Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Educadorfisicoadinis.com.br
Journal of PHYSIOLOGICAL ANTHROPOLOGY and Applied Human Science Original A Unique Method for Predicting Cardiorespiratory Fitness Using Rating of Perceived Exertion 1) Department of Epidemiology, National Institute for Longevity Sciences (NILS)2) Institute of Health and Sport Sciences, University of TsukubaAbstract The purpose of this study was to develop a (5): 255-261, 2001 http://www.jstage.jst.go.jp/en/
simple and convenient indirect method for estimating
Keywords: maximal
rating of perceived exertion (RPE) during a submaximal
f o u r he a l th y Ja p a ne s e m e n, a ge d 2 0 t o 6 4 ye a r s ,
Introduction
volunteered to participate in the study. The subjects wererandomly divided into two groups, a validation (V) group
Low levels of cardiorespiratory fitness and physical
(n=100) and a cross-validation (CV) group (n=54). The V
inactivity have been associated with an increased risk of
and CV groups performed a maximal cycling test and the
contracting several chronic disease states (Blair et al.,
1989; Paffenbarger et al., 1986), including coronary
documentation of three categories (overall, chest, legs) of
artery disease, stroke, hypertension, diabetes, and some
RPE, up to a rating of 15. Prediction equations of VO
forms of cancer. Direct measurement of maximal oxygen
were developed by multiple regression analysis
the V group were 2462 ± 484 ml·min–1 and 1349 ± 334
cardiorespiratory fitness, requires considerable expense
ml·min-1, respectively. Correlational analyses indicated
in terms of equipment and medical supervision, and
that the workrate (W) at which the legs RPE (RPE
might cause dyspnea, panting, leg pain and fatigue in a
reached 15 or higher was evaluated first (W
The anaerobic threshold (AT) determined as the lactate
threshold (LT) has been regarded as one of the most
(r=0.790), respectively. The developed prediction
useful indices in prescribing exercise intensity. Firstly,
A T o r LT w hi ch r e flec ts th e eff ic i enc y o f a er o b ic
(kgm·min–1) – 15.84age (yr) + 13.06
metabolism in peripheral skeletal muscles could be an
weight (kg) + 1365 (R=0.849, SEE=261 ml·min–1) VO
index of cardiorespiratory fitness (Ivy et al., 1980).
Secondly, these same indices can be used as possible
665 (R=0.816, SEE=195 ml·min–1) Results of a cross-
indices of effective and safe training intensity (Jacobs et
v ali dation analysi s indi ca ted a simi lar es ti mati on
al., 1986). In general, however, it is difficult to use AT in
(r=0.793 and 0.853, and SEE=240 ml·min–1 and 183
most public health-oriented facilities because of the
ml·min–1) compared with the above equations developed
complexity and high cost of the technique. A number of
from data of the V group. Reliability coefficients of V
methods for estimating AT have been developed (Brettoni
et al., 1989; Conconi et al., 1982), but these are not useful
significant and there was no difference in the mean value
from the perspective of accuracy and simplicity (Francis
between trials 1 and 2. The “RPE method” developed for
estimating cardiorespiratory fitness is not only a unique
A number of indirect methods for predicting VO2max
indirect method but also a valid and useful tool in various
using heart rate (HR) during submaximal exercise
settings of exercise prescription. J Physiol Anthropol 20
(Åstrand and Ryhming, 1954; Margaria et al., 1965;
Siconolfi et al., 1982; Miyashita et al., 1985) have been
Table 1 Physical and physiological characteristics of the subjects
developed. However, HR can be affected by many factors,
e.g., environmental temperature and humidity, state of
health and mind, and especially medications (caffeine
and β-blockers (Noble and Robertson, 1997)). Also, the
validity of these methods has been questioned by some
investigators (Gutmann et al., 1981; Pollock et al., 1986).
Therefore, the development of alternate methods for
estimating LT without HR are needed.
Borg’s 15-grade rating of perceived exertion scale
(RPE) (Borg, 1973) corresponding to AT during a graded
exercise test has been reported by many investigators to
range from 12 to 14 (Robertson and Noble, 1997) and it is
not influenced by exercise modality, gender, age, training
habits and medications (Noble and Robertson, 1997). Ithas been shown that RPE is closely correlated with
relative exercise intensity measured by VO
(Robertson, 1982). On the basis of the above findings, it
seems possible to assess cardiorespiratory fitness from
the RPE. Nevertheless, such RPE methods for predicting
during a maximal GCT using a Monark cycle ergometer
(type 818E). The cycle ergometer was calibrated weekly
using a 4.0-kg reference weight. The effect of the height
p r e d i c t e d f r o m a m e a s u r e o f w o r k r a t e a n d R P E
of the seat on oxygen consumption and lower limb
respectively during submaximal graded exercise. The
kinematics has been established; thus, height of the seat
purpose of this study was to develop a simple, convenient,
was standardized by having the subject sit on the cycle
ergometer and extend a leg onto the pedal in the down
(ml·min–1) from indices of workrate and RPE
position. Final height of the seat was adjusted so that leg
respectively. In the present study, the “RPE method” is
extension was approximately 165–170 degree angle at the
defined as a method which enables prediction of VO
knee joint. Following a resting electrocardiogram (ECG)
using the data collected during a submaximal
and a blood pressure recording, the exercise test began
with a 2 minute of unloaded warm-up cycling task (0 kg)
at 60 rpm. Following the warm-up, a workrate (W) of 90
Subjects and Methods
kgm·min–1 was given and the W was increased by 90kgm·min–1 each minute until volitional exhaustion
occurred. Pulmonary ventilation (VE) and gas exchange
One hundred and fifty-four healthy Japanese men, aged
were measured breath-by-breath with an on-line data
20 to 64 years (mean 40.8 ± 12.2 yr), volunteered to
acquisition system (Mijnhardt Oxycon αSystem). The
participate in this study. The subjects were randomly
turbine volume transducer was calibrated daily with a 3-
divided into two groups; a validation group (N=100) and a
liter calibration syringe. A continuous sample of expired
cross-validation group (N=54) (see Table 1 for subject
ga s w as tr a n s p or te d v i a h ea te d s am p l i n g l i n e s to
description). The physical activity level of the subjects
electronic gas analyzers for measurement of oxygen and
was either sedentary (N=106) or moderately active
c a r b o n d i o x i d e c o n c en t r a t i o n i n e x p i r e d a i r a n d
(N=48). The moderately active subjects engaged in
subsequent estimation of oxygen uptake (VO ), carbon
walking, jogging, swimming, and/or some other form of
dioxide output (VCO ) and the respiratory exchange ratio
exercise for approximately 30 to 60 minutes, 1–5 days a
(R). The gas analyzers were calibrated before each test
week (mean=3.5 days). None of them were elite athletes
with certified gases of known concentration (17.0%O and
or highly trained cyclists. The sedentary subjects
5.0%CO ). Throughout each test, ECG and HR were
reported no recent participation in regular physical
m o n i t o r e d c o n t i n u o u s l y ( D i n a s c o p e 5 0 1 , F u k u d a
activity. None of the subjects received any medication
known to affect the variables measured. Prior to the
initiation of the study, all subjects were informed of the
of VO (an increase of less than 150 ml·min–1) despite an
risks and benefits associated with the investigation and
increase in workrate; 2) the highest R value during the
signed a statement of informed consent.
final stage of the GCT was required to be > 1.10; 3)attainment of an age-predicted maximal HR was madeonly if the subjects met at least two of the above three
criteria. For detection of LT, a venous blood sample (1 mleach) was drawn each minute from the antecubital veinof each subject during the exercise test. Determination ofthe blood lactate concentration was performed by anelectrochemical enzymatic method using a lactateanalyzer (model 1500L, Yellow Springs Ins titute). Lactate threshold was conceptually defined as the pointat which the rate of lactate production and diffusionexceeded the rate of its removal, i.e., blood lactateconcentration increased non-linearly. To identify this
point, the log [blood lactate concentration] - log [VO ]
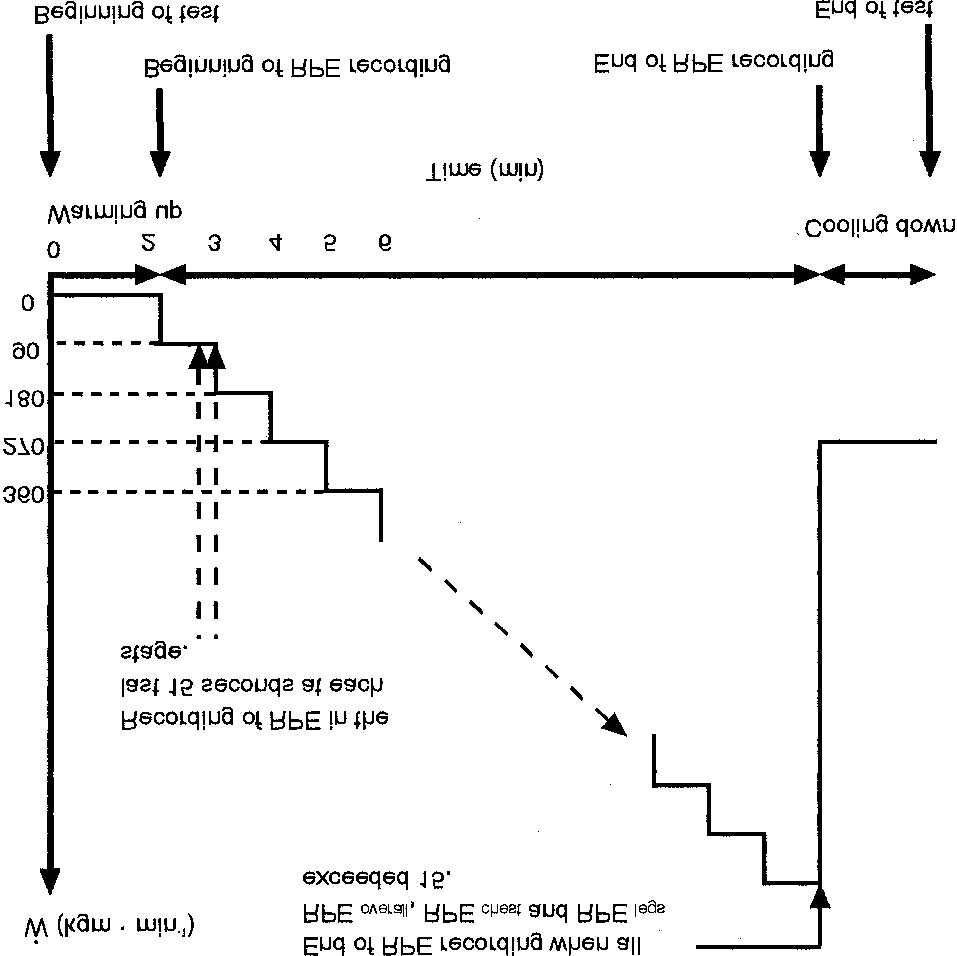
transformation method was used (Beaver et al., 1985). Evaluating 3 categories of RPE during GCTsubmax
Seven days after the maximal cycling test, GCTsubmax
was performed with documentation of RPE and HR only(see Fig. 1) terminated at RPE of 15. Three separatecategories of RPE were recorded: 1) An RPE
general feelings of physical fatigue; 2) An RPE
feelings associated with the cardiopulmonary system, and3) An R PE
, des cri bing feelings of str ai n in the
Fig. 1 Protocol of submaximal graded cycling test and recording
exercising muscles and joints (Pandolf et al., 1984).
These three RPEs were recorded one at a time during thelast 15 seconds of each stage by having each subject pointto an appropriate number to describe each feeling on the
RPE scale, held within easy reach by an investigator. Subjects were asked to give the RPE in the following
Physical and physiological characteristics of the
subjects are shown in Table 1. There were essentially no
significant difference (P>0.05) between the validation
group and the cross-validation group in all variables.
Pearson product-moment correlation coefficients (r)
were 2462 ± 484 and 1349 ± 334 ml·min–1, respectively
and in the cross-validation group 2462 ± 407 and 1377 ±
example, indicated as the workrate at which an RPE
F i g u r e 2 s h o w s m e a n ( ± S D ) o f w o r k r a t e s
of 15 or higher was first evaluated. Prediction equations
corresponding to each RPE. Workrates estimated by
were developed from the data of the validation group by
using a multiple linear regression analysis procedure
. Two dotted lines show the mean of W at AT (558
(stepwise method). The dependent variables were the V
kgm·min–1) and maximal exercise (1128 kgm·min–1).
Workrates at RPE of 13 were approximately equivalent to
the maximal GCT. The independent variables were 1) age
AT level. Ex er cis e intensi ty (p ercent of ma xim al
2) weight 3) height and 4) W variables, most significantly
workrate) at each RPE of 15 were 73.9 % for RPE
standard error of estimate (SEE = SD (1 – r2)1/2 ) and
I n Ta b le 2 t he co r r ela t i o n co e ffi c i en ts be tw ee n
percent SEE (%SEE = (SEE/mean) ·100) were calculated
to established the accuracy of the equations. The cross-
validity of the equations developed in the present study
was assessed in the cross-validation group by correlation
coefficients, SEE and %SEE. Test-retest reliability of the
respectively. Required time for estimation of WRPE legs 15
was 10.3 ± 2.1 min including warming up time (2 min)
correlation coefficients and paired t-test using randomly
drawn subjects (n=37) with a period of two days between
Multiple regression analyses by stepwise method using
trials 1 and 2. The probability of making a Type I error
was set at P ≤ 0.05 in paired t-test or P ≤ 0.001 in
weight and height as potential independent variables
yielded the equations in Table 3. In the equation of
Fig. 2 Means and standard deviations of workrates corresponding to each RPE.
height was not selected as an independent
Table 2 Correlation coefficients of workrate values at each RPEs
variable because height had no significant correlation
weight was not selected in the equation of VO
Relationships of the predicted values with measured
values in the cross-validation group are presented in Fig.
3. Correlation coefficients were significant (r=0.793 and
0.853), and SEE and %SEE in the predicted VO
against the measured values were 240 ml·min–1 and
183 ml·min–1, 9.7 % and 13.3 %, respectively.
The results of test-retest reliability are illustrated in Fig.
4 . C o m p a r i s o n b e t w e e n t r i a l 1 a n d 2 r e l i a b i l i t y
coefficients were significant (r=0.891 for VO
Discussion
There are a number of methods of predicting the
/ HR response to submaximal exercise on a cycle
ergometer. The treadmill ergometer, or stepping bench
or box are perhaps the most widely used methods(Shephard et al., 1968). Prediction is based on thesupposition that there is essentially a linear relationship
cardiac stimulants such as atropine accelerate exercise
Medications such as beta-blocking agents and cardiac
HR (Davies and Sargeant, 1979). Therefore, HR methods
stimulants are routinely used by patients with essential
hypertension who have a similar lifestyle to clinically
dosage of these medications is periodically titrated to
normal people. As an example, beta-blocking agents such
achieve an optimal therapeutic benefit. In such cases, it
as propranolol and atenolol attenuate exercise HR
(Hossack et al., 1980; Squires et al., 1982), whereas
the RPE. The correlation between RPE and %VO
Table 3 Prediction equations of VO
(R = 0.849, SEE = 261 ml·min–1, % SEE = 10.6%)
(R = 0.816, SEE = 195 ml·min–1, % SEE = 14.5%)
Fig. 3 Relationship of the predicted VO
measured values in the cross-validation group. Fig. 4 Relationship of VO
not change even if the dosage of these medications isperiodically titrated (Robertson, 1982). Hence, the RPE
allowed some trial and error in evaluating
the 3 categories of RPE in the beginning stage of a test.
in clinically normal people but also in patients with
Thus, the subjects could communicate accurate RPEs to
essential hypertension. Furthermore, the RPE method is
the examiners, especially, in the latter half of GCTsubmax.
frequently used as an adjunct to standard physiological
and clinical responses during a graded exercise test.
significantly to the high precision (good SEE and %SEE)
Measurement of perceived exertion during exercise
testing is an easily applied procedure, requiring no
bioelectri cal instrumentation or extensive s caling
most intense perceptual signal must be noted during
expertise on the part of a subject, patient, athlete, or
cycle ergometry. Robertson et al. (1979) reported that, in
physical education student (Noble and Robertson, 1997).
men, the perceptual signal from the legs was typically
For these reasons the use of an indirect method for
most intense (i.e., dominant) than from either the chest
evaluating cardiorespiratory fitness such as the RPE
or the overall signal. It also appeared that RPE
linked to blood lactate concentration through its relation
Fi tchett (1985) repor ted that the a sses sment of
to exercise intensity during an incremented test protocol
cardiorespiratory fitness by a incremental exercise test
(Robertson et al., 1986). On the basis of these reports it
protocol is more accurate than a method using a steady
has been hypo thesized in thi s s tud y tha t, u si ng 3
study could be terminated within 8 to 12 minutes in men
most intense signal would be able to be identified.
with average cardiorespiratory fitness. The duration of
The evidences supporting the above hypothesis are
shown in Fig. 2 and Table 2. As illustrated in Fig. 2,
VO during submaximal cycling at 100, 150 and 200
workrates estimated by the perceptual signal from legs
tended to be smaller than by the chest and overall signals.
previously reported to range from 2.0% to 5.6%, of which
90% is attributed to biological variability and 10% to
technological error (Katch et al., 1982). It may be
. In Table 2, especially noteworthy is the fact
difficult for indirect test methods to achieve %SEE of 10%
t h a t W v a l u e s b a s e d o n R P E
or lower. According to previous reports (Åstrand and
R y h m i n g , 1 9 5 4 ; R o w el l e t a l. , 1 9 6 4 ) , c o r r el a t i o n
coefficients between measured and predicted values
f i n d i n g s m a y b e d u e t o t he ex e r c i s e m o d e ( c yc le
using HR have been reported to range from r=0.58 to
ergometry). The workrate at which the RPE
r=0.95, and %SEE have ranged from 7% to 27% (Åstrand
and Ryhming, 1954; Fox, 1973; Margaria et al., 1965;
Rowell et al., 1964). Greiwe et al. (1995) reported that
(r=0.790), respectively. It was expected that the higher
%SEE of ACSM’s convenient submaximal cycle ergometer
the RPE score, the greater was the correlation between the
an RPE of 15 was the highest score recorded during the
in the current study may be better than other indirect
, W corresponding to this RPE had the highest
Test-retest reliability of the developed equations was
was observed for a W value corresponding to an RPE
examined using 37 randomly drawn subjects predicting
of 14. This may be due to the fact that AT occurs in most
from the main cohort of subjects (Fig. 4). In a comparison
cases at an RPE between 12 and 14 (Robertson and Noble,
between trials 1 and 2, reliability coefficients for VO2max
1997). These results in the validation group supported the
were r=0.891 and 0.870, respectively. The
above findings of Robertson’s report (1979).
values were significant and the difference between trials
In the current study the prediction equation of VO
was not significant. Therefore, it is suggested that VO
(Table 3). These two equations indicated that despite thesignificant correlation between age and cardiorespiratory
Conclusion
with them. The reason that weight was not selected as an
A simple and convenient method for predicting VO2max
was developed in this study. The workrate (W)
the case of forced adoption for weight as an independent
variable, multiple r (R=0.819) and SEE (195 ml·min–1)
as the best independent variables yielded the
including warming up time (2 min), which was equivalent
HRmax” test by Miyashita et al. (1985), the
– 15.84age (yr) + 13.06weight (kg) + 1365
most famous method in Japan. The purpose of that test
was to estimate the workrate corresponding to 75% of
maximal HR to each person. According to their report,
various physical and clinical risks were not found during
HRmax test”. In the current study, mean of
exercise intensity (percent of maximal workrate) for
Acknowledgement This study was supported in part by
Human Beings in the Ecosystem, Tsukuba Advanced
Research Alliance (TARA), University of Tsukuba.
v a l i d a t i o n g r o u p s w e r e c r o s s - v a l i d a t e d ( F i g . 3 ) .
Correlation coefficients between the RPE score and V
References
with SEE (240 ml·min–1 and 183 ml·min–1) and %SEE at
Armstrong LE, Costil DL (1985) Variability of respiration
9.7% and 13.3% which were good (low) enough to predict
and metabolism: responses to submaximal cycling and
and Costill (1985) demonstrated significant variability in
Å s t r a n d P O , R y h m i n g I ( 1 9 5 4 ) A n o m o g r a m f o r
calculation of aerobic capacity (physical fitness) from
Hrmax: A measure of aerobic work capacity.
pulse rate during submaximal work. J Appl Physiol 7:
Noble BJ, Robertson RJ (1997) The Role of RPE in
Beaver WL, Wasserman K, Whipp BJ (1985) Improved
Exercise Prescription. In Robertson RJ, Noble BJ eds.
detection of lactate threshold during exercise using a
Perceived exertion. Human Kinetics, Champaign, IL,
log-log transformation. J Appl Physiol 56: 1936–1940
Blair SN, Kohl HW, Paffenbarger RS, Clark DG, Cooper
Paffenbarger RS, Hyde RT, Wing AL, Rauramaa R (1986)
KH, Gibbons LW (1989) Physical fitness and all-cause
Physical activity, all-cause mortality and longevity of
mortality: A prospective study of healthy men and
college alumni. N Engl J Med 314: 605–613
Pandolf KB, Billings DS, Drolet LL, Pimental NA, Sawka
Borg G (1973) Perceived exertion: a note on “history” and
MN (1984) Differentiated ratings of perceived exertion
and various physiological responses during prolonged
Brettoni M, Alessandri F, Cupelli V, Bonifazi M, Martelli G
upper and lower body exercise. Eur J Appl Physiol 53:
(1989) Anaerobic threshold in runners and cyclists. J
Pollock ML, Jackson AS, Foster C (1986) The Use of the
Conconi F, Ferrari M, Giorgio Z, Droghetti P, Codeca L
Perception Scale for Exercise Prescription. In: Borg G,
(1982) Determination of the anaerobic threshold by a
Ottoson D eds. Perception of exertion in physical work.
noninvasive field test in runners. J Appl Physiol 52:
Rober tson RJ ( 1982) Central s ignals o f perceiv ed
Davies CT, Sargeant AJ (1979) The effects of atropine and
exertion during dynamic exercise. Med Sci Sports
practolo on the perception of exertion during treadmill
Robertson RJ, Noble BJ (1997) Perception of physical
F i tc he tt MA ( 19 85 ) P r edi ct ab i li ty o f VO
exertion: methods, mediators, and applications. In:
submaximal cycle ergometer and bench stepping tests.
Holloszy JO ed. Exercise and sport sciences reviews.
F o x E L ( 1 9 7 3 ) A s i m p l e , a c c u r a t e t e c h n i q u e f o r
Robertson RJ, Gillespie RL, Carthy JM, Rose KD (1979)
predicting maximal aerobic power. J Appl Physiol 35:
D i f f e r e n t i a t e d p e r c e p t i o n s o f e x e r t i o n : P a r t 2 .
R e l a t i o ns hi p t o l o c a l a n d c e n t r a l p h y s i o l o g i c a l
Francis KT, McClatchey PR, Sumsion JR, Hansen DE
responses. Percept Mot Skills 49: 691–697
(1989) The relationship between anaerobic threshold
Robertson RJ, Falkel JE, Drash AL, Swank AM, Metz KF,
and heart rate linearity during cycle ergometry. Eur J
Spungen SA, LeBoeuf JR (1986) Effect of blood pH on
peripheral and central signals of perceived exertion.
Greiwe JS, Kaminsky LA, Whaley MH, Dwyer GB (1995)
Evaluation of the ACSM submaximal ergometer test for
Rowell LB, Taylor HL, Wang Y (1964) Limitations to
prediction of maximal oxygen intake. J Appl Physiol 19:
Gutmann MC, Squires RW, Pollock ML, Foster C, Anholm
J (1981) Perceived exertion-heart rate relationship
Shephard RJ, Allen C, Benade A (1968) Standardization
during exercise testing and training in cardiac patients.
of submaximal exercise tests. Bull Wld Hlth Org 38:
Hossack KF, Bruce RA, Clarke LJ (1980) Influence of
Siconolfi SE, Cullinane M, Carleton RA, Thompson PD
propranolol on exercise prescription of training heart
modification of the Åstrand-Ryhming test. Med Sci
Ivy JL, Withers RT, Van Handel PJ, Elger DH, Costil DL
(1980) Muscle respiratory capacity and fiber types as
Squires RW, Rod JL, Pollock ML, Foster C (1982) Effect of
determinants of the lactate threshold. J Appl Physiol
p r o p r a n o l o l o n p e r c e i v e d e x e r t i o n s o o n a f t e r
myocardial revascularization surgery. Med Sci Sports
Jacobs I (1986) Blood lactate. Implications for training
and sports performance. Sports Med 3: 110–125
Ka tch V L , Sa d y SS, F r eed s o n P ( 198 2) B i o logi c al
variability in maximum aerobic power. Med Sci Sports
Correspondence to: Tomohiro Okura, Department of
M ar gar i a R, A d hem o P, R ou elli E ( 196 5) I nd i re ct
Epidemiology, National Institute for Longevity Sciences
determination of maximal oxygen consumption in man.
(NILS), 36-3 Gengo Morioka-cho, Obu, Aichi 474-8522,
Miyashita M, Mutoh Y, Yoshioka N, Sadamoto T (1985)
I N V E S T M E N T INTERSUISSE R E S E A R C H Antisense Therapeutics Ltd (ASX CODE: ANP) www.antisense.com.au December 2004 www.elixir-secs.com Victoria-based Antisense Therapeutics is one of the leading players in the discovery and development of second-generation antisense therapeutics. It has an important 5-year collaboration with the leading a
JETTI KATZ TROPICAL MEDICINE LAB TEST REQUISITION AND PRICE LIST Patient Name:________________________________ Purged: Non Purged: $ 400.00 Routine O/P Stool: Macroscopic and microscopy exam of stool for routine Protozoa and all Helminths, plus Entamoeba Histolytica Stool Antigen by E.I.A. and Giardia Stool Antigen by E.I.A. $ 670.00 Panel 1 Stool Test: Includes all test
 criteria. For detection of LT, a venous blood sample (1 mleach) was drawn each minute from the antecubital veinof each subject during the exercise test. Determination ofthe blood lactate concentration was performed by anelectrochemical enzymatic method using a lactateanalyzer (model 1500L, Yellow Springs Ins titute).
criteria. For detection of LT, a venous blood sample (1 mleach) was drawn each minute from the antecubital veinof each subject during the exercise test. Determination ofthe blood lactate concentration was performed by anelectrochemical enzymatic method using a lactateanalyzer (model 1500L, Yellow Springs Ins titute).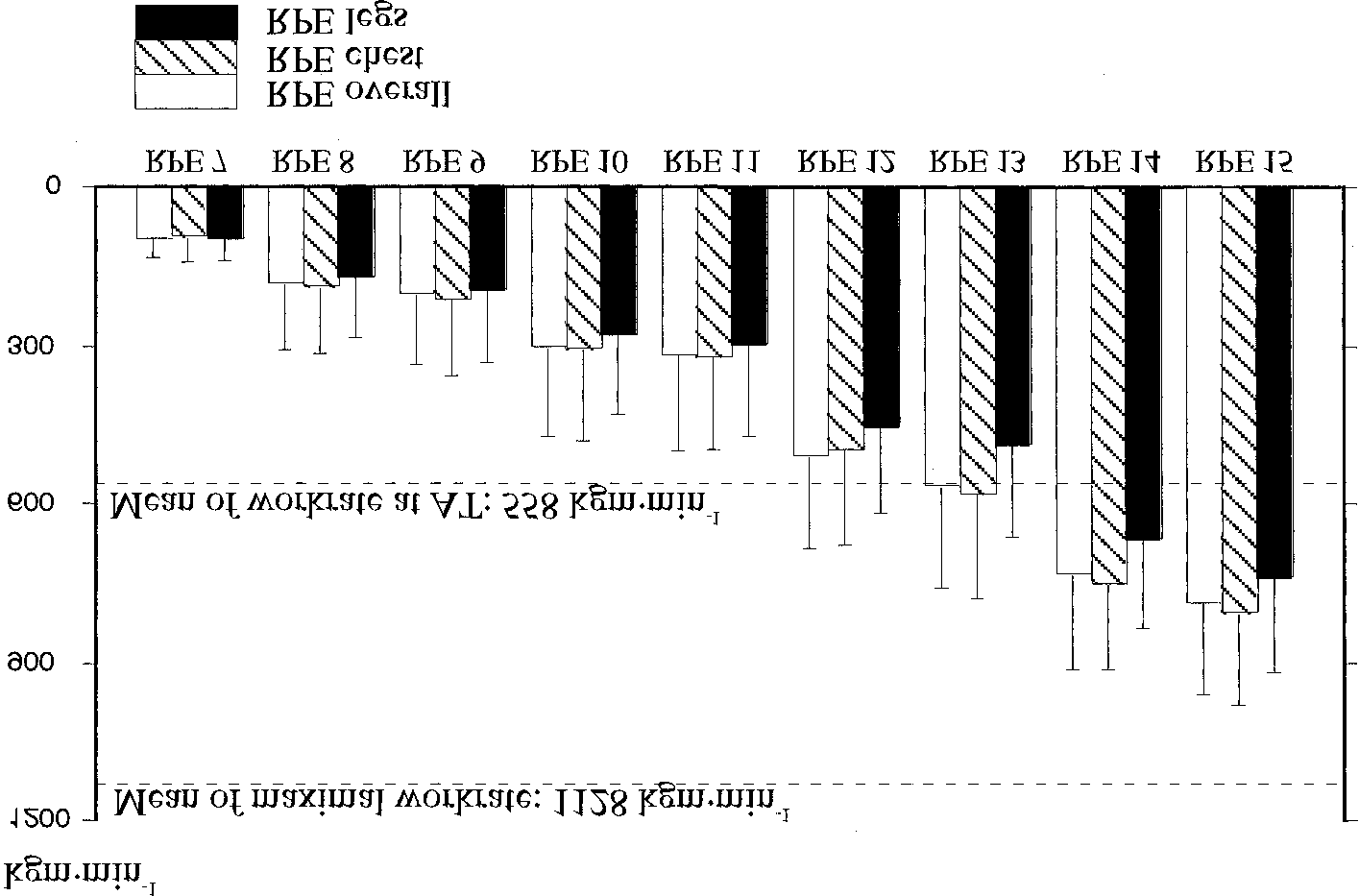 Fig. 2 Means and standard deviations of workrates corresponding to each RPE.
Fig. 2 Means and standard deviations of workrates corresponding to each RPE.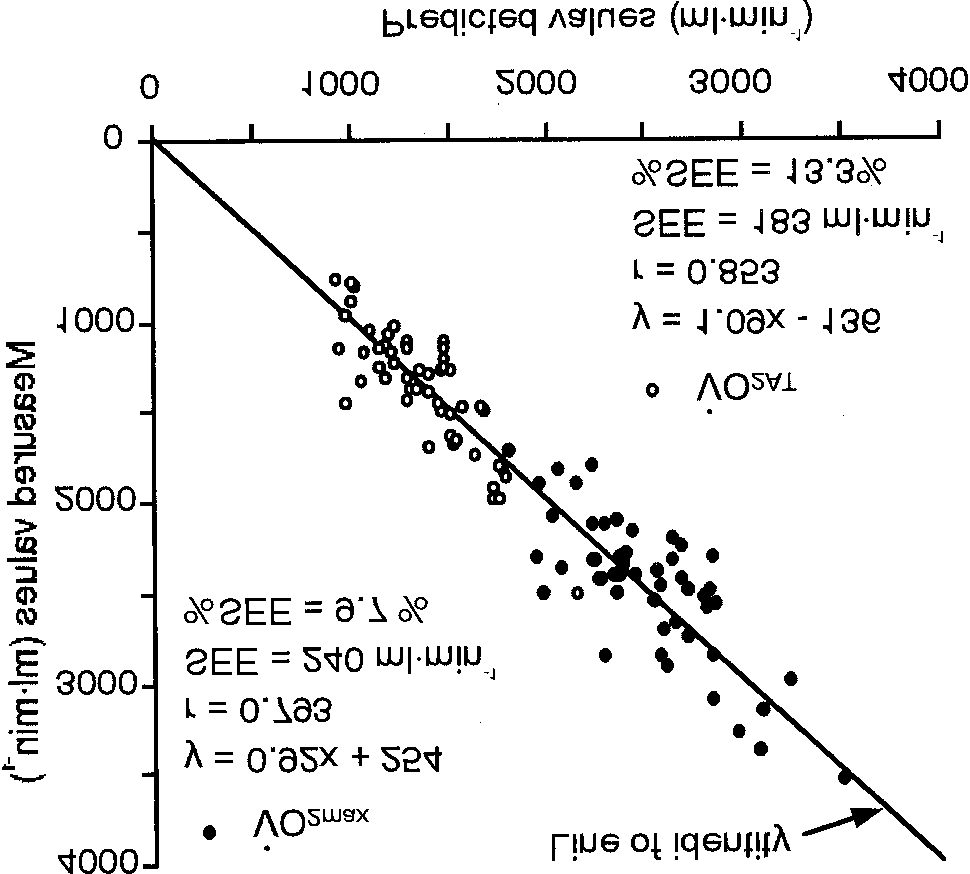
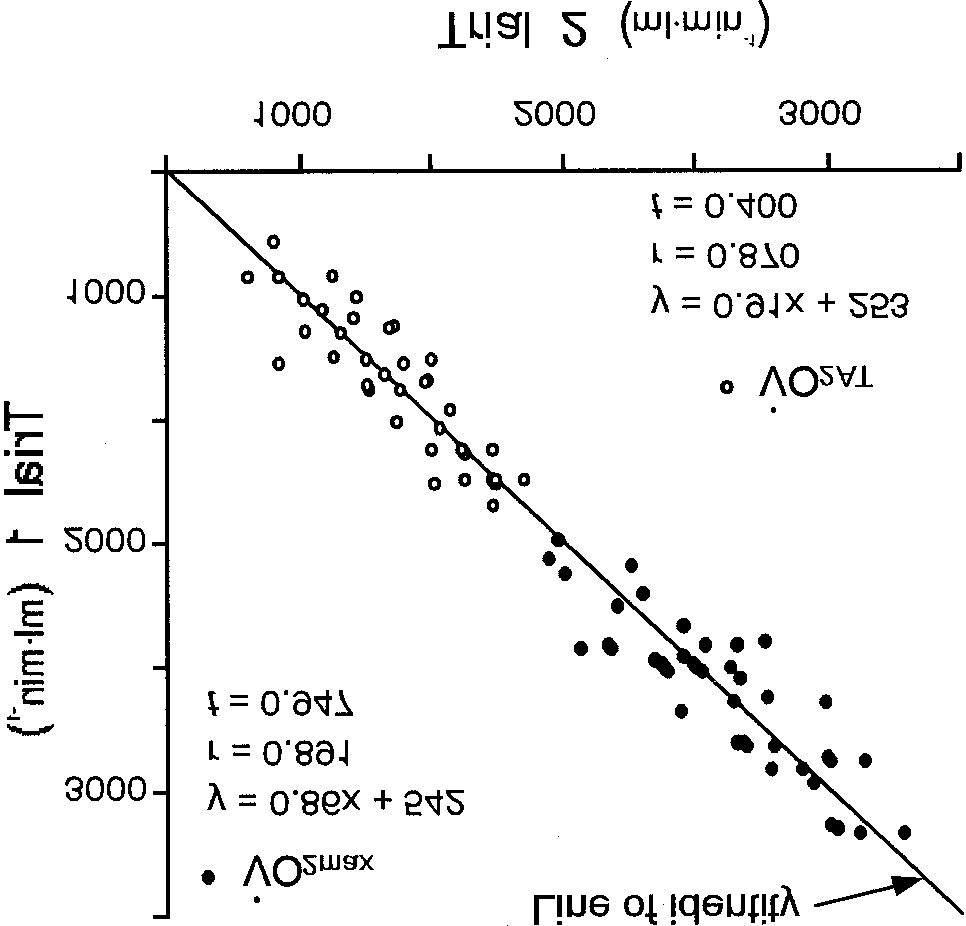 Table 3 Prediction equations of VO
Table 3 Prediction equations of VO