Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Dev1.adf.org.hk
E m e r g i n g T r e a t m e n t s a n d T e c h n o l o g i e s O R I G I N A L Development and Validation of Stroke Risk Equation for Hong Kong Chinese Patients With Type 2 Diabetes The Hong Kong Diabetes Registry ILIN YANG, PHD RAMON R. LYU, PHD ING-YEE SO, FRCP DONALD D. YIN, PHD Stroke is among the most common LICE P.S. KONG, FRCP CLIVE S. COCKRAM, MD HUNG-SHUN HO, PHD PETER C.Y. TONG, PHD
dence of stroke and related mortality than
HRISTOPHER W.K. LAM, PHD VIVIAN WONG, MD ICHARD J. STEVENS, PHD JULIANA C.N. CHAN, MD
Health Organization MONICA project(2). Diabetic patients have a two- to five-fold increased risk of stroke, in part due to
OBJECTIVE — We sought to develop stroke risk equations for Chinese patients with type 2
interactions between multiple risk factors
(3). The Framingham Study (4) and U.K. Prospective Diabetes Study (UKPDS) (5)
RESEARCH DESIGN AND METHODS — A total of 7,209 Hong Kong Chinese type 2
diabetic patients without a history of stroke at baseline were analyzed. The data were randomlyand evenly divided into the training subsample and the test subsample. In the training sub-
sample, stepwise Cox models were used to develop the risk equation. Validation of the U.K.
Prospective Diabetes Study (UKPDS) stroke risk engine and the current stroke equation was
performed in the test dataset. The life-table method was used to check calibration, and the area
under the receiver operating characteristic curve (aROC) was used to check discrimination.
cruited from a workforce (6), there is cur-rently no risk equation applicable to
RESULTS — A total of 372 patients developed incident stroke during a median of 5.37 years
(interquartile range 2.88 –7.78) of follow-up. Age, A1C, spot urine albumin-to-creatinine ratio
spite this number being projected to 42.3
(ACR), and history of coronary heart disease (CHD) were independent predictors. The perfor-
million by 2030 (7). In this study, we val-
mance of the UKPDS stroke engine was suboptimal in our cohort. The newly developed risk
idate and develop stroke risk equations to
equation defined by these four predictors had adequate performance in the test subsample. Thepredicted stroke-free probability by the current equation was within the 95% CI of the observed
predict first stroke in Chinese type 2 dia-
probability. The aROC was 0.77 for predicting stroke within 5 years. The risk score was com-
puted as follows: 0.0634 ϫ age (years) ϩ 0.0897 ϫ A1C ϩ 0.5314 ϫ log (ACR) (mg/mmol)
ϩ 0.5636 ϫ history of CHD (1 if yes). The 5-year stroke probability can be calculated by: 1 Ϫ0.9707EXP (Risk Score Ϫ 4.5674). RESEARCH DESIGN AND CONCLUSIONS — Although the risk equation performed reasonably well in Chinese type METHODS — Since 1995, all newly
2 diabetic patients, external validation is required in other populations.
referred diabetic patients to the Prince ofWales Hospital in Hong Kong underwent
Diabetes Care 30:65–70, 2007
comprehensive assessments of complica-tions and risk factors based on the Euro-pean DiabCare protocol (7a). Patientswith hospital admissions within 6 – 8
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
From the 1Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Hong Kong,
China; the 2Li Ka Shing Institute of Health Sciences, The Chinese University of Hong Kong, Hong Kong,China; the 3Department of Chemical Pathology, The Chinese University of Hong Kong, Hong Kong, China;
lyzed patients had a history of stroke. Pa-
the 4Oxford Centre for Diabetes, Endocrinology, and Metabolism, University of Oxford, Oxford, U.K.; the
5Nuffield Department of Clinical Medicine, University of Oxford, Oxford, U.K.; 6Worldwide Outcomes
Research, Merck & Co., Inc., Whitehouse Station, New Jersey; and the 7Hospital Authority Head Office,
Address correspondence and reprint requests to Professor Juliana C.N. Chan, Department of Medicine
and Therapeutics, The Chinese University of Hong Kong, The Prince of Wales Hospital, Shatin, NT, Hong
ment of insulin within 1 year of diagnosis
Kong SAR, China. E-mail: jchan@cuhk.edu.hk.
Received for publication 19 June 2006 and accepted in revised form 16 October 2006. Abbreviations: ACR, albumin-to-creatinine ratio; ARB, angiotensin II receptor blocker; aROC, area
under the receiver operating characteristic curve; CHD, coronary heart disease; eGFR, estimated glomerularfiltration rate; SBP, systolic blood pressure; UKPDS, U.K. Prospective Diabetes Study.
tee, and written informed consent was ob-
A table elsewhere in this issue shows conventional and Syste`me International (SI) units and conversion
2007 by the American Diabetes Association. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be herebymarked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
DIABETES CARE, VOLUME 30, NUMBER 1, JANUARY 2007
Risk equation for stroke in type 2 diabetes
glucose, A1C, lipid profile (total choles-
terol, HDL cholesterol, and triglycerides
analysis. Patients with transient cerebral
nal and liver functions. A sterile, random,
ischemia (code 435) were not included.
the albumin-to-creatinine ratio (ACR).
Details of assessment methods, laboratory
count observation time and censoring. RESULTS — Between 1995 and 2005,
the training data (n ϭ 3,652) and test data
(n ϭ 3,559). Cox proportional hazard re-
type 1 diabetes (n ϭ 332), uncertain type
gression with the stepwise algorithm (P Ͻ
1 diabetes status (n ϭ 5), non-Chinese or
ated Modification of Diet in Renal Disease
0.05 for entry and stay) was used to select
unknown nationality (n ϭ 49), and past
predictors at baseline for incident stroke.
history of stroke (n ϭ 325) were ex-
(0.742 if female), where SCR is serum cre-
diabetic patients were included in the fi-
smoking status, history of coronary heart
teristics of patients with and without in-
of foot pulses, confirmed by an ankle-to-
cident stroke. In this cohort, the median
(46 – 67) and median disease duration 5
through dilated pupils were performed.
total-to-HDL cholesterol ratio, A1C, sys-
changes due to diabetes, laser scars, or a
5.16% of patients (n ϭ 372) developed
globin. In developing the current predict-
stroke was 9.66 (95% CI 8.69 –10.64) per
(stroke: 5.18% or 190) and 3,541 (stroke:
history was defined as having a history of
5.14% or 182) patients, respectively.
During the follow-up period, 705 patients
or stress test, myocardial infarction, an-
gina coronary artery bypass graft surgery,
stroke (among the 372 stroke events).
1 Ϫ S(j)EXP (Risk Score Ϫ Mean of the Risk Score),
where X1, X2, . . . , Xp are baseline predic-
tors and 1, 2, . . . , p are, respectively,
the estimated coefficients of baseline pre-
stroke risk engine are listed in Table 2. Of
dictors 1 to p, and S(j) is the survival func-
tion over j years when the risk score takes
sex, current smoking status, and total-to-
inhibitors (statins) (10) and blockers of
cant. In the stepwise algorithm, log10 ACR
(11) reduced the risk of stroke by Ͼ20%.
lected as significant predictors of stroke,
(codes 430 – 434 and 436) or deaths from
was not selected by the new model. In the
stroke (codes 430 – 434 and 436 – 438).
(ARB), other antihypertensive drugs, oral
nese patients with type 2 diabetes, i.e., the
while all others were classified as ischemic
was performed in the test subsample. Cal-
stroke. All diagnoses of stroke were con-
ibration was checked using the same life-
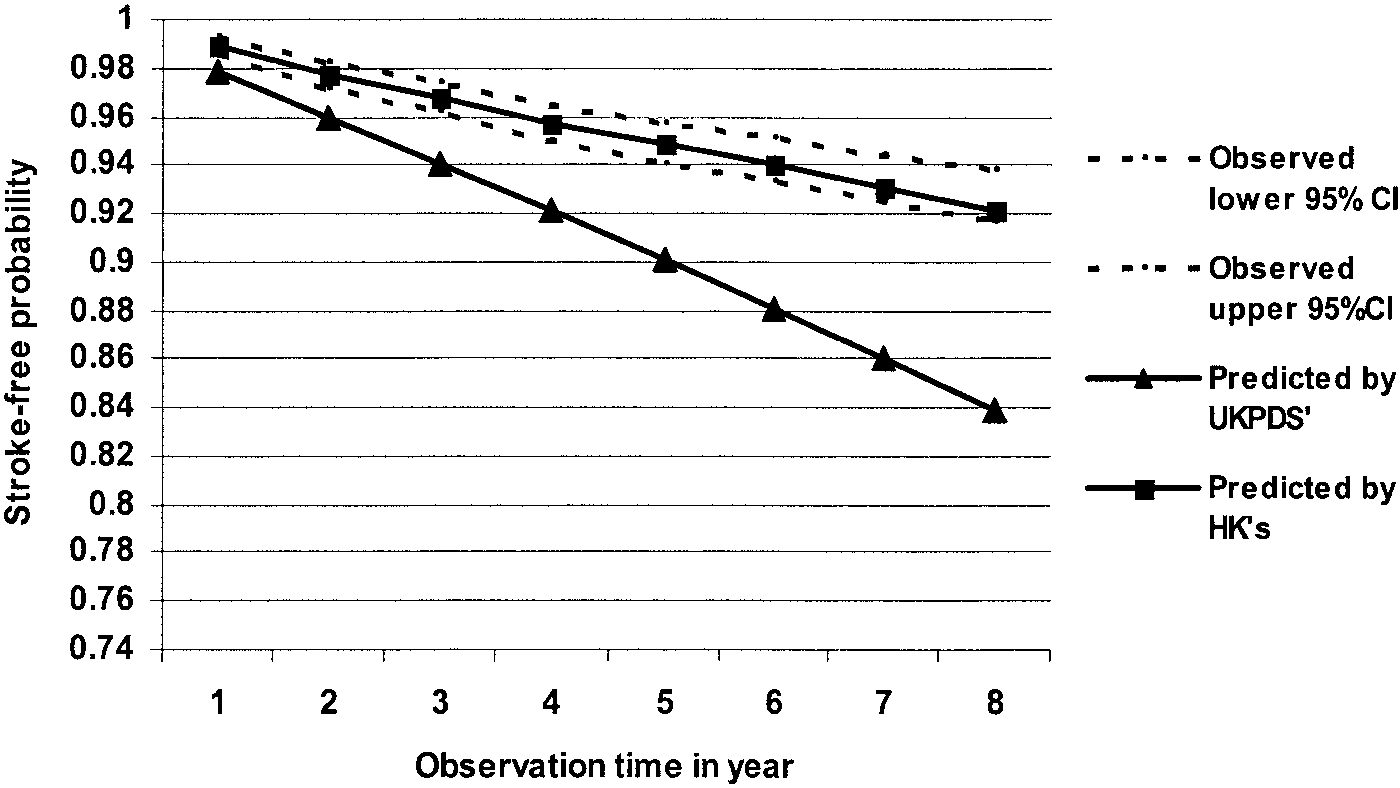
CI of the observed curve (Fig. 1). The pre-
firmed by the attending physician on dis-
dicted stroke probabilities (or stroke-free
probability) by the new stroke risk equa-
under the receiver operating characteris-
guidelines of the hospital authority. Only
tic curve (aROC) was utilized to indicate
DIABETES CARE, VOLUME 30, NUMBER 1, JANUARY 2007
Yang and Associates Table 1—Baseline clinical and biochemical characteristics of 7,209 Chinese type 2 diabetic patients with no history of stroke divided according to the development of first stroke during a
in this cohort was 0.588 (95% CI 0.549 –
median follow-up of 5.37 years
0.626). The unadjusted aROC for the newrisk equation was 0.749 (0.716 – 0.782). Taking into consideration follow-up time
RESEARCH DESIGN AND METHODS, the risk equa-
tion for predicting the first stroke event can
mates of models 1 and 2 listed in Table 2.
score ϭ 0.0634 ϫ age (years) ϩ 0.0897 ϫ
ϩ 0.5636 ϫ history of CHD (1, if yes; 0,
otherwise); the 5-year stroke probability ϭ
1 Ϫ 0.9707EXP (Risk Score Ϫ 4.5674). At the cut-
off point of Ն5.3099 for the risk score, cor-
over 5 years of follow-up, the sensitivity was
65.7% and specificity 74.9%. Sensitivities
and specificities for other cutoff points are
The predictive ability of the current risk
equation for hemorrhagic stroke and isch-
emic stroke was further estimated by using
Use of oral antidiabetes drugs at baseline
points in the test subsample. Using the risk
Use of antihypertensive drugs at baseline
rhagic stroke (n ϭ 32) and ischemic
stroke (n ϭ 150) were 0.770 and 0.785,
respectively, for 5 years of follow-up. CONCLUSIONS — In this prospec-
Data are percent or median (interquartile range) unless otherwise indicated. eGFR was from the glomerular
filtration rate from the modified Modification of Diet in Renal Disease formula. *Derived from 2 test.
†Derived from Wilcoxon two-sample test. ‡Data for 1,271 patients (stroke events ϭ 82) who enrolled before1 December 1996 were not available. ACEI, ACE inhibitor; DBP, diastolic blood pressure; LLD, lipid-
in Chinese type 2 diabetic patients due to
different risk profiles. Thus, there is aneed to develop a Chinese-relevant riskequation to predict incident stroke using
Table 2—Parameter estimates of the risk equation for Hong Kong Chinese type 2 diabetic patients and reestimated hazard ratios of the predictors used by the UKPDS stroke engine in the training subsample
Current smoking status (1 if yes; 0 otherwise)
DIABETES CARE, VOLUME 30, NUMBER 1, JANUARY 2007
Risk equation for stroke in type 2 diabetes
study (6) consisting of a small cohort ofChinese male steel workers (n ϭ 4,400),the aROC was 0.78 and 0.82 for ischemicand hemorrhage stroke, respectively. However, the 95% CIs were not reported. Besides, the event rate was relatively lowin this community cohort with only 49ischemic strokes and 33 hemorrhagicstrokes in the training subsample and 21ischemic strokes and 15 hemorrhagicstrokes in the validation subsample (6). This is compared with 372 strokes (190 inthe training subsample and 182 in the testsubsample) in our cohort.
tures with that developed from theUKPDS (5) and a Chinese cohort of steelworkers (6), all of which used commonly
Figure 1—The predicted stroke-free probabilities by the UKPDS stroke engine and the Hong Kong(HK) Chinese stroke risk score, as well as the 95% CIs of the observed stroke-free probability over8 years of observation in the test dataset.
of seven predictors (age, sex, smoking sta-tus, total-to-HDL cholesterol ratio, SBP,
for periodic assessments. These risk pre-
ventricular hypertrophy. The inclusion of
22 additional nontraditional risk factors
and markers of subclinical atherosclerotic
status). Our equation consists of four pre-
diseases, such as BMI, waist-to-hip ratio,
compared with 0.61– 0.74 for other risk
including smoking status, sex, and total-
that have only minor contributions to the
to-HDL cholesterol ratio, were not signif-
icant in the analysis, whereas the effect of
overfitting the risk equation (15). It may
(14), a basic model of stroke equation was
also increase the probability of inaccuracy
diabetic population has a very high prev-
Table 3—Sensitivity, specificity, and positive predictive values in the test data at selected risk scores and their corresponding 5-year stroke probabilities 5.3099†
*Calculated using the risk score and 5-year stroke probability equation. †The suggested cutoff point.
DIABETES CARE, VOLUME 30, NUMBER 1, JANUARY 2007
Yang and Associates
1996), use of aspirin was not included as
4. D’Agostino RB, Wolf PA, Belanger AJ, Kan-
a predictor for stroke (P ϭ 0.6890). Sec-
nel WB: Stroke risk profile: adjustment for
ond, although atrial fibrillation is a risk
antihypertensive medication: the Framing-
factor for stroke (24), it has been included
ham Study. Stroke 25:40 – 43, 1994
in some (25) but not all stroke risk equa-
5. Kothari V, Stevens RJ, Adler AI, Stratton
UKPDS 60: risk of stroke in type 2 diabe-
factors for cardiovascular and renal dis-
et al. (25) also reported that inclusion of
Diabetes Study risk engine. Stroke 33:
cluding atrial fibrillation did not signifi-
6. Zhang XF, Attia J, D’Este C, Yu XH, Wu
cantly improve the predicting accuracy of
XG: A risk score predicted coronary heart
tive effects of these risk factors. Although
stroke risk equations. Besides, the preva-
disease and stroke in a Chinese cohort.
lence of atrial fibrillation in the diabetic
J Clin Epidemiol 58:951–958, 2005
7. Wild S, Roglic G, Green A, Sicree R, King
has been reported (19,20), renal function
H: Global prevalence of diabetes: esti-mates for the year 2000 and projections
for 2030. Diabetes Care 27:1047–1053,
study, only baseline measurements of risk
factors were used to develop and validate
7a.Piwernetz K, Home PD, Snorgaard O, Ant-
in the stroke equation. This may be due to
buminuria as an expression of endothelial
tee: Monitoring the targets of the St. Vin-
equation to predict stroke in Chinese type
2 diabetic patients. It is noteworthy that
the DiabCare initiative. Diabet Med10:371–377, 1993
general populations (4,14) but not in the
may not adequately predict the event risk
type of diabetes. Diabetes Care 8:114 –
(5). The use of antihypertensive drugs, in-
incidences of the event of interest. How-
ever, the ranking may still be appropriate
(26). Thus, further validation is required
univariate Cox models in our patients but
blood cell count is associated with macro-
not selected in the stepwise algorithm.
Chinese patients with type 2 diabetes.
study, the effects of drugs on stroke were
Acknowledgments — This study was par-
10. Colhoun HM, Betteridge DJ, Durrington
ables. In this respect, the efficacy of ARB
tially supported by a Merck Sharp & Dohme
Foundation for Research and Development in
Menys V, Fuller JH: Primary prevention of
firmed in randomized clinical trials (16).
Diabetes, established under the auspices of the
Chinese University of Hong Kong. R.J.S. was
stratification and prediction of clinical
of Health, for her assistance in data retrieval
trolled trial. Lancet 364:685– 696, 2004
events (21). This periodic assessment may
Julius S, Beevers G, de Faire U, Fyhrquist
especially in clinical settings where close
References
Pedersen O, Lindholm LH, Nieminen MS,Omvik P, Oparil S, Wedel H: Cardiovas-
1. Murray CJ, Lopez AD: Mortality by cause
for eight regions of the world: Global Bur-
den of Disease Study. Lancet 349:1269 –
specialist physicians in carrying out these
randomised trial against atenolol. Lancet
12. Hanley JA, McNeil BJ: The meaning and
and determinants in cardiovascular diseases
use of the area under a receiver operating
in China. Part i. Morbidity and mortality
characteristic (ROC) curve. Radiology
patients did not have lipid testing over the
monitoring. Circulation 103:462–468,
3. Almdal T, Scharling H, Jensen JS, Vester-
gaard H: The independent effect of type 2
curve for long-term risk prediction. Stat
First, use of aspirin might increase the risk
14. Chambless LE, Heiss G, Shahar E, Earp
MJ, Toole J: Prediction of ischemic stroke
with 20 years of follow-up. Arch Intern
munities Study. Am J Epidemiol 160:259 –
DIABETES CARE, VOLUME 30, NUMBER 1, JANUARY 2007
Risk equation for stroke in type 2 diabetes
patients: Hong Kong Diabetes Registry.
15. Harrell F: Regression Modelling StrategiesDiabetologia 49:2299 –2308, 2006
with Applications to Linear Models, Logistic
19. Mann JF, Gerstein HC, Pogue J, Bosch J,
Regression, and Survival Analysis. New
Yusuf S: Renal insufficiency as a predictor
radiologic features. Neurology 54:2298 –
24. Woo J, Lau EM: Risk factors predisposing
trial. Ann Intern Med 134:629 – 636, 2001
tion: a longitudinal study. Neuroepidemi-
25. Moons KG, Bots ML, Salonen JT, Elwood
Prevalence (MAP) Study. Diabetologia 48:
PC, Freire de Concalves A, Nikitin Y, Siv-
filtration rate in addition to albuminuria is
enius J, Inzitari D, Benetou V, Tuomilehto
17. Gerstein HC, Mann JF, Yi Q, Zinman B,
important in managing type II diabetes.
of stroke in the general population in Eu-
21. International Diabetes Federation: IDF
global guideline for type 2 diabetes. Avail-
fibrinogen and electrocardiography? J
events, death, and heart failure in diabetic
Epidemiol Community Health 56 (Suppl.
and nondiabetic individuals. JAMA 286:
26. Thomsen TF, McGee D, Davidsen M, Jor-
18. Yang XL, So WY, Kong AP, Clarke P, Ho
22. Saaddine JB, Engelgau MM, Beckles GL,
gensen T: A cross-validation of risk-scores
for coronary heart disease mortality based
diabetes report card for the United States:
JC: End-stage renal disease risk equations
quality of care in the 1990s. Ann Intern
Studies and Framingham Heart Study. Int
DIABETES CARE, VOLUME 30, NUMBER 1, JANUARY 2007
Klinische Studien_KORR1_Musterseiten 06.09.13 07:13 Seite 19 1.2 Signifikanz (p-Wert)Um welches Problem geht es in diesem Unterkapitel?Im Rahmen einer wissenschaftlichen Studie können in der Regel nicht alle Patienten untersucht werden. Das führt zu dem Problem, dass von einer Aus- wahl (Stichprobe) auf die Grundgesamtheit (Population) geschlossen werden muss. Wie aber ist es möglich, vo
CONSIDERAZIONI SULL’USO DEGLI IMMUNOSOPPRESSORI EQUIVALENTI DOPO TRAPIANTO D’ORGANO SOLIDO Introduzione I pazienti portatori di un trapianto d’organo solido (rene, fegato, cuore, polmone, pancreas, intestino) devono assumere quotidianamente farmaci immunosoppressori per la prevenzione del L’uso di questi farmaci ha rappresentato, e rappresenta tutt’ora, uno degli
 Risk equation for stroke in type 2 diabetes
Risk equation for stroke in type 2 diabetes