONS: Our office personnel and your doctor are eager to support you through this process. We always have a doctor on-call. Please do not hesitate to call if you have questions or problems, and remember, be sure to call us in any of the following circumstances:
• Bleeding (as noted above) • Fever 102° F or higher, or fever that does not respond to Tylenol or ibuprofen
• Dehydration • Constipation that becomes a problem • If your doctor instructs you to, make a follow-up appointment to be seen in __________ weeks.
International Journal of Gynecology and Obstetrics 86 (2004) 351–357Human chorionic gonadotrophin and progesterone levels inG. Condousa , *, C. Lub, S.V. Van Huffelb, D. Timmermanc, T. Bournea Pregnancy, Gynaecological Ultrasound and MAS Unit, Department of Obstetrics & Gynaecology, St George’s Hospital Medical School, Cranmere Terrace, London SW17 0RE, UK of Electrical Engineerin
Marinoff’s Therapy: A Critique of His Books on Philosophical Practice Shlomit C. Schuster Shlomit C. Schuster is a practicing philosophical counselor. She has written several scholarly articles on philosophical counseling and is the author of Philosophy Practice: An Alternative to Counseling and Psychotherapy (Praeger, 1999) and The Philosopher’s Autobiography: A Qualitativ
 Instructions for parents
Instructions for parents