Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Cmeinstitute.com
Pilot RCT of SSRI vs Bupropion: Effects on Suicidal Behavior, Ideation and Mood in MDD with Past Attempt or Current Ideation
Michael F. Grunebaum; Steven Ellis; Naihua Duan; Ainsley Burke;
This poster is presented in columns for online reading. You may also see the poster in it
Pilot RCT of SSRI vs Bupropion: Effects on Suicidal Behavior, Ideation and Mood in MDD with Past Attempt or Current Ideation Grunebaum MF, Ellis SP, Duan N, Burke AK, Oquendo MA, Mann JJ NYSPI/Columbia University Medical Center ABSTRACT
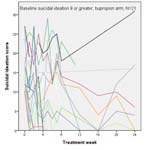
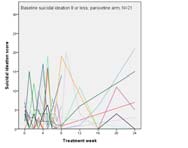
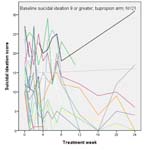
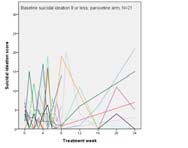
• Worsening SI: in Pts at 75th percentile of SSI “Spaghetti plots” of SSI vs Time, by Tx and median split of SSI :
RCT of paroxetine (N = 36) vs bupropion (N = 38) in DSM IV MDD towards protective effect of PXT at Wk 1: (est = 1.77, SE = 1 line = 1 patient. with past suicide attempt or current suicidal ideation. Acute (8
0.94, df = 121.4, t = 1.89, p = .06, OR = 5.9, 95% CI = 0.94 to
weeks) and continuation treatment (up to 16 weeks).
Outcomes: suicidal events and ideation; secondary outcome: non- suicidal mood Sxs. Treatment was not associated with time to a suicidal event. No treatment main effect or treatment x time
• Non-suicidal depressive symptoms: PXT superior in Pts interaction on suicidal ideation or non-suicidal depressive
most depressed at baseline (est = -0.46; p = 0.02)
symptoms was found. Exploratory model selection showed modest advantages for PXT for non-suicidal depressive
• Only predictor of SI in weeks 8-24 was SSIBL
symptoms (p = 0.02), and for suicidal ideation (p = 0.03), with benefit increasing with baseline severity. Patients with greater
• Attrition Wk 1-8 32%: 9/36 PXT and 15/38 BUP subjects did baseline severity appeared to experience greater acute
not complete 8 weeks of randomized treatment. Overall, 29/38
improvement in suicidal ideation and non-suicidal depressive symptoms with PXT compared to BUP. If confirmed by future
(76%) on BUP and 24/36 (67%) on PXT did not complete 24
studies, this would favor first use of PXT or other SSRI in suicidal
Scatterplots of SSI vs Time, by Tx and median split of SSI ; LOESS lines. = 8 or less = 9 or greater
• No differences by Tx in: time to last outcome assessment,
AIM / HYPOTHESIS
adherence; side effect intensity; proportion prescribed zolpidem
Compare serotonergic vs. non-serotonergic
antidepressant on suicidal behavior/ideation in higher risk MDD (h/o attempt or current SI)
• BZD dose (mg) 2x higher in BUP (PXT = 1.8±1.4, BUP = Hypothesis 1: Fewer suicidal events (attempts or
3.6±2.8; U = 153.0, p = .03).
increased ideation requiring change in treatment) on PXT . CONCLUSIONS Hypothesis 2: Greater reduction in SI on PXT.
•RCT in this sample is feasible, can yield useful findings.
•Exploratory model selection showed PXT reduced SI more than BUP in patients with higher SSI
• ELIGIBILITY: 18-75yo, MDD with HAM17≥16 plus
past suicide attempt or current SI, or both
•SSI scale: “weak” vs “moderate to strong” desire to attempt
• SI threshold: HDRS-SI ≥ 2 , “wishes to be dead or
suicide (item 4) is 1 point diff; no plans vs “definite plans” for
has any thoughts of possible death to self”
BASELINE: No differences by group in Age, Sex, Race, Education, Employed,
suicide (item 18) is 2 point diff(Beck et al. 1979).
Inpatient, Ham17, #past MDEs, length current MDE, #past antidepressant trials,
• EXCLUSIONS: bipolar, psychosis, AN/BN, SSRI/BUP
Cluster B co-morbidity, lifetime SUD, SSI, h/o past attempt
•Carpenter et al. JCP 2011 meta-analysis: 1) PXT vs pbo: 2)
for other indications (e.g. anxiety), drug/EtOH
Retrospective; 3) most trials excluded suicidal patients; 4)
dependence within 6m, unstable medical illness,
10 suicidal events: 2 attempts, neither w/serious injury. Tx not associated with
we stratified by prior attempt and inpatient; 5) less rating-
contraindication to either drug, non-response to 3
time to first event (log rank chi sq=0.17, df=1, p=.68). scale based treatment emergent suicidal behavior or
SSRIs, PXT, or BUP in last 2y , pregnancy, capacity
ideation in PXT-treated c/w pbo across all indications in Suicidal Ideation: Tx x time NS (p=.27, est=0.81); Tx main effect NS (p=.07,
• INTERVENTION: Triple-blind, randomized to
•Limitations of our study: sample size, exploratory finding, Exploratory Model Selection (BIC): SSI
attrition, no differential Tx effects in continuation phase.
Optional increase to PXT 50mg or BUP 450mg
Tx x SSI : SE=0.14, df=59.9, t=-2.17, p=.03, est=-0.29 (-0.6 to -0.02)
• ASSESSMENTS: qWk x 8 weeks ; qMo x 16 weeks Disclosure: PXT and BUP donated by GSK to defray costs first 3 years of study, purchased with grant thereafter. Dr. Mann support for unrelated brain MODEL PREDICTIONS OF SUICIDAL IDEATION:
imaging studies from GSK and Novartis. Dr. Duan support from Pfizer for
• STATISTICS:
unrelated health services research. GSK, Novartis and Pfizer were not involved
in the design or execution of the study, had no access to the data or had any
• K-M survival analysis of time to first suicidal “event”
• 3.7 points lower on PXT at Wk 1 (p = 0.009) Acknowledgments:
• GLS regression of follow-up score on Beck SSI
NARSAD Young Investigator grant (mfg) and NIMH
• 2.5 points lower on PXT at Wk 4 (p = 0.03) Contact: mfg14@columbia.edu Pilot RCT of SSRI vs Bupropion: Effects on Suicidal Behavior, Ideation and Mood in MDD with Past Attempt or Current Ideation Grunebaum MF, Ellis SP, Duan N, Burke AK, Oquendo MA, Mann JJ NYSPI/Columbia University Medical Center ABSTRACT
• Worsening SI: in Pts at 75th percentile of SSI “Spaghetti plots” of SSI vs Time, by Tx and median split of SSI :
RCT of paroxetine (N = 36) vs bupropion (N = 38) in DSM IV MDD towards protective effect of PXT at Wk 1: (est = 1.77, SE = 1 line = 1 patient. with past suicide attempt or current suicidal ideation. Acute (8
0.94, df = 121.4, t = 1.89, p = .06, OR = 5.9, 95% CI = 0.94 to
weeks) and continuation treatment (up to 16 weeks).
Outcomes: suicidal events and ideation; secondary outcome: non- suicidal mood Sxs. Treatment was not associated with time to a suicidal event. No treatment main effect or treatment x time
• Non-suicidal depressive symptoms: PXT superior in Pts interaction on suicidal ideation or non-suicidal depressive
most depressed at baseline (est = -0.46; p = 0.02)
symptoms was found. Exploratory model selection showed modest advantages for PXT for non-suicidal depressive
• Only predictor of SI in weeks 8-24 was SSIBL
symptoms (p = 0.02), and for suicidal ideation (p = 0.03), with benefit increasing with baseline severity. Patients with greater
• Attrition Wk 1-8 32%: 9/36 PXT and 15/38 BUP subjects did baseline severity appeared to experience greater acute
not complete 8 weeks of randomized treatment. Overall, 29/38
improvement in suicidal ideation and non-suicidal depressive symptoms with PXT compared to BUP. If confirmed by future
(76%) on BUP and 24/36 (67%) on PXT did not complete 24
studies, this would favor first use of PXT or other SSRI in suicidal
Scatterplots of SSI vs Time, by Tx and median split of SSI ; LOESS lines. = 8 or less = 9 or greater
• No differences by Tx in: time to last outcome assessment,
AIM / HYPOTHESIS
adherence; side effect intensity; proportion prescribed zolpidem
Compare serotonergic vs. non-serotonergic
antidepressant on suicidal behavior/ideation in higher risk MDD (h/o attempt or current SI)
• BZD dose (mg) 2x higher in BUP (PXT = 1.8±1.4, BUP = Hypothesis 1: Fewer suicidal events (attempts or
3.6±2.8; U = 153.0, p = .03).
increased ideation requiring change in treatment) on PXT . CONCLUSIONS Hypothesis 2: Greater reduction in SI on PXT.
•RCT in this sample is feasible, can yield useful findings.
•Exploratory model selection showed PXT reduced SI more than BUP in patients with higher SSI
• ELIGIBILITY: 18-75yo, MDD with HAM17≥16 plus
past suicide attempt or current SI, or both
•SSI scale: “weak” vs “moderate to strong” desire to attempt
• SI threshold: HDRS-SI ≥ 2 , “wishes to be dead or
suicide (item 4) is 1 point diff; no plans vs “definite plans” for
has any thoughts of possible death to self”
BASELINE: No differences by group in Age, Sex, Race, Education, Employed,
suicide (item 18) is 2 point diff(Beck et al. 1979).
Inpatient, Ham17, #past MDEs, length current MDE, #past antidepressant trials,
• EXCLUSIONS: bipolar, psychosis, AN/BN, SSRI/BUP
Cluster B co-morbidity, lifetime SUD, SSI, h/o past attempt
•Carpenter et al. JCP 2011 meta-analysis: 1) PXT vs pbo: 2)
for other indications (e.g. anxiety), drug/EtOH
Retrospective; 3) most trials excluded suicidal patients; 4)
dependence within 6m, unstable medical illness,
10 suicidal events: 2 attempts, neither w/serious injury. Tx not associated with
we stratified by prior attempt and inpatient; 5) less rating-
contraindication to either drug, non-response to 3
time to first event (log rank chi sq=0.17, df=1, p=.68). scale based treatment emergent suicidal behavior or
SSRIs, PXT, or BUP in last 2y , pregnancy, capacity
ideation in PXT-treated c/w pbo across all indications in Suicidal Ideation: Tx x time NS (p=.27, est=0.81); Tx main effect NS (p=.07,
• INTERVENTION: Triple-blind, randomized to
•Limitations of our study: sample size, exploratory finding, Exploratory Model Selection (BIC): SSI
attrition, no differential Tx effects in continuation phase.
Optional increase to PXT 50mg or BUP 450mg
Tx x SSI : SE=0.14, df=59.9, t=-2.17, p=.03, est=-0.29 (-0.6 to -0.02)
• ASSESSMENTS: qWk x 8 weeks ; qMo x 16 weeks Disclosure: PXT and BUP donated by GSK to defray costs first 3 years of study, purchased with grant thereafter. Dr. Mann support for unrelated brain MODEL PREDICTIONS OF SUICIDAL IDEATION:
imaging studies from GSK and Novartis. Dr. Duan support from Pfizer for
• STATISTICS:
unrelated health services research. GSK, Novartis and Pfizer were not involved
in the design or execution of the study, had no access to the data or had any
• K-M survival analysis of time to first suicidal “event”
• 3.7 points lower on PXT at Wk 1 (p = 0.009) Acknowledgments:
• GLS regression of follow-up score on Beck SSI
NARSAD Young Investigator grant (mfg) and NIMH
• 2.5 points lower on PXT at Wk 4 (p = 0.03) Contact: mfg14@columbia.edu Pilot RCT of SSRI vs Bupropion: Effects on Suicidal Behavior, Ideation and Mood in MDD with Past Attempt or Current Ideation Grunebaum MF, Ellis SP, Duan N, Burke AK, Oquendo MA, Mann JJ NYSPI/Columbia University Medical Center ABSTRACT
• Worsening SI: in Pts at 75th percentile of SSI “Spaghetti plots” of SSI vs Time, by Tx and median split of SSI :
RCT of paroxetine (N = 36) vs bupropion (N = 38) in DSM IV MDD towards protective effect of PXT at Wk 1: (est = 1.77, SE = 1 line = 1 patient. with past suicide attempt or current suicidal ideation. Acute (8
0.94, df = 121.4, t = 1.89, p = .06, OR = 5.9, 95% CI = 0.94 to
weeks) and continuation treatment (up to 16 weeks).
Outcomes: suicidal events and ideation; secondary outcome: non- suicidal mood Sxs. Treatment was not associated with time to a suicidal event. No treatment main effect or treatment x time
• Non-suicidal depressive symptoms: PXT superior in Pts interaction on suicidal ideation or non-suicidal depressive
most depressed at baseline (est = -0.46; p = 0.02)
symptoms was found. Exploratory model selection showed modest advantages for PXT for non-suicidal depressive
• Only predictor of SI in weeks 8-24 was SSIBL
symptoms (p = 0.02), and for suicidal ideation (p = 0.03), with benefit increasing with baseline severity. Patients with greater
• Attrition Wk 1-8 32%: 9/36 PXT and 15/38 BUP subjects did baseline severity appeared to experience greater acute
not complete 8 weeks of randomized treatment. Overall, 29/38
improvement in suicidal ideation and non-suicidal depressive symptoms with PXT compared to BUP. If confirmed by future
(76%) on BUP and 24/36 (67%) on PXT did not complete 24
studies, this would favor first use of PXT or other SSRI in suicidal
Scatterplots of SSI vs Time, by Tx and median split of SSI ; LOESS lines. = 8 or less = 9 or greater
• No differences by Tx in: time to last outcome assessment,
AIM / HYPOTHESIS
adherence; side effect intensity; proportion prescribed zolpidem
Compare serotonergic vs. non-serotonergic
antidepressant on suicidal behavior/ideation in higher risk MDD (h/o attempt or current SI)
• BZD dose (mg) 2x higher in BUP (PXT = 1.8±1.4, BUP = Hypothesis 1: Fewer suicidal events (attempts or
3.6±2.8; U = 153.0, p = .03).
increased ideation requiring change in treatment) on PXT . CONCLUSIONS Hypothesis 2: Greater reduction in SI on PXT.
•RCT in this sample is feasible, can yield useful findings.
•Exploratory model selection showed PXT reduced SI more than BUP in patients with higher SSI
• ELIGIBILITY: 18-75yo, MDD with HAM17≥16 plus
past suicide attempt or current SI, or both
•SSI scale: “weak” vs “moderate to strong” desire to attempt
• SI threshold: HDRS-SI ≥ 2 , “wishes to be dead or
suicide (item 4) is 1 point diff; no plans vs “definite plans” for
has any thoughts of possible death to self”
BASELINE: No differences by group in Age, Sex, Race, Education, Employed,
suicide (item 18) is 2 point diff(Beck et al. 1979).
Inpatient, Ham17, #past MDEs, length current MDE, #past antidepressant trials,
• EXCLUSIONS: bipolar, psychosis, AN/BN, SSRI/BUP
Cluster B co-morbidity, lifetime SUD, SSI, h/o past attempt
•Carpenter et al. JCP 2011 meta-analysis: 1) PXT vs pbo: 2)
for other indications (e.g. anxiety), drug/EtOH
Retrospective; 3) most trials excluded suicidal patients; 4)
dependence within 6m, unstable medical illness,
10 suicidal events: 2 attempts, neither w/serious injury. Tx not associated with
we stratified by prior attempt and inpatient; 5) less rating-
contraindication to either drug, non-response to 3
time to first event (log rank chi sq=0.17, df=1, p=.68). scale based treatment emergent suicidal behavior or
SSRIs, PXT, or BUP in last 2y , pregnancy, capacity
ideation in PXT-treated c/w pbo across all indications in Suicidal Ideation: Tx x time NS (p=.27, est=0.81); Tx main effect NS (p=.07,
• INTERVENTION: Triple-blind, randomized to
•Limitations of our study: sample size, exploratory finding, Exploratory Model Selection (BIC): SSI
attrition, no differential Tx effects in continuation phase.
Optional increase to PXT 50mg or BUP 450mg
Tx x SSI : SE=0.14, df=59.9, t=-2.17, p=.03, est=-0.29 (-0.6 to -0.02)
• ASSESSMENTS: qWk x 8 weeks ; qMo x 16 weeks Disclosure: PXT and BUP donated by GSK to defray costs first 3 years of study, purchased with grant thereafter. Dr. Mann support for unrelated brain MODEL PREDICTIONS OF SUICIDAL IDEATION:
imaging studies from GSK and Novartis. Dr. Duan support from Pfizer for
• STATISTICS:
unrelated health services research. GSK, Novartis and Pfizer were not involved
in the design or execution of the study, had no access to the data or had any
• K-M survival analysis of time to first suicidal “event”
• 3.7 points lower on PXT at Wk 1 (p = 0.009) Acknowledgments:
• GLS regression of follow-up score on Beck SSI
NARSAD Young Investigator grant (mfg) and NIMH
• 2.5 points lower on PXT at Wk 4 (p = 0.03) Contact: mfg14@columbia.edu
El Cerrito Police Department Memorandum Subject: Recent Information Regarding Marijuana and Dispensaries As we have discussed, I have continued to follow current events as they relate to Marijuana and Dispensary related issues. I have assembled some of the information I have collected into four categories, immerging trends, secondary effects, ordinance related stories and medic
Hackthorn Church of England Primary School www.hackthorn.lincs.sch.uk Dear Parents and Friends Illness There has been a lot of illness about this winter and it seems to be continuing into summer. There seems to be a ‘lively’ bug in the area at the moment. Many children and adults have been sick over the last couple of weeks. This began at the be
 Pilot RCT of SSRI vs Bupropion: Effects on
Pilot RCT of SSRI vs Bupropion: Effects on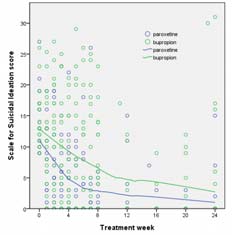


 Pilot RCT of SSRI vs Bupropion: Effects on Suicidal Behavior, Ideation and
Pilot RCT of SSRI vs Bupropion: Effects on Suicidal Behavior, Ideation and 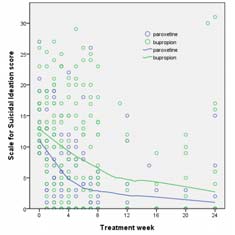




 Pilot RCT of SSRI vs Bupropion: Effects on Suicidal Behavior, Ideation and
Pilot RCT of SSRI vs Bupropion: Effects on Suicidal Behavior, Ideation and 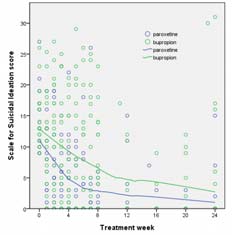


 Pilot RCT of SSRI vs Bupropion: Effects on Suicidal Behavior, Ideation and
Pilot RCT of SSRI vs Bupropion: Effects on Suicidal Behavior, Ideation and