Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
1471-2288-8-72.fm
BMC Medical Research Methodology
Research article Use of the Oxford Handicap Scale at hospital discharge to predict Glasgow Outcome Scale at 6 months in patients with traumatic brain injury Pablo Perel*, Phil Edwards, Haleema Shakur and Ian Roberts
Address: Department of Epidemiology and Population Health, London School of Hygiene & Tropical Medicine, London, UK
Email: Pablo Perel* - pablo.perel@lshtm.ac.uk; Phil Edwards - phil.edwards@lshtm.ac.uk; Haleema Shakur - haleema.shakur@lshtm.ac.uk; Ian Roberts - ian.roberts@lshtm.ac.uk
Received: 24 June 2008Accepted: 6 November 2008
BMC Medical Research Methodology 2008, 8:72
2008 Perel et al; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract Background: Traumatic brain injury (TBI) is an important cause of acquired disability. In evaluating the effectiveness of clinical interventions for TBI it is important to measure disability accurately. The Glasgow Outcome Scale (GOS) is the most widely used outcome measure in randomised controlled trials (RCTs) in TBI patients. However GOS measurement is generally collected at 6 months after discharge when loss to follow up could have occurred. The objectives of this study were to evaluate the association and predictive validity between a simple disability scale at hospital discharge, the Oxford Handicap Scale (OHS), and the GOS at 6 months among TBI patients. Methods: The study was a secondary analysis of a randomised clinical trial among TBI patients (MRC CRASH Trial). A Spearman correlation was estimated to evaluate the association between the OHS and GOS. The validity of different dichotomies of the OHS for predicting GOS at 6 months was assessed by calculating sensitivity, specificity and the C statistic. Uni and multivariate logistic regression models were fitted including OHS as explanatory variable. For each model we analysed its discrimination and calibration. Results: We found that the OHS is highly correlated with GOS at 6 months (spearman correlation 0.75) with evidence of a linear relationship between the two scales. The OHS dichotomy that separates patients with severe dependency or death showed the greatest discrimination (C statistic: 84.3). Among survivors at hospital discharge the OHS showed a very good discrimination (C statistic 0.78) and excellent calibration when used to predict GOS outcome at 6 months. Conclusion: We have shown that the OHS, a simple disability scale available at hospital discharge can predict disability accurately, according to the GOS, at 6 months. OHS could be used to improve the design and analysis of clinical trials in TBI patients and may also provide a valuable clinical tool for physicians to improve communication with patients and relatives when assessing a patient's prognosis at hospital discharge. Trial Registration Number: ISRCTN74459797 (page number not for citation purposes)BMC Medical Research Methodology 2008, 8:72
http://www.biomedcentral.com/1471-2288/8/72
Background
form of the OHS was used in which moderate handicap
Traumatic brain injury (TBI) is an important cause of
and moderately severe handicap were combined.
acquired disability. In evaluating the effectiveness of clin-
Although the OHS has been previously used in brain
ical interventions for TBI it is important to measure disa-
injury trials, its association with GOS at 6 months in TBI
bility accurately. The Glasgow Outcome Scale (GOS) is
patients has not been previously reported.[
the most widely used outcome measure in randomisedcontrolled trials (RCTs) in TBI patients.[ However,
The aim of this paper is to describe the association
because the GOS assesses how well patients function in
between an early disability outcome (OHS), and a 6
their daily social interactions, it is only applicable after the
months disability outcome (GOS). Specifically the objec-
patient has been discharged from hospital.
Loss to follow up after hospital discharge is a common
1) Evaluate the correlation between OHS at hospital dis-
problem in clinical trials in TBI and some amount of miss-
ing data is often unavo] If an early outcomemeasure was available that could predict long term disa-
2) Evaluate different dichotomies of the OHS at hospital
bility, it could be valuable for dealing with missing data,
and might potentially be used as a surrogate outcome.
3) Evaluate the extent to which OHS at hospital discharge
The MRC CRASH Trial was a large, randomised placebo
controlled trial of the effects of a 48-hour infusion of cor-ticosteroids on death and disability, among 10,008
ad] Using data from this cohort of patients we have
Potential predictor
previously identified hospital admission variables that
The OHS (tables assessed at 14 days, hospital dis-
accurately predict 6 months GO This cohort also
charge or death (whichever occur first).
presents an opportunity to evaluate the predictive validityof an early disability outcome measure for TBI patients. A
Variables that have previously been reported to be associ-
modified version of the Oxford Handicap Scale (OHS)
ated with the outcome were considered as potential con-
was completed at hospital discharge and the GOS was
founders and included in an adjusted model: age,
completed at 6 months after injury. The OHS, which was
Glasgow Coma Scale (GCS) at randomization, pupil reac-
originally developed for stroke patients, comprises six cat-
tivity, whether the patient sustained a major extra cranial
egories: no symptoms, minor symptoms, minor handi-
injury and computerised tomography (CT) scan
cap, moderate handicap, moderately severe handicap, and
Table 1: Original Oxford Handicap Scale and OHS used in the MRC CRASH Trial Original OHS Modified OHS used in CRASH Categories Categories
Minor symptoms that do not interfere with lifestyle
Minor handicap, symptoms that lead to some restriction in lifestyle but do not interfere with
Some restriction in lifestyle but independent
the patient's capacity to look after himself
Moderate handicap, symptoms that significantly restrict lifestyle and prevent totally independent
Dependent but not requiring constant attention
Moderately severe handicap, symptoms that clearly prevent independent existence though not needing constant attention
Severe handicap, totally dependent patient requiring constant attention night and day
Fully dependent requiring attention day and night
(page number not for citation purposes)BMC Medical Research Methodology 2008, 8:72
http://www.biomedcentral.com/1471-2288/8/72
418 no dat a on GOS at 6 m ont hs
Sa m p l e f o r o b j e ct i v e s 1 a n d 2
Flowchart of patients used in the analysis. Outcome
sent waiver and others consent from a legal representative.
The outcome was GOS at 6 months. The GOS comprises
We always adhered to these requirements.
five categories: death, persistent vegetative state, severedisability, moderate disability and good re
Of 10,008 study participants enrolled in the MRC CRASH
was dichotomised for analysis in the CRASH Trial into
Trial, 99 (1%) had missing data on the OHS, 418 (4.2%)
favourable outcome (good recovery or moderate disabil-
had missing data on the GOS at 6 months, and 36 (0.3%)
ity) and unfavourable outcome (severe disability, persist-
had missing data for both OHS and GOS. A further 8
ent vegetative state or death). We created two further
patients were excluded from analysis as they had a Glas-
dichotomies: good recovery versus other outcomes, and
gow Coma Scale (GCS) score of 15 at randomisation.
Analysis for objectives 1 and 2 were therefore performedusing data for 9,447 (94.4%) patients (fige
The sample of patients
third objective (predictive validity of OHS among survi-
The MRC CRASH trial was a large international double-
vors), the 1,948 patients who died within 14 days of
blind randomised placebo-controlled trial of the effect of
admission were excluded and the analysis was based on
early administration of a 48-h infusion of a corticosteroid
data for the remaining 7,499 patients (figure
(methylprednisolone) on the risk of death and disabilityafter TBI. The characteristics of the patients randomised,
Analysis
and results of the trial have already been reported in
de, Briefly, adults (aged 16 years or older) with a
A cross-tabulation between the OHS and GOS categories
head injury and a GCS of 14 or less were randomly allo-
was performed. Their relation was assessed with the Spear-
cated to commence either a 48 hour infusion of methyl-
prednisolone or matching placebo within eight hours ofinjury; patients from 239 hospitals in 48 countries were
randomised. All collaborating MRC CRASH investigators
The validity of the different dichotomies of the OHS for
were required to secure local ethics or research committee
predicting GOS at 6 months was assessed by calculating
approval before recruitment could begin. Patients with
sensitivity, specificity and the c statistic (an equivalent
clinically significant head injury are unable to give valid
concept to area under the receiver operator characteristic
informed consent. Local ethics committees set consent
procedures for participating hospitals. Some allowed con-
(page number not for citation purposes)BMC Medical Research Methodology 2008, 8:72
http://www.biomedcentral.com/1471-2288/8/72
(37.3%) patients were severely disabled or had died. Most
A logistic regression model was first fitted including only
deaths (84%) occurred within the first 14 days. OHS at 14
OHS as explanatory variables (model 1). A second model
days and GOS at 6 months were highly correlated (Spear-
was then fitted that also included demographic and clini-
man rank correlation coefficient 0.75) and they showed a
cal variables (model 2). Finally, a third model was fitted
that included all variables in model 2, plus CT scan varia-bles. All the demographic, clinical and CT variables have
OHS for predicting 6 months outcome
been previously reported as being independently associ-
Five dichotomies of the OHS were consider
ated with unfavourable outcome at 6 months.[ eachmodel we analysed its discrimination using the c statistic
When their validity was assessed in relation to unfavoura-
and calibration (graphically and with the Hosmer-Leme-
ble outcome as defined by the GOS (severe disability or
death), dichotomy D showed the highest discrimination(c statistic) with high specificity (Table
We then estimated the positive predictive value (with 95%confidence intervals) of each OHS category for GOS at 6
Among survivors at hospital discharge the OHS showed a
strong association with GOS at 6 months. The crude anal-ysis showed that patients who were fully dependent at 14
days had 24 higher odds of an unfavourable outcome at 6
General characteristics of the population
months. Although adjusting for known prognostic factors
Taows the characteristics of the sample included in
attenuated the strength of the association, OHS remained
the analysis. At 14 days 1,863 (19%) were dependent and
a strong predictor with a highly statistically significant test
1,948 patients had died (21%). At 6 months, 3,525
between Oxford Handicap Scale and unfavourable outcome (GOS) at 6 months
Relationship between Oxford Handicap Scale and unfavourable outcome (GOS) at 6 months. (page number not for citation purposes)BMC Medical Research Methodology 2008, 8:72
http://www.biomedcentral.com/1471-2288/8/72
Table 2: Glasgow Outcome Scale at 6 months by Oxford Handicap Scale at 14 days Glasgow Outcome Scale at 6 months Oxford Handicap Scale at 14 days Good recovery Severe disability Total Some restriction in lifestyle but independentDependent but not requiring constant attentionFully dependent requiring attention day & night
OHS showed very good discrimination and excellent cali-
hospital discharge the OHS showed a very good discrimi-
nation and excellent calibration when used to predictGOS outcome at 6 months.
Ta shows the prediction of different 6 months out-comes (as measured with GOS) according to the hospital
Strengths and weakness of the study
discharge OHS. For example, a patient with minor symp-
To our knowledge this is the first study that evaluated the
toms at hospital discharge will have a probability of
predictive validity of a simple scale for disability at hospi-
approximately 67% of good recovery, 89% of good recov-
tal discharge in TBI patients. The main strengths of our
ery or moderate disability and 98% of survival at 6
study include the large sample size which ensures preci-
sion in our estimates, and the inclusion of patients fromboth high and low & middle income countries, which
Discussion
increases the generalizability of our conclusions. The
Principal findings
main limitation is that the measurement of OHS was not
We found that the OHS is highly correlated with GOS at 6
standardized between centres. However, because we
months with evidence of a linear relationship between the
would expect that any measurement error would result in
two scales. The OHS dichotomy that separate patients
non-differential misclassification, in general we would
who were severely dependent or dead (dichotomy D)
expect that the association reported would be underesti-
showed the greatest discrimination. Among survivors at
mated rather than overestimated. Finally, our study is the
Table 3: Dichotomies of OHS for determining unfavourable outcome Some restriction in lifestyle but independentDependent but not requiring constant attentionFully dependent requiring attention day and night(page number not for citation purposes)BMC Medical Research Methodology 2008, 8:72
http://www.biomedcentral.com/1471-2288/8/72
Table 4: Validity of the Oxford Handicap Scale at 14 days for Glasgow Outcome Scale at 6 months
first to report this association which should therefore beexamined in an external cohort of patients in order to con-
Calibration of model 1. Comparison with other studies The incidence of unfavourable GOS outcome at 6 months Conclusion
in our cohort was lower in comparison to one reported in
We have shown that OHS is strongly related and predicts
a series of TBI coho] However, unlike ours, most of
accurately the GOS at 6 months. It may therefore be help-
these cohorts had been restricted to severe TBI patients.
ful in tackling the problem of missing data in clinical trials
The OHS has previously been used in RCTs of brain injury
in TBI. It might also serve as a potential surrogate outcome
patients, and Bamford et al. reported good inter-observer
measure and this application should be explored in fur-
agreement (a weighted kappa of 0.72] Ours is the first
ther studies. If our findings are replicated, OHS could be
study in TBI which has evaluated the relationship between
a simple and useful outcome measure to use in trials in
OHS and GOS. Nevertheless, previous studies have shown
settings for which long term follow-up is problematic.
a good agreement between the Modified Rankin Scale (the
Furthermore, OHS could be a useful variable to collect in
scale from which the OHS was derived) and the
rehabilitation trials in TBI patients to ensure that there isa similar distribution of disability among participants
Table 5: Association between OHS and unfavourable outcome (GOS) among survivors Model 1 Model 3
Some restriction in lifestyle but independent
Dependent but not requiring constant attention
Fully dependent requiring attention day & night
Model 1: OHSModel 2: model 1 plus GCS, pupil reactivity, major extra-cranial injury and ageModel 3: model 2 plus CT findings (petechial haemorrhages, obliteration of the third ventricle or basal cisterns, subarachnoid bleed, midline shift, non evacuated haematoma)
(page number not for citation purposes)BMC Medical Research Methodology 2008, 8:72
http://www.biomedcentral.com/1471-2288/8/72
Table 6: Prediction of three dichotomies of GOS at 6 months according to OHS Good recovery or Moderate disabilityMinor symptoms
Some restriction in lifestyle but independent
Dependent but not requiring constant attention
Fully dependent requiring attention day & night
Maas AI, Marmarou A, Murray GD, Teasdale SG,
between groups at baseline. We have also shown that,
among survivors, the OHS is able to predict disability at 6
J Neurotrauma 2007, 24(2):232-238.
Tilley BC, Marler J, Geller NL, Lu M, Legler J, Brott T, Lyden P, Grotta
months and thus may provide a valuable clinical tool for
physicians to improve communication with patients and
relatives when assessing a patient's prognosis at hospital
Stroke 1996, 27(11):2136-2142. Pre-publication history Competing interests
The pre-publication history for this paper can be accessed
The authors declare that they have no competing interests. Authors' contributions
ww.biomedcentral.com/1471-2288/8/72/prepub
PP designed the study, performed the analysis and pre-pared the manuscript. IR conceived the study, revised anddrafted the manuscript. PE and HS revised and drafted themanuscript. Acknowledgements The authors express their gratitude to all of the study participants and all the collaborators from the MRC CRASH Trial. We also want to thank Taemi Kawahara for helping with the tables and figures. References 1.
Bullock MR, Merchant RE, Choi SC, Gilman CB, Kreutzer JS, Marma- rou A, Teasdale GM: Neurosurg Focus 2002, 13(1):ECP1.
Dickinson K, Bunn F, Wentz R, Edwards P, Roberts I: BMJ 2000, 320(7245):1308-1311.
scientist can read your work free of charge
"BioMed Central will be the most significant development for
2005, 365(9475):1957-1959. disseminating the results of biomedical researc h in our lifetime."
CRASH Trial Collaborators: Predicting outcome after trau- matic brain injury: practical prognostic models based on large cohort of international patients.BMJ 2008, 12:12.
Bamford JM, Sandercock PA, Warlow CP, Slattery J:
available free of charge to the entire biomedical community
Stroke 1989, 20(6):828.
peer reviewed and published immediately upon acceptance
Jennett B, Bond M: Lancet 1975, 1(7905):480-484.
cited in PubMed and archived on PubMed Central
Lancet 2004, 364(9442):1321-1328. (page number not for citation purposes)
Matrix metalloproteinase Matrix metalloproteinases Collectively they are capable of degrading all kinds of molecules. They are known to be involved inin/activation. MMPs are also thought to play a major role on cell behaviors such as. They are distinguished from other endopeptidases by their s were described by Jermome Gross and Charles Lapiere (1962) who observed triple helix degrada
ORAL-VIEW™ Saliva Multi-Drug of Abuse Test One Step Assay PRINCIPLE OF THE PROCEDURE Rapid Visual Results For Forensic Use Only The ORAL-VIEW™ Saliva Multi-Drug of Abuse Test is a one-step lateral flow chromatographic immunoassay based on the principle of INTENDED USE competition for limited antibody binding sites between the drug in the The ORAL-VIEW™ Saliva M
 BMC Medical Research
BMC Medical Research 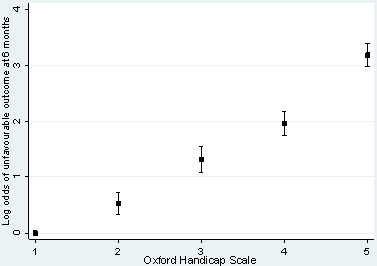 BMC Medical Research Methodology 2008, 8:72
BMC Medical Research Methodology 2008, 8:72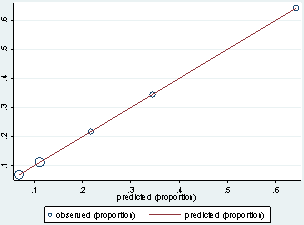 BMC Medical Research Methodology 2008, 8:72
BMC Medical Research Methodology 2008, 8:72