Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Pulmonary alveolar microlithiasis in childhood: clinical and radiological follow-up
Pediatric Pulmonology 34:384–387 (2002)
Pulmonary Alveolar Microlithiasis in Childhood:
Stipan Jankovic, MD, PhD,1* Neven Pavlov, MD, PhD,2 Ante Ivkosic, MD,3 Ivana Erceg, MD,3
Meri Glavina-Durdov, MD, PhD,4 Jadranka Tocilj, MD, PhD,5 Slavica Dragisic-Ivulic, MD,2
Summary. This report describes a case of pulmonary alveolar microlithiasis that was diagnosed inan 8.5-year-old girl by high-resolution computed tomography (CT) and open lung biopsy. Presenceof symptoms (productive cough, fever), their periodic occurrence (lasting up to 1 week), andcomparatively long asymptomatic periods should be emphasized. Despite extensive X-rayabnormalities, tests of pulmonary interstitium involvement and exercise tests revealed normalresults. A therapeutic regimen, including disodium etidronate, was administered for 18 months withno significant clinical or radiological improvement. Pediatr Pulmonol. 2002; 34:384–387.
Key words: pulmonary alveolar microlithiasis; high-resolution computed tomography;
healthy until age 8 years. At that time, her symptomsreappeared: temperature up to 398C, bronchitis, pneumo-
Pulmonary alveolar microlithiasis (PAM) is a rare
nia, and cough with expectoration of purulent sputum
disorder of unknown etiology. As of 1996, only 36 cases of
lasting up to 10 days. Afterwards she would become
PAM were recorded in children under age 12 years.1–3 It
afebrile and feel subjectively better.
occurs predominantly in adults in the second decade of
This time the patient was sent to the hospital because of
life, with slightly more females affected.4 Until 1993, 173
pain in the chest and cough. At admission she was eupneic
cases had been reported from all over the world, and for
and afebrile, with a productive cough. Her body weight
unknown reasons PAM is most prevalent in Turkey.5 PAM
was in the 10th and her height between 10th and 25th
is characterized by intraalveolar calcifications diffusely
percentiles. Breath sounds were diminished over the lungs
arranged in the middle and lower parts of lungs. No
bilaterally (more markedly in the basal zones). Laboratory
general disturbance in calcium metabolism has been
findings included an elevated erythrocite sedimentation
demonstrated.6 Children with PAM are commonly
rate (50 mm/hr). Complete blood counts, urine, electro-
asymptomatic, although occasionally chronic cough as a
lytes in serum, calcium, phosphorus, alkaline phospha-
nonspecific symptom is present. The diagnosis is usually
tase, urea, creatinine, uric acid, C3 and C4 complement
based on the characteristic miliary (spotlike) ‘‘sandstorm’’ changes on chest X-ray, usually detected inciden-
tally. In some cases, clinical and radiological findings may
Department of Radiology, University Hospital Split, Split, Croatia.
2Department of Pediatrics, University Hospital Split, Split, Croatia.
3Department of Genetics and Developmental Biology, University ofConnecticut School of Medicine, Farmington, Connecticut.
M.V., an 8.5-year-old girl, was sent from a regional
hospital in Bosnia and Herzegovina with a diagnosis of
4Department of Pathology, University Hospital Split, Split, Croatia.
miliary tuberculosis. She was admitted to our Department
5Department of Pulmonology, University Hospital Split, Split, Croatia.
of Pediatrics because of pain in the chest and productivecough. The parents were not consanguineous; both were
*Correspondence to: Stipan Jankovic, M.D., Ph.D., Department of
healthy, as was a 5-year-old brother (all had normal chest
Radiology, University Hospital Split, 21000 Split, Croatia.
X-rays). History revealed that the patient, from age 4
months up to approximately 1 year, suffered from frequent
Received 9 January 2000; Accepted 12 January 2001.
high temperatures (up to 418C) lasting up to a week, witha clinical picture of bronchitis. She was treated with
antibiotics and mucolytic agents. Thereafter, she was
Published online in Wiley InterScience (www.interscience.wiley.com).
Childhood Pulmonary Alveolar Microlithiasis
components, fibrinogen, C-reactive protein, immunodif-fusion (IgA, IgG, IgM), parathyroid hormone, andacid-base status were normal. Electrophoresis of serumproteins (EFP) indicated slightly elevated total proteins,a1, a2, and b-globulins. Ratio of Ca/creatinine (in 24 hrurine) was 1.48 mmol/day (2.47 mg/kg/day; withinnormal limits). Ratio of Ca (urine)/creatinine (urine) was0.07 (no hypercalciuria). PPD3 IU showed 6 mm indur-ation (she had the BCG scar). The M. tuberculosis culturefrom gastric lavage taken for 3 successive days wasnegative.
Chest radiographs revealed bilateral diffuse punctiform
shadows in the middle and lower pulmonary fields (Fig. 1). High-resolution computed tomography (CT) was per-formed and showed tiny miliary consolidations, primarlyin an alveolar setting, symmetrically in both lungs (Fig. 2).
Open biopsy of the right lung lobe revealed firm and
Fig. 2. High-resolution CT of the thorax (4- and 2-mm scans).
gritty subpleural pulmonary tissue. Histologically, alveoli
Tiny, firm miliary consolidations, primarily in an alveolar setting,
contained numerous concentrically lamelated concretions
can be seen symmetrically, mainly hilopetally in both lobes of thelungs. Interstitial fibrous changes in the form of netlike and
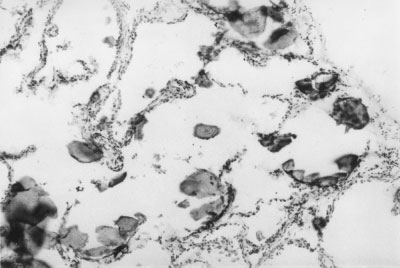
measuring 50–100 mm in diameter (Fig. 3). Histhochemi-
stripped interstitial beams are also present, predominantly in
cally, they are calcospherites which have polysaccharide-
anterior segments of lung lobes. Elements of retractive pulmo-
rich core and a rim of tricalcium phosphate with small
nary changes with compensatory local hyperinsuffllations can
amounts of magnesium and aluminium (periodic acid-
Schiff reagent method for mucopolysaccharides waspositive, von Kossa alizarin red method for calcium was
positive). Intraalveolar septa are thin, with mild chronicinflammatory cell infiltrates without significant fibrosis.
Pulmonary function tests were normal (spirometry,
flow-volume curve, diffusing capacity of the lungs, andexercise tests).
The disodium salt of 1-hydroxythylidene diphosphonic
acid (disodium etidronate) was used at a dose of 400 mgper day for 18 months. Despite this therapy, no significantclinical or radiological improvement was reported (Fig. 4).
The first report of a high incidence of PAM in family
members was published in 1954.8 Further, a number of
Fig. 1. Chest X-ray of 8.5-year-old girl. Parenchyma punctiformshadows bilaterally diffuse in lungs, predominantly in the middleand lower fields, more to the center where they form modularshadows up to a few millimeters in diameter.
Fig. 3. Pathohistological findings. Alveoli contained numerous
concentrically lamelated concretions measuring 50–100 mm
sputum, high temperature with duration of a week perepisode. Between the above-mentioned episodes therewere longer asymptomatic periods (some of them lastingfor a couple of years). Our patient was sent for hospitaltreatment with a diagnosis of miliary tuberculosis. She hadher first chest X-ray done immediately before admission. Despite impressive changes on the chest X-ray, no sign ofpulmonary function disorders could be found (normalfindings of spirometry, flow-volume curve, diffusingcapacity of the lungs, and exercise tests) which wouldsuggest any extensive disease of the pulmonary inter-stitium. HRCT of the lungs revealed irregularly arrangedchanges in the lungs (most pronounced in the middle andlower lung fields, more to the center). Interstitial fibrouschanges were also present, mainly in the anterior lung
Fig. 4. Chest X-ray of 8.5-year-old girl after 18 months of
segments, with retractive changes of the lung parenchyma
treatment with disodium etidronate. Despite therapy, no radio-logical improvement was seen (compare with Fig. 1).
and compensating local hyperinsufflations. We could findno evidence of ventilation disorders. No specific therapyof PAM has been reported. There are a few reports of lung
papers published on this condition underline a familial
transplantation, which might be the only therapy for
component of PAM in siblings,9 relatives,1 and twins,9,10
patients with progressive disease.17 Glucosteroid therapy
suggesting the possible autosomal-recessive character of
may lead to improvement of pulmonary function and
the disease. So far, no definitive predisposing factors have
exercise tolerance.12 Gocmen et al.18 gave diphosphonate
been identified, such as an environmental exposure to
and disodium etidronate to a 3.5-year-old-girl with PAM
toxic substances, or airborne or infectious agents.
in order to inhibit the growth of hydroxyapatite micro-
Children with PAM are commonly asymptomatic;
crystals (duration, 36 months at a dose of 15 mg/kg). They
sometimes a chronic cough occurs as the main symptom.
obtained radiological improvement in the form of some
However, in most cases, a persistent cough of more than
clearing of lung bases, as well as subjective improvement
3 years’ duration,11 clinically significant interstitial pul-
monary disease,12 and lymphocytic interstitial pneumo-
We treated our patient for 18 months with disodium
nitis have been reported. Hemoptysis has been reported in
etidronate, but the results suggest no radiological im-
one patient.13 While expectoration of unidentifiable mi-
provement (Fig. 4). Similar results were published by
croliths has not been reported in children, there are several
Mariotta et al.19 Our experience allows us to emphasize
reports of microliths in sputum specimens of adults.14
the importance of HRCT in diagnosis of PAM in children.
Dyspnea develops with the progress of the disease, and it
Although the final evidence of diagnoses can be obtained
may spread slowly, having benign characteristics,6 even
only by lung biopsy, HRCT can yield highly accurate
though there is no report of spontaneous remission of the
data on the involvement and intensity of pulmonary
disease. With the progress of PAM, pulmonary insuffi-
changes, which are particularly important when pulmo-
ciency with cyanosis, hypoxya, and clubbing of fingers
nary function tests are normal. We started the therapy
develops, and death results from impaired pulmonary
with disodium etidronate, firmly believing that a control
HRCT will be of great help in the evaluation of its
The diagnosis of PAM is usually based on the charac-
teristic ‘‘sand storm’’ changes on chest X-ray. It can beconfirmed by open biopsy of the lung, which will
demonstrate typical microliths in one third to two thirdsof alveoli, and by bronchoalveolar lavage (BAL). The use
1. Biary MS, Adullah MA, Assaf HM, Wazzan A. Pulmonary
of high-resolution computed tomography (HRCT), a
alveolar microlithiasis in a Saudi child and two cousins. Ann TropPaediatr 1993;13:409–413.
method with a high degree of accuracy, may be of great
2. Schmidt H, Lorcher U, Kitz R, Zielen S, Ahrens P, Koning R.
help in the diagnosis of PAM.15 Signs of interstitial
Pulmonary alveoar microlithiasis in children. Pediatr Radiol
thickening may present radiological signs.16 The micro-
liths are characterized by intraalveolar depositions of
3. Wallis C, Whitehead B, Malone M, Dinwiddie R. Pulmonary
calcified granules, usually varying in size from about 0.1–
alveolar microlithiasis: diagnosis by transbronchal biopsy. PediatrPulmonol 1996;21:62–64.
4. Mariotta S, Guidi L, Papale M, Ricci A, Bisetti A. Pulmonary
Our patient had the following symptoms: pain in the
alveolar microlithiasis: review of Italian reports. Eur J Epidemiol
chest, intensive cough, abundant expectoration of purulent
Childhood Pulmonary Alveolar Microlithiasis
5. Ucan ES, Keyf AI, Aydilek R, Yalcin Z, Sebit S, Kudu M, Ok U.
12. Ratjen FA, Schoenfeld B, Wiesemann HG. Pulmonary alveolar
Pulmonary alveolar microlithiasis: review of Turkish reports.
microlithiasis and lymphocytic interstitial pneumonitis in a ten
year old girl. Eur Respir J 1992;5:1283–1285.
6. Phelan PD, Olinsky A, Robertson C. Pulmonary alveolar
13. Thind GS, Bhatia JL. Pulmonary alveolar microlithiasis. Br J Dis
microlithiasis. In: Phelan PD, Olinsky A, Robertson C, editors.
Respiratory illness in children. London: Blackwell Scientific
14. Tao LC. Microliths in sputum specimens and their relationship
to pulmonary alveolar microlithiasis. Am J Clin Pathol 1978;69:
7. Shisido S, Toritani T, Nakano H, Tokushima T. A case of alveolar
microlithiasis which developed spontaneous pneumothorax due to
15. Korn MA, Schurawitzki H, Klepetko W, Burghuber OC.
progression of emphysematous bullae during 34 years after
Pulmonary alveolar microlithiasis: findings on high resolution
established diagnoses. Nippon Kyobu Shikkan Gakkai Zasshi
16. Melamed JW, Sostman HD, Ravin CE. Interstitial thickening in
8. Mikhail V. Pulmolithiasis endalveolaris et interstitialis difusa.
pulmonary alveolar microlithiasis; an underappreciated finding.
9. Arguelles M, Quinonez MG, Cicero R, Giacinti P. Pulmonary
17. Stamatis G, Zerkowski HR, Doetsch N. Sequential bilateral lung
alveolar microlithiasis in two siblings. Rev Invest Clin 1993;45:
transplantation for pulmonary alveolar microlithiasis. Ann
10. Caffrey PR, Captain MC, Altman RS. Pulmonary alveolar
18. Gocmen A, Toppare MF, Kiper N, Buyukpamukcu N. Treatment
microlithiasis occuring in premature twins. J Pedatr 1965;16:
of pulmonary alveolar microlithiasis with diphosphonate—
preliminary results of a case. Respiration 1992;59:250–252.
11. Turktas I, Saribas S, Balkanci F. Pulmonary alveolar micro-
19. Mariotta S, Guidi L, Mattia P, Torelli L, Pallone G, Pedicelli G,
lithiasis presenting with chronic cough. Postgrad Med J 1993;69:
Bisetti A. Pulmonary microlithiasis. Report of two cases. Respira-
The discovery of ribonucleic acid interference has sparked a wave of enthusiasm in the scientific community. Since the discovery of RNA interference scientists have used it to identify the molecular processes of different diseases. RNA interference has the potential to be used in a wide range of applications one of which is cancer therapies. The unique key to RNA interference as it does have an


 Childhood Pulmonary Alveolar Microlithiasis
components, fibrinogen, C-reactive protein, immunodif-fusion (IgA, IgG, IgM), parathyroid hormone, andacid-base status were normal. Electrophoresis of serumproteins (EFP) indicated slightly elevated total proteins,a1, a2, and b-globulins. Ratio of Ca/creatinine (in 24 hrurine) was 1.48 mmol/day (2.47 mg/kg/day; withinnormal limits). Ratio of Ca (urine)/creatinine (urine) was0.07 (no hypercalciuria). PPD3 IU showed 6 mm indur-ation (she had the BCG scar). The M. tuberculosis culturefrom gastric lavage taken for 3 successive days wasnegative.
Childhood Pulmonary Alveolar Microlithiasis
components, fibrinogen, C-reactive protein, immunodif-fusion (IgA, IgG, IgM), parathyroid hormone, andacid-base status were normal. Electrophoresis of serumproteins (EFP) indicated slightly elevated total proteins,a1, a2, and b-globulins. Ratio of Ca/creatinine (in 24 hrurine) was 1.48 mmol/day (2.47 mg/kg/day; withinnormal limits). Ratio of Ca (urine)/creatinine (urine) was0.07 (no hypercalciuria). PPD3 IU showed 6 mm indur-ation (she had the BCG scar). The M. tuberculosis culturefrom gastric lavage taken for 3 successive days wasnegative.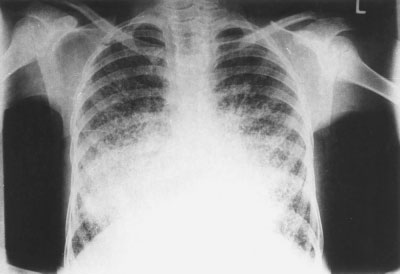 sputum, high temperature with duration of a week perepisode. Between the above-mentioned episodes therewere longer asymptomatic periods (some of them lastingfor a couple of years). Our patient was sent for hospitaltreatment with a diagnosis of miliary tuberculosis. She hadher first chest X-ray done immediately before admission.
sputum, high temperature with duration of a week perepisode. Between the above-mentioned episodes therewere longer asymptomatic periods (some of them lastingfor a couple of years). Our patient was sent for hospitaltreatment with a diagnosis of miliary tuberculosis. She hadher first chest X-ray done immediately before admission.