Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Patients with early rheumatoid arthritis who smoke are less likely to respond to treatment with methotrexate and tumor necrosis factor inhibitors: observations from the epidemiological investigation of rheumatoid arthritis and the swedish rheumatology register cohorts
2011, American College of Rheumatology
Patients With Early Rheumatoid Arthritis Who Smoke Are
Less Likely to Respond to Treatment With Methotrexate and
Observations From the Epidemiological Investigation of Rheumatoid Arthritis
and the Swedish Rheumatology Register Cohorts
´n,1 Maria Seddighzadeh,1 Camilla Bengtsson,2
Annmarie Wesley,2 Staffan Lindblad,1 Johan Askling,1 Lars Alfredsson,2 and Lars Klareskog1
Objective. To determine whether cigarette smok- European League Against Rheumatism criteria at the ing influences the response to treatment in patients with 3-month visit. The influence of cigarette smoking (cur- early rheumatoid arthritis (RA). rent or past) on the response to therapy was evaluated Methods. We retrieved clinical information about by logistic regression, with never smokers as the refer- patients entering the Epidemiological Investigation of ent group. Rheumatoid Arthritis (EIRA) early RA cohort from Results. Compared with never smokers, current 1996 to 2006 (n ؍ 1,998) who were also in the Swedish smokers were less likely to achieve a good response at 3 Rheumatology Register (until 2007). Overall, 1,430 of months following the start of MTX (27% versus 36%; the 1,621 registered patients were followed up from the P ؍ 0.05) and at 3 months following the start of TNF time of inclusion in the EIRA cohort. Of these, 873 inhibitors (29% versus 43%; P ؍ 0.03). In multivariate started methotrexate (MTX) monotherapy at inclusion, analyses in which clinical, serologic, and genetic factors and 535 later started treatment with a tumor necrosis were considered, the inverse associations between cur- factor (TNF) inhibitor as the first biologic agent. The rent smoking and good response remained (adjusted primary outcome was a good response according to the odds ratio [OR] for MTX response 0.60 [95% CI 0.39–0.94]; adjusted OR for TNF inhibitor response 0.52 [95% CI 0.29–0.96]). The lower likelihood of a good
The Epidemiological Investigation of Rheumatoid Arthritis
study was supported by grants from the Swedish Medical Research
response remained at later followup visits. Evaluating
Council, the Stockholm County Council, the Flight Attendant Medical
remission or joint counts yielded similar findings. Past
Research Institute, the Swedish Council for Working Life and Social
smoking did not affect the chance of response to MTX or
Research, King Gustaf V’s 80-Year Foundation, the Swedish Rheu-matism Association, the Swedish Combine project, and the European
TNF inhibitors. Evaluating the overall cohort, which
Community Sixth Framework Programme (project AutoCure). reflects all treatments used, current smoking was simi-
1Saedis Saevarsdottir, MD, PhD, Sara Wedre´n, MD, PhD,
larly associated with a lower chance of a good response
Maria Seddighzadeh, PhD, Staffan Lindblad, MD, PhD, JohanAskling, MD, PhD, Lars Klareskog, MD, PhD: Karolinska Institutet
(adjusted ORs for the 3-month, 6-month, 1-year, and
and Karolinska University Hospital, Stockholm, Sweden; 2Camilla
5-year visits 0.61, 0.65, 0.78, 0.66, and 0.61, respectively).
Bengtsson, PhD, Annmarie Wesley, MPH, Lars Alfredsson, PhD:Karolinska Institutet, Stockholm, Sweden. Conclusion. Among patients with early RA, cur-
Dr. Askling has received consulting fees, speaking fees, and/or
rent cigarette smokers are less likely to respond to MTX
honoraria from Wyeth and Bristol-Myers Squibb (less than $10,000
and TNF inhibitors.
Address correspondence to Saedis Saevarsdottir, MD, PhD,
Rheumatology Unit, Department of Medicine, Karolinska University
In patients with rheumatoid arthritis (RA), early
Hospital, 17176 Stockholm, Sweden. E-mail: saedis.saevarsdottir@
and efficient reduction of inflammatory activity is im-
portant for improving long-term outcome (1–3). The
Submitted for publication April 16, 2010; accepted in revised
panel of effective, yet often expensive, drugs with which
SMOKING AND RESPONSE OF EARLY RA TO MTX AND TNF INHIBITORS
to achieve this goal is growing. Baseline predictors of
PATIENTS AND METHODS
response to individual treatments would facilitate a
Source population of RA patients. We evaluated RA
rational choice of therapeutic strategy. In this regard,
patients from the Epidemiological Investigation of Rheuma-
modifiable predictors, such as cigarette smoking habits,
toid Arthritis (EIRA) study. EIRA is a population-based
are of particular interest. Since methotrexate (MTX)
case–control study covering the middle and southern parts of
and tumor necrosis factor (TNF) inhibitors are widely
Sweden, including as cases RA patients ages 18–70 years whoare within 1 year of diagnosis and, on average, within 10
used as first-and second-line treatments for recent-onset
months of symptom onset. All cases of RA were diagnosed by
RA, efforts to find predictors of response to these drugs
a rheumatologist, fulfilled the American College of Rheuma-
tology (ACR) 1987 criteria for RA (18), and were predomi-
Cigarette smoking has, in most studies following
nantly of Caucasian ancestry (97% of the participants). Weincluded in the present study all patients with RA who
patients with early RA or inflammatory polyarthritis,
participated in the EIRA study during its first decade, from
been associated with more use of disease-modifying
1996 to 2006. Of 2,097 patients included from the participating
antirheumatic drugs (DMARDs) and increased occur-
clinics, 1,998 (95%) answered a questionnaire that included
rence of extraarticular manifestations, including nod-
This study was approved by the Ethical Review Board
ules, while findings with regard to disease activity have
at the Karolinska Institute. All participants gave informed
not been conclusive (5–11). Smoking has also been
associated with radiologic progression in advanced RA
Capture of clinical data for EIRA patients from the
(8,12), while findings in early disease are less consistent
SRR. The SRR is a web-based national surveillance system that was started in the mid-1990s and is used optionally by
(5,9–11,13). However, only limited data are currently
rheumatologists to follow incident RA cases longitudinally as a
available about the influence of cigarette smoking on the
part of standard care. Information about disease activity,
response to individual treatments in early RA. For MTX
disability, and treatment are registered at each visit, which
monotherapy, a report of a randomized controlled clin-
occurs at predefined time points, although the clinical practicesetting allows some flexibility around the intended dates. Also
ical trial of 205 patients indicated a not significantly
hosted within the SRR is the Anti-Rheumatic Therapy in
reduced response among smokers (14), and no informa-
Sweden (ARTIS) registry, in which patients who receive
tion exists as to whether previous smoking influences
treatment with biologic agents, including TNF inhibitors, are
response. With respect to TNF inhibitors, current smok-
followed. ARTIS covers more than 90% of patients who haveever taken a biologic agent (ref. 19 and Neovius M: unpub-
ing (15,16) and the number of pack-years smoked (17)
have been associated with a reduced response in patients
By virtue of their early RA, patients included in EIRA
with established RA. Further, the extent to which an
are also invited to participate in the SRR. For the purpose of
apparent effect of smoking on the risk of developing RA
the present study, we linked these two data sources to captureclinical information about disease course and therapy. A
may be influenced by genetic factors known to interact
unique personal identification number permitted deterministic
linkage between the data sources. Of the 1,998 RA patients in
In the present study, we therefore linked baseline
the EIRA cohort, 1,621 had been registered in the SRR; 1,430
information on cigarette smoking (current or past and
of these patients started SRR followup at the time of EIRAinclusion (Figure 1) and were thus eligible for the current
cumulative dose) from a large population-based cohort
of patients with newly diagnosed RA to followup data on
DMARD treatment at baseline. Of the 1,430 patients
disease activity and treatment from the Swedish Rheu-
whose cases were followed from the time of EIRA inclusion,
matology Register (SRR) and investigated the influ-
873 (61%) received methotrexate monotherapy as their firstDMARD, 382 (27%) received treatment with other DMARDs
ence of smoking on treatment response in the overall
or combinations, and 175 (12%) received clinical care without
group, as well as specifically to the subgroup of patients
DMARD treatment at baseline. An overview of the DMARD
who initially started MTX monotherapy and the sub-
treatments or combinations initiated at baseline is shown in
group who later started TNF inhibitors as the first
Supplementary Table 1 (available on the Arthritis & Rheuma-tism web site at http://onlinelibrary.wiley.com/journal/10.1002/
biologic agent. Demographic and disease character-
(ISSN)1529-0131). In the present study, we focused on MTX
istics, serologic factors (rheumatoid factor [RF] and
as the initial DMARD, since it was the most commonly used
anti–cyclic citrullinated peptide [anti-CCP] antibody
first-line treatment. Other treatment options were included in
status), and genetic susceptibility factors (HLA–
Therapy with a biologic agent. Treatment with a TNF
DRB1 shared epitope and the PTPN22*620W risk al-
inhibitor (infliximab, etanercept, or adalimumab) was initiated
lele) were evaluated as potential confounders or effect
as the first biologic agent in 535 patients at a median of 3 years
after the diagnosis of RA (Figure 1). Fewer than 30 patients
Figure 1. Flow chart showing the distribution of rheumatoid arthritis (RA) patients who entered the Epidemiological Investigation of Rheumatoid Arthritis (EIRA) study during 1996–2006 and were also in the Swedish Rheumatology Register (SRR). The numbers of RA patients who had baseline data in the SRR at EIRA inclusion, had Disease Activity Score in 28 joints (DAS28) data available at the followup time points, and had been categorized as current, past, or never smokers are shown for the overall cohort, for patients receiving methotrexate (MTX) at baseline, and for patients receiving tumor necrosis factor (TNF) inhibitors during the followup until 2007. * In accordance with the eligibility criteria for the SRR and the EIRA study, the baseline visit in the SRR could occur up to 12 months before, and up to 2.5 months after, inclusion in the EIRA study. ** Detailed treatment data for all patients who received MTX monotherapy at baseline is shown in Supplementary Table 1 (available on the Arthritis & Rheumatism web site at http:// onlinelibrary.wiley.com/journal/10.1002/(ISSN)1529-0131). *** Predefined times for followup visits were at 3 months (range 2.5–5 months), 6 months (range 5–7.5 months), 1 year (range 7.5 months to 1.5 years), 2 years (range 1.5–2.5 years), and 5 years (range 4.5–5.5 years). # Patients who continued the same treatment until the followup visit. Reasons for treatment changes were not documented, but most patients changing treatment had no response according to the European League Against Rheumatism criteria.
had started any of the other available biologic agents (ritux-
Clinical variables were captured from the SRR. RF status was
imab, abatacept, anakinra, or unspecified biologic agent in
determined using standard procedures, and anti-CCP antibod-
clinical trials) before the end of the followup period in 2007,
ies were determined by the standard enzyme-linked immu-
usually after treatment with a TNF inhibitor.
nosorbent assay (Immunoscan RA Mark 2 ELISA; Euro-
Definition of treatment response. In accordance with
Diagnostica). The methods for determining the HLA–DRB1
recent guidelines from the European League Against Rheu-
shared epitope alleles and the PTPN22*620W (1858C/T) poly-
matism (EULAR) and the American College of Rheumatol-
morphism have been previously reported (22–25). At baseline,
ogy (ACR) (20), we used the EULAR response criteria (21),
the following data were not available: DAS28 for 0.8%, Heath
which are based on the Disease Activity Score 28-joint assess-
Assessment Questionnaire (HAQ) score for 3.4%, RF status
ment (DAS28), to define response to treatment. The primary
for 0.5%, anti-CCP antibody status for 4.3%, shared epitope
outcome of interest was a good response according to the
allele status for 2.0%, and PTPN22*R620W status for 3.7%.
EULAR response criteria (DAS28 Ͻ3.2 at the followup visit
Statistical analysis. We used 2 approaches to analyze
and Ͼ1.2 units decrease compared with the baseline DAS28),
the association between current smoking and a good response
and the secondary outcome was remission according to the
or remission according to the EULAR criteria. First, a good
EULAR response criteria (DAS28 Ͻ2.6 units at followup). We
response (DAS28 Ͻ3.2 at followup and Ͼ1.2 units decrease
evaluated these outcomes at the following predefined time
from baseline) as compared with no response (DAS28 Ͼ5.1 or
points: the 3-month, 6-month, 1-year, 2-year, and 5-year visits.
Ͻ0.6 units decrease) or a moderate response (falls between
The numbers of patients with available DAS28 and smoking
good response and no response) was evaluated using univari-
ate and multivariate logistic regression analyses. The results
Definition of baseline variables. Smoking status. We
were expressed as univariate P values and multivariate odds
retrieved information on smoking status from the EIRA
ratios (ORs) with 95% confidence intervals (95% CIs). Sepa-
questionnaire. Patients were classified according to their smok-
rate models were constructed for each time point for the
ing status at the time of RA diagnosis as never, past, current,
overall EIRA cohort at the 3-month, 6-month, 1-year, 2-year,
or irregular cigarette smokers, as well as other than cigarette
and 5-year followup visits. For the groups treated with MTX or
smokers (Table 1). The number of pack-years smoked (1
with TNF inhibitors, we restricted our analyses to the 3-month
pack-year ϭ 20 cigarettes/day for 1 year) was used to measure
and 6-month visits and considered only those who continued to
the cumulative dose of smoking. Information about cigarette
take the same treatment, since the reason for treatment
smoking habits was not available for 4.6% of the patients, and
changes was not registered (for example, lack of response or
8.2% lacked information about the number of pack-years.
side effects). The numbers of patients continuing each treat-
Other variables. Baseline parameters that we evaluated
ment are shown in Figure 1. Their smoking habits did not
as potential confounders or effect modifiers are listed in Table
differ significantly from the smoking habits of those who
1 and are described under the statistical analysis section below.
SMOKING AND RESPONSE OF EARLY RA TO MTX AND TNF INHIBITORS
Patient characteristics at treatment baseline*
Irregular smoking/other tobacco, no. (%)‡
* The study population consisted of patients from the Epidemiological Investigation of Rheumatoid Arthritis cohort who had baseline data in theSwedish Rheumatology Register (SRR). Subgroups represent patients who started monotherapy with methotrexate (MTX) or who received nodisease-modifying antirheumatic drug (DMARD) at baseline, as well as those who started a tumor necrosis factor (TNF) inhibitor as the first biologicagent during the followup period. DAS28 ϭ Disease Activity Score in 28 joints; IQR ϭ interquartile range; anti-CCP ϭ anti-cyclic citrullinatedpeptide; HAQ ϭ Health Assessment Questionnaire; NSAIDs ϭ nonsteroidal antiinflammatory drugs. † Not all patients had available information about smoking status, disease characteristics, or genetic factors. Missing values for each parameter aresummarized in Patients and Methods. ‡ Patients in this category were excluded from further analyses of cigarette smoking habits.
The following baseline parameters were evaluated in
ification, each parameter was also evaluated as a potential
the multivariate regression model: age at baseline (in 10-year
effect modifier. All stratum-specific ORs were similar. Thus,
increments), sex, current cigarette smoking, past cigarette
the final nonstratified models included only the a priori
smoking, RF status (positive/negative), anti-CCP antibody
status (positive/negative), baseline DAS28 (per unit increase),
The distribution of DAS28 units on a continuous scale
and baseline HAQ score (per unit increase), carriage of the
at the 3-month visit was compared between current smokers
HLA–DRB1 shared epitope (1 or 2 copies versus no copies),
and never smokers and between past smokers and never
and carriage of the PTPN22*R620W risk allele (1 or 2 copies
smokers by use of t-tests, as well as for each of the components
versus no copies), as well as disease duration for those who
of the DAS28 (swollen joint count, tender joint count, eryth-
received TNF inhibitor treatment. Age, sex, past smoking, and
rocyte sedimentation rate (ESR), patient’s assessment of
baseline DAS28 were included as potential confounders or a
global health status using a 100-mm visual analog scale [VAS])
priori covariates in all models. In addition, we included
by use of Wilcoxon’s rank sum test, since these parameters
concurrent use of prednisolone or nonsteroidal antiinflamma-
tory drugs (NSAIDs) in the models investigating the specific
Statistical analysis was performed using the SAS ver-
treatments. For the group starting TNF inhibitors during the
sion 9.1 software (SAS Institute). All tests were 2-sided, and
followup period, we also included disease duration at the start
the significance level was set at 0.05.
of TNF inhibitor treatment and concurrent use of MTX orother DMARDs. Furthermore, we considered the remainingbaseline parameters as potential confounders by assessing
whether their addition (one at a time) to the model containingsmoking and the a priori covariates altered the OR associated
Eligibility of patients for analyses. Patients who
with smoking by more than 10%. None of these factors
had available DAS28 data at baseline and were classifi-
materially altered the association with smoking. Through strat-
able as current, past, or never smokers constitute the
Figure 2. European League Against Rheumatism (EULAR) response in the overall EIRA cohort and in the subgroups receiving MTX or clinical care without a disease-modifying antirheumatic drug (DMARD) at baseline, as well as in those receiving TNF inhibitors later on, according to smoking status. Values are the proportion of patients achieving a good response according to the EULAR criteria at the 3-month visit divided by the number in the smoking category who had DAS28 data available at followup. Numbers across the bottom are the total number with DAS28 and smoking status data. P values were determined by univariate logistic regression. See Figure 1 for other definitions.
basis for all analyses (Figure 1). Baseline characteristics
ates at the 3-month followup visit (adjusted OR 0.61
of the study patients are shown in Table 1. Baseline
[95% CI 0.44–0.87]) (Figure 3, left) and was similar at
characteristics did not differ between RA patients with
later followup visits as compared with baseline (adjusted
and those without available DAS28 data.
ORs for the 6-month, 1-year, 2-year, and 5-year visits
Cigarette smoking and the chance of response.
0.65, 0.78, 0.66, and 0.61, respectively).
There was no indication that smokers were more likely
The influence of smoking did not differ signifi-
to be included in the SRR (data available upon request
cantly between anti-CCP–positive and anti-CCP–
Findings in the entire EIRA cohort irrespective
Current smokers were also less likely to achieve
of treatment. Overall, 1,430 EIRA patients were fol-
remission at the 3-month followup visit (adjusted OR
lowed in SRR from baseline; 1,418 of them had DAS28
0.60 [95% CI 0.40–0.88]) (Figure 3, right), and similar
data available at baseline (Figure 1), and 1,199 had
results were observed at all later followup visits (ad-
DAS28 data available at the 3-month visit (994 with
justed ORs for the 6-month, 1-year, 2-year, and 5-year
smoking status). At the 3-month visit, 32% were good
responders according to the EULAR criteria and 24%
The cumulative dose of smoking did not further
were in remission. At the 6-month visit, 1,124 had
add to the results among current smokers. Thus, no
DAS28 data available (952 with smoking status), and
association was observed between the number of pack-
42% of them had achieved a good response and 34%
years smoked and a good response according to the
EULAR criteria at the 3-month followup visit (adjusted
As shown in Figure 2, 26% of current smokers
OR per pack-year increase 1.00 [95% CI 0.98–1.02]).
(80 of 305) in the whole cohort achieved a good response
Findings in the patients starting MTX mono-
according to the EULAR criteria after 3 months, com-
therapy at baseline. A total of 873 patients started
pared with 35% of never smokers (123 of 349; P ϭ 0.01).
methotrexate (MTX) as the only DMARD treatment at
Past smokers had a similar chance of having a good
baseline. Of these, 865 had an available DAS28 measure
response (32% [110 of 340]) as never smokers (P ϭ 0.42).
at baseline (Figure 1), and 761 (626 with smoking status)
This decreased chance of a good response in
of those who had not changed their treatment before
current smokers remained after adjustment for covari-
followup had DAS28 data available at the 3-month
SMOKING AND RESPONSE OF EARLY RA TO MTX AND TNF INHIBITORS
Figure 3. Association between current smoking and a good response (left) or remission (right) according to the European League Against Rheumatism criteria in the overall group of EIRA patients. Values are the adjusted odds ratios with 95% confidence intervals (95% CIs) determined at the 3-month, 6-month, 1-year, 2-year, and 5-year followup visits, as calculated by multivariate logistic regression, adjusting for age, sex, past smoking, and baseline DAS28. Construction of the models and definition of the covariables are described in Patients and Methods. See Figure 1 for other definitions and numbers of patients in each group.
followup visit. We found that 33% were good responders
current smokers as compared with never smokers re-
according to the EULAR criteria, and 24% were in
mained in the multivariate model and was not influ-
remission. At the 6-month followup visit, 522 patients
enced by any of the covariates (adjusted OR 0.60 [95%
(436 with smoking data) had not changed their treat-
CI 0.39–0.94]) (Figure 4, left). Similar results for a good
ment and had available DAS28 data, and of that group,
response at the 6-month visit were observed (adjusted
48% had achieved good response and 39% were in
OR 0.58 [95% CI 0.36–0.94]). Current smokers also
tended to be less likely to be in remission after 3 months
After 3 months of MTX monotherapy, 27% of
(OR 0.66 [95% CI 0.40–1.08]) (Figure 4, right), and at
current smokers (54 of 197) had reached a EULAR
the 6-month followup visit, this was significant (OR 0.41
good response as compared with 36% of never smokers
(78 of 214; P ϭ 0.05) (Figure 2), whereas the frequency
Among current smokers, the number of pack-
of good response did not differ between past smokers
years smoked was not associated with the chance of good
(37% [79 of 215]) and never smokers (P ϭ 0.95).
response after 3 months (adjusted OR per pack-year
The decreased chance of a good response in
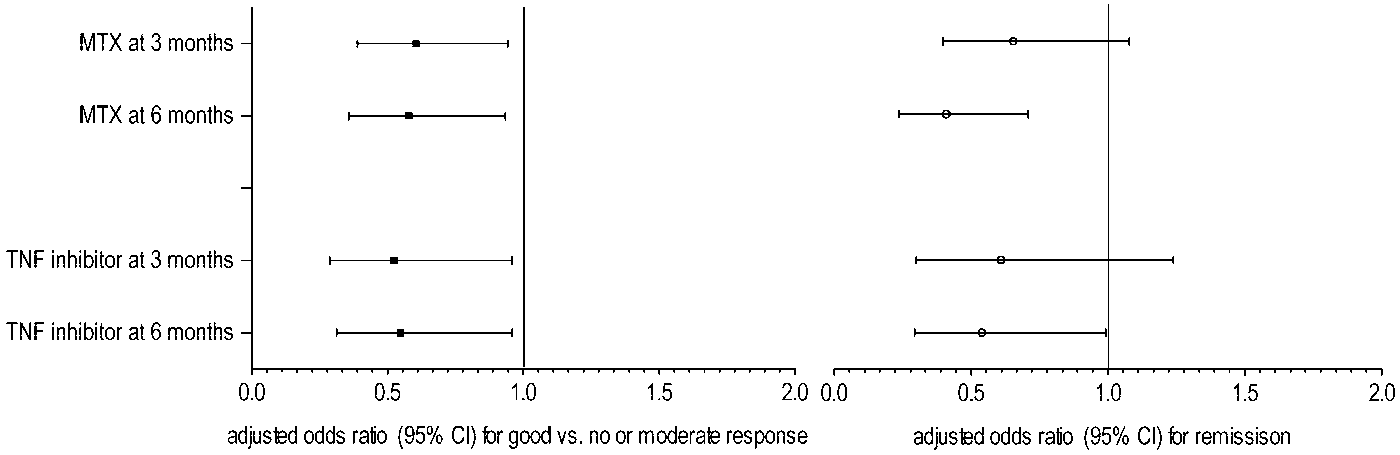
increase 0.99 [95% CI 0.98–1.02]). Figure 4. Association between current smoking and a good response (left) or remission (right) according to the European League Against Rheumatism criteria in patients starting MTX at baseline and in patients starting a TNF inhibitor as the first biologic agent. Values are the adjusted odds ratios with 95% confidence intervals (95% CIs) determined at the 3-month and the 6-month visits, as calculated by multivariate logistic regression, adjusting for age, sex, past smoking, DAS28 at diagnosis, and concurrent treatment with prednisolone, nonsteroidal antiinflammatory drugs, and in the TNF inhibitor–treated group, MTX. Construction of the models and definition of the covariables are described in Patients and Methods. See Figure 1 for other definitions and numbers of patients in each group.
The influence of smoking did not differ signifi-
cantly between anti-CCP–positive and anti-CCP–negative patients or between patients with and withoutconcurrent prednisolone treatment (data not shown).
None of the DAS28 components differed be-
tween current, past, and never smokers at baseline (datanot shown). However, consistent with the categorizedresults above for a good response and remission accord-ing to the EULAR criteria, current smokers had signif-icantly higher scores on the DAS28 as a continuousvariable than did never smokers (mean 4.10 versus 3.62;P ϭ 0.001) at the 3-month followup visit, whereas pastsmokers and never smokers had similar scores on theDAS28 (mean 3.65 versus 3.62; P ϭ 0.83). This alsoapplied to the individual components of the DAS28(Figure 5), where current smokers as compared withnever smokers had higher numbers of swollen joints(P ϭ 0.02) and tender joints (P ϭ 0.03), a higher ESR(P ϭ 0.008), and tended to have higher VAS score forthe patient’s assessment of global health (P ϭ 0.09) at3 months. These parameters were not significantly dif-ferent between past smokers and never smokers(swollen joint count P ϭ 0.47, tender joint count P ϭ0.64, erythrocyte sedimentation rate P ϭ 0.85, andVAS score for the patient’s assessment of global healthP ϭ 0.21). Findings in patients who did not start DMARD therapy at baseline. Eighteen percent of the patients who did not start any DMARD treatment at baseline (n ϭ 175) received oral prednisolone treatment, and 46% took NSAIDs regularly. At baseline, 158 of the patients had DAS28 data available, and at the 3-month followup visit, 129 had DAS28 data available (109 with smoking status). At the 3-month visit, 22% of these patients were classifiable as EULAR good responders and 21% were in remission. At the 6-month followup visit, 52 of those with available DAS28 data were still not receiving DMARD treatment, and of those, 27% were classifiable as EULAR good responders and 29% were in remission.
After 3 months, 14% of current smokers (4 of 28)
achieved a good response according to the EULARcriteria as compared with 34% of never smokers (15 of44; P ϭ 0.07), and past smokers had a significantly lowerchance of achieving a good response (14% [5 of 37])than did never smokers (P ϭ 0.04). The influence ofsmoking did not differ significantly between patients
Figure 5. Influence of smoking habits on individual components of
who did and those who did not receive prednisolone in
the DAS28 in patients receiving MTX or a TNF inhibitor, as deter-
this non–DMARD-treated group, although those who
mined at the 3-month followup visit. Data are shown as box plots. Eachbox represents the upper and lower interquartile range. Lines inside
received prednisolone were more likely to reach a good
the boxes represent the median. Whiskers represent the fifth percen-
tiles. P values are versus never smokers, as determined by Wilcoxon’srank sum test (significant at P Ͻ 0.05). VAS-global ϭ visual analogscale (0–100 mm) for the patient’s assessment of global health.
SMOKING AND RESPONSE OF EARLY RA TO MTX AND TNF INHIBITORS
Findings in the patients who later started a TNF
differ significantly between past smokers and never
inhibitor as the first biologic agent. By the end of the
followup period in 2007, a total of 535 patients whoentered the EIRA cohort during 1996–2006 had started
DISCUSSION
a TNF inhibitor, and 486 of these patients had DAS28data available at the start of treatment (Figure 1). The
In this population-based early RA cohort receiv-
median time from RA diagnosis to the start of a TNF
ing real-life care, we found that current smokers were
inhibitor was 3 years (interquartile range 1–5 years).
less likely to respond to MTX treatment and to TNF
Of the patients who had smoking status available, 199
inhibitor treatment. The decreased chance of response
received infliximab, 136 received etanercept, and 66
associated with current smoking in both treatment
received adalimumab. When pooled, 301 had DAS28
groups was observed for the primary end point of a good
data and smoking category available at the 3-month
response according to the EULAR criteria, for remis-
followup visit. Of these 301 patients, 38% were good
sion according to the EULAR criteria, and for the
responders and 28% were in remission. At the 6-month
DAS28 scores or the joint counts at followup and was
followup visit, 324 had DAS28 data available, and
not explained by other factors. The influence of current
44% had achieved a good response and 36% were in
smoking was similar at later followup visits and was also
observed for the overall group, without regard to which
Current smokers were less likely to respond well
treatment was used. On the other hand, past smoking
to TNF inhibitors after 3 months of therapy (29% [28 of
did not influence the chance of treatment response,although it seemed to have a negative effect in the group
98]) than never smokers were (43% [49 of 113]; P ϭ
that did not start DMARD treatment at baseline.
0.03), whereas past smokers (39% [35 of 90]) had a
Our findings provide new information concerning
similar frequency of good response as never smokers
the influence of smoking on the response to MTX
(P ϭ 0.52). The lower likelihood of a good response in
monotherapy and extend the information concerning
current smokers remained in the multivariate model
response to TNF inhibitors in patients with longstanding
after adjustment for covariates (adjusted OR 0.52 [95%
RA (15–17). Previous findings of smoking as a predictor
CI 0.29–0.96]). Findings were similar at the 6-month
of later disease activity in early RA or inflammatory
followup visit (adjusted OR 0.55 [95% CI 0.31–0.96]).
polyarthritis have been somewhat inconsistent, maybe
Using remission as the outcome measure showed a
due to the different treatments used, the outcome
tendency toward an association of current smoking with
measures, and the followup time points, which makes
remission after 3 months (adjusted OR 0.61 [95% CI
the study results difficult to compare (5,8–11,26). Thus,
0.30–1.24]), which was significant at the 6-month visit
we evaluated both the likelihood of a good response and
(adjusted OR 0.54 [95% CI 0.30–0.99]).
remission, which are recommended as outcome mea-
Among current smokers, the number of pack-
sures in the ACR and EULAR joint guidelines (20,21),
years smoked was not associated with the chance of good
and found similar results for current smoking up to 5
response after 3 months (adjusted OR per pack-year
years later, results which were independent of other
increase for current smokers 1.00 [95% CI 0.96–1.04]).
The influence of smoking did not differ signifi-
The strength of our study is that it is population-
cantly between anti-CCP–positive and anti-CCP–
based, using information about real-life care of patients
negative patients or between patients who were and
with early RA, with almost complete information about
those who were not receiving concurrent prednisolone
smoking habits. Compared with clinical trials, the find-
ings may have a higher external validity for routine care,
While none of the DAS28 components differed
since the only selection criteria applied were being
between the groups of current, past, and never smokers
between the ages of 18 and 70 years and having RA of
at baseline (data not shown), at the 3-month visit,
recent onset. The influence of smoking was studied in
current smokers had higher DAS28 scores than did
the context of the main treatment options of today, and
never smokers (P ϭ 0.003). As shown in Figure 5, this
most RA patients in whom these treatments were
also applied to the individual DAS28 components of
started should have been captured because of the
swollen joint count (P ϭ 0.002) and VAS score for the
population-based setting and high coverage of the EIRA
patient’s assessment of global health (P ϭ 0.01), whereas
and SRR registers. Other DMARDs used as part of
a trend was observed for the tender joint count (P ϭ
standard care during the study period (see Supplemen-
0.10) and the ESR (P ϭ 0.09). These parameters did not
tary Table 1, available on the Arthritis & Rheumatism
web site at http://onlinelibrary.wiley.com/journal/
years, many were lost to followup, partly because they
10.1002/(ISSN)1529-0131) were found in the whole co-
had not yet reached that time point and partly because
hort, but the numbers of patients receiving each of these
during the first years of the SRR and the EIRA study,
treatments were too low for a meaningful analysis in
clinicians were instructed to follow their RA cases for
only 2 years. Further, some patients were excluded
Another strength of the present study is that the
because they did not start their followup in the SRR at
information about smoking was detailed enough to
the time of EIRA inclusion. It should be noted, however,
permit analysis of both current and past smoking as well
that the findings were similar if all RA patients with
as of the number of pack-years. Furthermore, we had
followup data were kept in the analyses.
data on genetic risk factors (HLA–DRB1 shared epitope
This study did not intend to explore the reasons
and the PTPN22*620W risk allele) as well as serology
why smoking may have a negative effect on response to
(RF and anti-CCP antibodies) for analysis of eventual
treatment, but the following factors may be considered.
modifying effects of these factors, which have been
First, smoking may possibly be associated with refracto-
shown to interact with smoking in terms of the risk of
riness to medications because of pharmacokinetic (PK)
developing the seropositive form of RA and, in some but
or pharmacodynamic (PD) interactions. Accordingly, a
not all studies, have been reported to be associated with
recent study in RA patients showed that smokers had
response to MTX (27–30) or to TNF inhibitors (31,32).
lower concentrations of MTX polyglutamates, the active
The association estimates for current smoking, however,
metabolites retained in cells, which indicates that smok-
turned out to be unaffected by all covariates tested.
ers metabolize MTX differently (33). We did not ob-
The observational design of this study gives also
serve any influence of initial MTX dosage on the
rise to its main limitations. First, some patients stopped
response frequencies (data not shown). For TNF inhib-
the treatment, received alternative drugs, or received
itors, we are not aware of any studies on the influence of
additional drugs before the 3-month or 6-month fol-
lowup visit when treatment response was evaluated. The
Second, it may also be that smokers have a more
reason for changes in medications before the followup
persistent “natural” disease course of RA, irrespective
visit (lack of response, side effects, etc.) was not re-
of treatment. Since only 175 patients did not start any
corded, and those patients were therefore excluded from
DMARD treatment, only 52 of whom were not receiving
the analyses of individual treatment groups for that time
any DMARD after 6 months from inclusion, our power
point (see Figure 1). Thus, the numbers of patients with
to detect differences in disease course that were depen-
available data for an evaluation of treatment response
dent on smoking was limited. Thus, the observational
are likely to be selected on response since they contin-
setting of our study makes it impossible to determine
ued to take the same treatment, but a more conservative
whether it is the underlying disease that is made more
approach of keeping in the analyses all patients who
severe by smoking or whether smoking specifically af-
initiated each treatment yielded similar findings (data
fects response to therapy. From a clinical perspective, it
is important to know the impact of smoking on disease
Treatment changes also made it difficult to eval-
activity in individuals who are treated with MTX or TNF
uate the influence of smoking on the response to
inhibitors, irrespective of whether the effect of smoking
particular drugs after the 6-month followup. We did,
is mainly acting on the underlying disease course (which
however, evaluate the whole cohort at later followup
is then not compensated for by the treatment) or
visits to give an overall picture of the more long-term
whether the effect of smoking is specific for the actual
influence of smoking, which yielded similar findings of a
detrimental effect of smoking. For the TNF inhibitor–
Cigarette smoking is a well-known risk factor for
treated group, smoking information was retrieved from
the RA diagnosis, particularly in the subset of patients
the time of study entry. This may have introduced bias,
with anti-CCP antibodies (1), but the anti-CCP status
but our findings are consistent with those of previous
had no modifying effect on the association of current
smoking with response. Thus, the mechanisms through
Second, some patients were lost to followup in
which smoking influences susceptibility to RA and its
the SRR registry. This might affect the external validity
disease course, respectively, may differ.
of the results, especially if the smoking habits of those
In conclusion, our findings indicate that cigarette
who were lost to followup differed from those who were
smokers have a diminished chance of responding well to
not, but this was not the case (data not shown). After 2
the currently first- and second-line agents of choice in
SMOKING AND RESPONSE OF EARLY RA TO MTX AND TNF INHIBITORS
early RA treatment today: MTX and TNF inhibitors,
REFERENCES
respectively. This was also observed in the whole group
1. Klareskog L, Catrina AI, Paget S. Rheumatoid arthritis. Lancet
of RA patients during the first years, indicating that
smokers have a more persistent disease activity irrespec-
2. De Vries-Bouwstra JK, Goekoop-Ruiterman YP, Verpoort KN,
tive of which treatment is used. These findings support
Schreuder GM, Ewals JA, Terwiel JP, et al. Progression of jointdamage
the idea that smoking should be taken into account when
HLA–DRB1, rheumatoid factor, and anti–citrullinated protein
trying to predict response to antirheumatic agents.
antibodies in relation to different treatment strategies. Arthritis
Whether discontinuation of smoking prior to initiating
3. Anderson JJ, Wells G, Verhoeven AC, Felson DT. Factors
treatment is beneficial, as suggested by the observation
predicting response to treatment in rheumatoid arthritis: the
that past smokers responded equally well to treatment as
importance of disease duration. Arthritis Rheum 2000;43:22–9.
those who had never smoked, remains to be studied
4. Klarenbeek NB, Allaart CF, Kerstens PJ, Huizinga TW, Dijkmans
BA. The BeSt story: on strategy trials in rheumatoid arthritis. Curr
further. Meanwhile, the findings provide a strong impe-
tus for clinicians to include measures against smoking as
5. Westhoff G, Rau R, Zink A. Rheumatoid arthritis patients who
a fundamental part of the therapeutic armamentarium
smoke have a higher need for DMARDs and feel worse, but theydo not have more joint damage than non-smokers of the same
serological group. Rheumatology (Oxford) 2008;47:849–54.
6. Turesson C, O’Fallon WM, Crowson CS, Gabriel SE, Matteson
EL. Extra-articular disease manifestations in rheumatoid arthritis:
ACKNOWLEDGMENTS
incidence trends and risk factors over 46 years. Ann Rheum Dis2003;62:722–7.
We thank all of the participating control subjects and
7. Nyhall-Wahlin BM, Petersson IF, Nilsson JA, Jacobsson LT,
RA patients, as well as the following people who recruited
Turesson C, and the BARFOT study group. High disease activity
patients for EIRA, along with their collaborating clinicians and
disability burden and smoking predict severe extra-articular man-
nurses: Ingeli Andreasson (Landvetter); Eva Baecklund (Aka-
ifestations in early rheumatoid arthritis. Rheumatology (Oxford)
demiska Hospital); Ann Bengtsson and Thomas Skogh (Linko-
ping Hospital); Johan Bratt, Ingiald Hafstrom, and Birgitta
8. Wolfe F. The effect of smoking on clinical, laboratory, and
Nordmark (Karolinska University Hospital); Kjell Huddenius
radiographic status in rheumatoid arthritis. J Rheumatol 2000;27:
(Rheumatology Clinic, Stockholm); Shirani Jayawardene
9. Papadopoulos NG, Alamanos Y, Voulgari PV, Epagelis EK,
(Bollnas Hospital); Ann Knight (Hudiksvall Hospital and
Tsifetaki N, Drosos AA. Does cigarette smoking influence disease
Uppsala University Hospital); Ido Leden (Kristianstad Hospi-
expression, activity and severity in early rheumatoid arthritis
tal); Goran Lindahl (Danderyd Hospital); Bengt Lindell (Kal-
patients? Clin Exp Rheumatol 2005;23:861–6.
mar Hospital); Christine Lindstrom and Gun Sandahl (Sophia-
10. Manfredsdottir VF, Vikingsdottir T, Jonsson T, Geirsson AJ,
hemmet); Bjorn Lofstrom (Katrineholm Hospital); Ingemar
Kjartansson O, Heimisdottir M, et al. The effects of tobacco
Petersson (Spenshult Hospital); Christoffer Schaufelberger
smoking and rheumatoid factor seropositivity on disease activity
(Sahlgrenska University Hospital); Patrik Stolt (Vasteras Hos-
and joint damage in early rheumatoid arthritis. Rheumatology
pital); Berit Sverdrup (Eskilstuna Hospital); Olle Svernell
(Vastervik Hospital); and Tomas Weitoft (Gavle Hospital).
11. Harrison BJ, Silman AJ, Wiles NJ, Scott DG, Symmons DP. The
association of cigarette smoking with disease outcome in patients
We thank Marie-Louise Serra and Lena Nise for excellent
with early inflammatory polyarthritis. Arthritis Rheum 2001;44:
collection of the data as part of EIRA, Dr. Leonid Padyukov
for providing the HLA–DRB1 data, Prof. Ronald van Vollen-
12. Saag KG, Cerhan JR, Kolluri S, Ohashi K, Hunninghake GW,
hoven for critical reading of the manuscript, and Drs. Jing Cui
Schwartz DA. Cigarette smoking and rheumatoid arthritis sever-
¨m for methodologic discussions. We are also
indebted to the Swedish Rheumatology Register and ARTIS
13. Finckh A, Dehler S, Costenbader KH, Gabay C. Cigarette smok-
groups, and last, but not least, we thank all of the clinicians
ing and radiographic progression in rheumatoid arthritis. Ann
who have followed the cases of the registry patients over the
14. Wessels JA, van der Kooij SM, le Cessie S, Kievit W, Barerra P,
Allaart CF, et al, for the Pharmacogenetics Collaborative Re-search Group. A clinical pharmacogenetic model to predict the
AUTHOR CONTRIBUTIONS
efficacy of methotrexate monotherapy in recent-onset rheumatoidarthritis. Arthritis Rheum 2007;56:1765–75.
All authors were involved in drafting the article or revising it
15. Hyrich KL, Watson KD, Silman AJ, Symmons DP. Predictors of
critically for important intellectual content, and all authors approved
response to anti-TNF-␣ therapy among patients with rheumatoid
the final version to be published. Dr. Saevarsdottir had full access to all
arthritis: results from the British Society for Rheumatology Bio-
of the data in the study and takes responsibility for the integrity of the
logics Register. Rheumatology (Oxford) 2006;45:1558–65.
data and the accuracy of the data analysis.
16. Abhishek A, Butt S, Gadsby K, Zhang W, Deighton CM. Anti-
Study conception and design. Saevarsdottir, Wedre
TNF-␣ agents are less effective for the treatment of rheumatoid
arthritis in current smokers. J Clin Rheumatol 2010;16:15–8. Acquisition of data. Saevarsdottir, Wedre
17. Mattey DL, Brownfield A, Dawes PT. Relationship between
pack-year history of smoking and response to tumor necrosis
Analysis and interpretation of data. Saevarsdottir, Bengtsson, Wesley,
factor antagonists in patients with rheumatoid arthritis. J Rheu-
18. Arnett FC, Edworthy SM, Bloch DA, McShane DJ, Fries JF,
ations with rheumatoid arthritis in Ͼ4,000 samples from North
Cooper NS, et al. The American Rheumatism Association 1987
America and Sweden: association of susceptibility with PTPN22,
revised criteria for the classification of rheumatoid arthritis.
CTLA4, and PADI4. Am J Hum Genet 2005;77:1044–60.
26. Forslind K, Hafstrom I, Ahlmen M, Svensson B. Sex: a major
19. Askling J, Fored CM, Geborek P, Jacobsson LT, van Vollenhoven
predictor of remission in early rheumatoid arthritis? Ann Rheum
R, Feltelius N, et al. Swedish registers to examine drug safety and
clinical issues in RA. Ann Rheum Dis 2006;65:707–12.
27. Criswell LA, Lum RF, Turner KN, Woehl B, Zhu Y, Wang J, et al.
20. Aletaha D, Landewe R, Karonitsch T, Bathon J, Boers M,
The influence of genetic variation in the HLA–DRB1 and
Bombardier C, et al. Reporting disease activity in clinical trials of
LTA–TNF regions on the response to treatment of early rheuma-
patients with rheumatoid arthritis: EULAR/ACR collaborative
toid arthritis with methotrexate or etanercept. Arthritis Rheum
recommendations. Ann Rheum Dis 2008;67:1360–4.
21. Van Gestel AM, Prevoo ML, van ’t Hof MA, van Rijswijk MH, van
28. Hider SL, Silman AJ, Thomson W, Lunt M, Bunn D, Symmons
de Putte LB, van Riel PL. Development and validation of the
DP. Can clinical factors at presentation be used to predict
European League Against Rheumatism response criteria for rheu-
outcome of treatment with methotrexate in patients with early
matoid arthritis: comparison with the preliminary American Col-
inflammatory polyarthritis? Ann Rheum Dis 2009;68:57–62.
lege of Rheumatology and the World Health Organization/
29. O’Dell JR, Nepom BS, Haire C, Gersuk VH, Gaur L, Moore GF,
International League Against Rheumatism criteria. Arthritis
et al. HLA-DRB1 typing in rheumatoid arthritis: predicting re-
sponse to specific treatments. Ann Rheum Dis 1998;57:209–13.
22. Ronnelid J, Wick MC, Lampa J, Lindblad S, Nordmark B,
30. Van Dongen H, van Aken J, Lard LR, Visser K, Ronday HK,
Klareskog L, et al. Longitudinal analysis of citrullinated protein/
Hulsmans HM, et al. Efficacy of methotrexate treatment in
peptide antibodies (anti-CP) during 5 year follow up in earlyrheumatoid arthritis: anti-CP status predicts worse disease activity
patients with probable rheumatoid arthritis: a double-blind, ran-
and greater radiological progression. Ann Rheum Dis 2005;64:
domized, placebo-controlled trial. Arthritis Rheum 2007;56:
23. Padyukov L, Silva C, Stolt P, Alfredsson L, Klareskog L, for the
31. Plenge RM. Recent progress in rheumatoid arthritis genetics: one
Epidemiological Investigation of Rheumatoid Arthritis Study
step towards improved patient care. Curr Opin Rheumatol 2009;
Group. A gene–environment interaction between smoking and
shared epitope genes in HLA–DR provides a high risk of seropos-
32. Potter C, Hyrich KL, Tracey A, Lunt M, Plant D, Symmons DP, et
itive rheumatoid arthritis. Arthritis Rheum 2004;50:3085–92.
al. Association of rheumatoid factor and anti-cyclic citrullinated
24. Klareskog L, Stolt P, Lundberg K, Kallberg H, Bengtsson C,
peptide positivity, but not carriage of shared epitope or PTPN22
Grunewald J, et al, and the Epidemiological Investigation of
susceptibility variants, with anti-tumour necrosis factor response in
Rheumatoid Arthritis Study Group. A new model for an etiology
rheumatoid arthritis. Ann Rheum Dis 2009;68:69–74.
of rheumatoid arthritis: smoking may trigger HLA–DR (shared
33. Stamp LK, O’Donnell JL, Chapman PT, Zhang M, Frampton C,
epitope)–restricted immune reactions to autoantigens modified by
James J, et al. Determinants of red blood cell methotrexate
citrullination. Arthritis Rheum 2006;54:38–46.
polyglutamate concentrations in rheumatoid arthritis patients re-
25. Plenge RM, Padyukov L, Remmers EF, Purcell S, Lee AT,
ceiving long-term methotrexate treatment. Arthritis Rheum 2009;
Karlson EW, et al. Replication of putative candidate-gene associ-
2010-2011 Dille Fund For Excellence Grant Recipients The Grant committee received 22 proposals requesting a total of $36,049.85 and was able to award only $6,000, supporting 14 projects. This year’s committee members included: Teri Walseth (Dean of Education & Human Services), Joan Justesen (Vice President Alumni Foundation), Brittney Goodman (Associate Vice President for Instruction
The red secTion The Myth of Statin-Induced Hepatotoxicity Am J Gastroenterol 2010;105:978–980; doi:10.1038/ajg.2010.102Statin-induced hepatotoxicity is a myth. cebo trial with a median follow-up of 5 years have a 1.13% incidence of liver test abnor-“Myth” is used here to mean a false collec-randomized 6,500 subjects to drug and pla-malities vs. 0.29% with placebo ( P = 0.04) ti
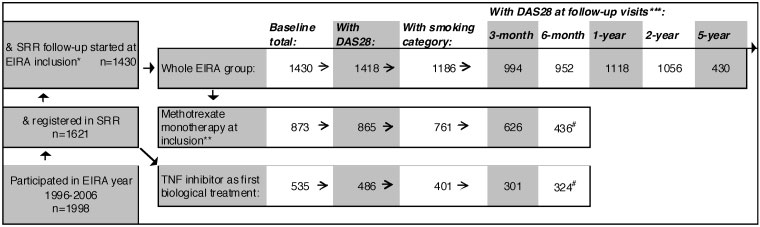 Figure 1. Flow chart showing the distribution of rheumatoid arthritis (RA) patients who entered the Epidemiological Investigation
Figure 1. Flow chart showing the distribution of rheumatoid arthritis (RA) patients who entered the Epidemiological Investigation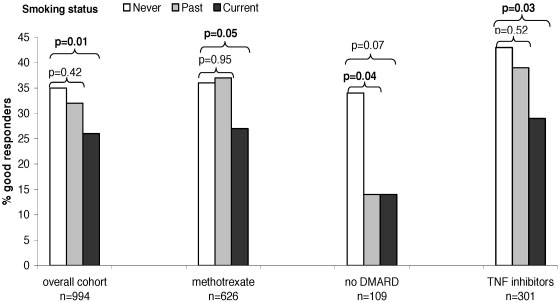 Figure 2. European League Against Rheumatism (EULAR) response in the overall EIRA cohort
Figure 2. European League Against Rheumatism (EULAR) response in the overall EIRA cohort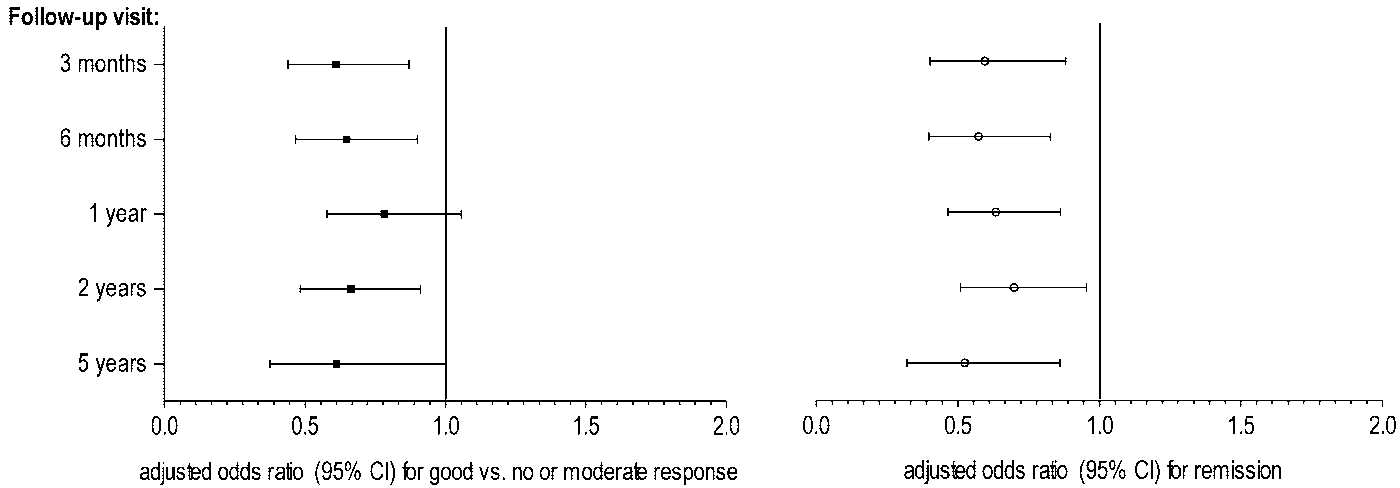
 SMOKING AND RESPONSE OF EARLY RA TO MTX AND TNF INHIBITORS
Figure 3. Association between current smoking and a good response (left) or remission (right)
SMOKING AND RESPONSE OF EARLY RA TO MTX AND TNF INHIBITORS
Figure 3. Association between current smoking and a good response (left) or remission (right)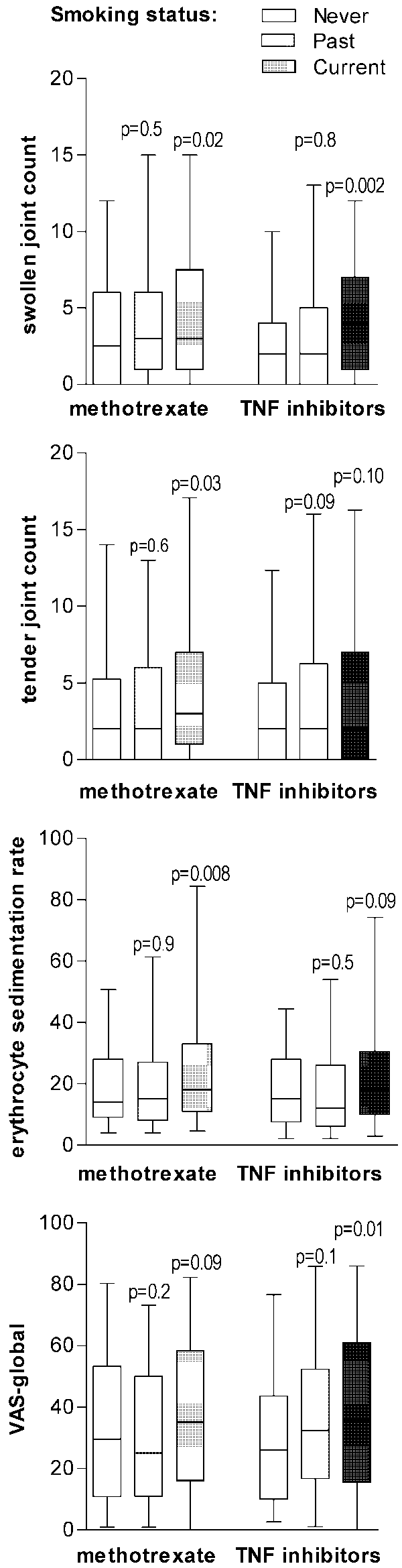 The influence of smoking did not differ signifi-
cantly between anti-CCP–positive and anti-CCP–negative patients or between patients with and withoutconcurrent prednisolone treatment (data not shown).
The influence of smoking did not differ signifi-
cantly between anti-CCP–positive and anti-CCP–negative patients or between patients with and withoutconcurrent prednisolone treatment (data not shown).