Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Maxprep_gense07
PRINTER-FRIENDLY VERSION AT GASTROENDONEWS.COM • Department of Medicine (Gastroenterology)Department of Medicine (Gastroenterology)The Mount Sinai School of MedicineThe Mount Sinai School of Medicine
Furthermore, suboptimal bowel preparation leads to
prolonged procedure times, lower rates of cecal intuba-
tion, reduced screening intervals, higher screeningcosts, and possibly, an increased risk for procedure-
related complications. Consequently, the adoption of
Tcancer is highly dependent upon more effective methods of bowel cleansing and a
greater emphasis on patient compliance with prepara-
tion instructions will improve the effectiveness and effi-ciency of colonoscopy, as well as minimize the risk for
Bowel Preparations
The available purgatives for colonoscopy can be clas-
sified into 1 of 3 categories: osmotic agents, polyethyl-
ene glycol–based (PEG) solutions, and stimulants. Osmotic laxatives increase intraluminal water by pro-
examinations, results in missed adenomas.1
moting the passage of extracellular fluid across thebowel wall. Examples of osmotic preparations includesodium phosphate (NaP), magnesium citrate, and man-nitol. The PEG-based solutions consist of a high molec-ular weight nonabsorbable polymer in a dilute elec-trolyte solution. PEG solutions are designed to beosmotically balanced, limiting the exchange of fluid andelectrolytes across the colonic membrane. Stimulantlaxatives work by increasing smooth muscle activitywithin the wall of the colon. Examples of stimulantpurgatives include senna, bisacodyl, and sodium pico-sulfate. Dietary modification, consisting of a clear liquidor a low fiber diet for 24 hours prior to the procedure, is
G A S T R O E N T E R O L O G Y & E N D O S C O P Y N E W S S P E C I A L E D I T I O N • 2 0 0 7
usually combined with a purgative regimen. This section
gastric outlet obstruction, high-grade small bowel
provides a brief overview of the available purgatives for
obstruction, and suspected bowel perforation.
bowel preparation (Table). Several comprehensivereviews on the comparative efficacy, safety, and tolera-
bility of these agents have recently been published, and
Oral NaP solution (Fleet Phospho-soda Oral Saline
readers wanting a more in-depth analysis of this subject
Laxative, CB Fleet) contains monobasic and dibasic
sodium phosphate, and is usually administered as 2, 45-mL doses 10 to 12 hours apart. Patients are instructed to
consume significant quantities of liquid (64 oz) during
A variety of PEG-based lavage regimens are current-
the preparation in order to prevent dehydration and
ly available for bowel cleansing prior to colonoscopy.
electrolyte disturbances. The mean onset and duration
These preparations differ with respect to volume of
of bowel activity following ingestion of the first dose is
lavage solution, electrolyte content, molecular weight of
1.7 and 4.6 hours, respectively.9 It is recommended that
the polymer, requirement for an adjunctive laxative, and
NaP not be used in patients with impaired renal function
the presence of artificial sweeteners. Commercially
(creatinine clearance <60 mL/min), congestive heart
available PEG lavage solutions include the traditional 4-
failure, or hypercalcemia. In addition, caution is advised
L preparations (GoLYTELY [Braintree], Colyte [Schwarz
when using NaP in individuals with pre-existing dehy-
Pharma], NuLYTELY [Braintree], TriLyte [Schwarz
dration, electrolyte disturbances, or an inability to con-
Pharma]), and low-volume 2-L regimens (HalfLytely
sume an appropriate quantity of fluids. Patients using
[Braintree], MiraLAX [Schering-Plough]) that require
NaP preparations should be carefully instructed to
the addition of bisacodyl or magnesium citrate. The rec-
maintain adequate fluid intake throughout the bowel
ommended dosing of most PEG solutions is 240 mL (8
cleansing process and to not exceed the recommended
oz) every 10 minutes. A “split-dose” regimen—in which
part of the laxative is taken the evening before, and the
A tablet formulation of NaP, designed to improve
remainder is taken the morning of the procedure—has
patient tolerability, was approved by the FDA in 2000.
been demonstrated to be more effective and better tol-
Visicol (Salix), the initial formulation, was recommended
erated than a single dose taken the evening before the
at a dose of 48 to 60 g, or 28 to 40 tablets split between
procedure (see below). It is estimated that 5% to 38% of
2 doses. Due to the presence of insoluble microcrys-
patients are unable to complete the 4-L PEG prepara-
talline cellulose—an insoluble excipient within the NaP
tion because of volume-related symptoms of abdominal
tablet that obscured visualization of colonic mucosa, in
fullness, nausea, or vomiting.4 Low-volume PEG prepa-
some instances—a residue-free NaP tablet was devel-
rations were developed in an effort to improve patient
oped. OsmoPrep (Salix) is smaller and has a smooth
waxy surface that improves its ease of swallowing. The
The low-volume PEG products are generally associat-
recommended dosage is 32 tablets—20 tablets the
ed with less abdominal discomfort, nausea, and vomiting
evening before and 12 tablets 3 to 5 hours prior to exam-
than the 4-L preparations, yet with equivalent efficacy.4-5
ination. Compared with Visicol, OsmoPrep induced less
At the current time, most low-volume PEG preparations
pronounced changes in electrolyte levels and fewer
require the addition of adjunctive stimulant laxative.
adverse events, including abdominal distention, nausea,
Patients ingest 4 bisacodyl delayed-release tablets (20
mg) at approximately 12 noon the day before the proce-
At least 16 studies have compared the efficacy and
dure, and start the lavage solution following evacuation
tolerability of PEG with NaP.4 Overall, these trials
or no more than 6 hours later. A low-volume PEG prepa-
demonstrated that NaP is more effective than either the
ration has recently been introduced that does not require
2-L or 4-L PEG-based preparations. In most of these
the addition of a laxative (MoviPrep, Salix). In addition to
studies, patient tolerance and compliance with bowel
PEG-3350 and sodium sulfate, it contains ascorbic acid
preparations was also superior with NaP. These conclu-
which serves as an osmotic agent to enhance bowel
sions are supported by the findings of two meta-analy-
cleansing. A multicenter, randomized, single-blind study
ses and an evidence-based position statement prepared
found MoviPrep to be as effective as 4 L PEG.6 In anoth-
by the Canadian Association of Gastroenterology.2-4
er comparative study, MoviPrep and an oral NaP-based
The use of NaP is often associated with abnormalities
preparation produced comparable results in overall colon
in serum electrolytes, including hypernatremia,
hypokalemia, hypocalcemia, and hyperphosphatemia.
Overall, the safety record with PEG-based prepara-
Although these alterations are usually transient and clin-
tions has been excellent. During the 6-year period end-
ically asymptomatic, the FDA received 34 reports of
ing in 2002, the FDA received 100 reports of adverse
adverse events between 1997 and 2002, including 18
events with PEG solutions, including 30 serious and 6
serious events and 8 fatalities related to the use of NaP
fatal events.4 Complications of PEG preparations include
preparations.4 A recent study reported 21 cases of acute
hypothermia, hyponatremia, intestinal perforation, aspi-
phosphate nephropathy, all occurring in patients that
ration, and Mallory-Weiss tear.8 The use of PEG-based
had recently taken a NaP bowel preparation.11 Seventeen
bowel cleansing is contraindicated in patients with
patients (81%) were female, the mean age among
I N D E P E N D E N T LY D E V E L O P E D B Y M C M A H O N P U B L I S H I N G
Table. Commonly Used Purgatives for Colonoscopy Preparation Recommended Usage* Sodium Phosphate
colonoscopy; 45 mL 10 to 12 h later (at least 3 h before the procedure)
colonoscopy; 30 mL 10 to 12 h later (at least 3 h before the procedure)
20 tablets (3 tablets every 15 min) at 5 to 6 pmthe evening before colonoscopy; repeat with 12 to 20 tablets 10 to 12 h later (at least 3 hbefore the procedure)
20 tablets (4 tablets every 15 min) at 5 to 6 pmthe evening before colonoscopy; repeat with 12 tablets 10 to 12 h later (at least 3 h before the procedure)
Polyethylene glycol 4-L PEG-ELS
240 mL (8 oz) every 10 min beginning at 5 to 6 pm the evening before colonoscopy(total, 3 L); remaining 1 L 10 to 12 h later (at least 3 h before the procedure)
4-L SF-PEG 2-L PEG-ELS and bisacodyl
4 bisacodyl delayed-release tablets at 12 noon
delayed-release tablets
the day before colonoscopy; 240 mL (8 oz)every 10 min beginning at 5 to 6 pm (total, 1 L);repeat 240 mL (8 oz) every 10 min beginning 3 to 4 h before the procedure (total, 1 L)
2-L PEG and bisacodyl delayed-release tablets 2-L PEG with ascorbate
240 mL (8 oz) every 15 min beginning at 5 to 6 pm the evening before colonoscopy(total, 1 L), followed by at least 16 oz fluid; 240mL (8 oz) every 15 min at least 3 to 4 h beforethe procedure (total, 1 L), followed by 16 oz fluid
Magnesium citrate
magnesium citrate (pre-measured quantity) at 5 to 6 pm the evening before colonoscopy; 4 bisacodyl delayed-release tablets at 7 to 8 pm (2 h after magnesium citrate); bisacodyl suppository 2 to 3 h before the procedure
ELS, electrolyte lavage solution; h, hours; L, liters; min, minutes; mL, milliliters; oz, ounces; PEG, polyethylene glycol; SF, sulfate-free
* In some cases, these recommendations do not correspond with the FDA-approved dosage.
I N D E P E N D E N T LY D E V E L O P E D B Y M C M A H O N P U B L I S H I N G
patients was 64 years, 16 of the 21 (76%) had a history
eliminating the need to discuss with the patient more
of hypertension, and 14 (67%) were taking an
than one regimen of bowel cleansing. Among the disad-
angiotensin-converting enzyme inhibitor or angiotensin
vantages, however, is an inability to adjust for differ-
receptor blocker. Although the exact incidence of this
ences between patients. For example, individuals vary in
complication cannot accurately be quantified, the risk
their tolerance and reaction to purgatives.14 The same
appears to be quite low considering the relatively small
cathartic may be well tolerated by one patient but pro-
number of cases reported and the extraordinarily large
duce nausea, vomiting, and abdominal cramps in anoth-
number of exposures to NaP (estimated to be in excess
er. Some patients prefer NaP pills whereas others favor
of 5,000,000 per year).12 On the basis of its overall safe-
the solution. Individuals with chronic constipation may
ty and efficacy, NaP is an appropriate option for bowel
require a more rigorous bowel cleansing regimen for
preparation in healthy individuals not possessing one of
adequate bowel cleansing. Differences such as these are
best accommodated by offering several bowel prepara-tions, so that each patient can be matched with the
preparation that is most likely to be effective, safe, and
Magnesium citrate is a hyperosmotic saline laxative
that increases intraluminal fluid volume, and, via stimu-
When endoscopy is performed in an open access set-
lation of cholecystokinin release, enhances gut motility.
ting, it is necessary to prescreen patients before select-
It is administered as a split dose, 300 mL (10 oz) the
ing a purgative regimen. In our practice, a receptionist
evening before colonoscopy and 3 to 5 hours prior to
or medical assistant completes a brief medical question-
the procedure. Since magnesium is eliminated by the
naire for each patient at the time of scheduling.
kidneys, it should not be used in patients with renal dis-
Information obtained that pertains to the choice of
purgative regimen includes: 1) a list of current medica-
A prepackaged low-fiber diet (NutraPrep [E-Z-EM])
tions and drug/food allergies; 2) a history of heart fail-
has recently been introduced, containing three low-
ure, kidney disease, ascites, or fluid/electrolyte abnor-
residue meals and snacks. The product is intended for
malities; and 3) a history of chronic constipation or
use in combination with a bowel cleansing system that
incomplete colonoscopy. Based upon the responses, a
contains a low-sodium magnesium citrate, bisacodyl-
bowel cleansing regimen (NaP versus PEG) is then sug-
delayed release tablets, and a bisacodyl suppository
gested. If oral NaP is chosen, patients are given the
(10 mg; LoSo Prep [E-Z-EM]). Patients are instructed
option of solution or pill formulation. When using a PEG-
to take magnesium citrate and 4 bisacodyl tablets (20
based regimen, the 2-L PEG preparation is chosen,
mg) the evening before colonoscopy plus a bisacodyl
except for use in patients with chronic constipation (see
suppository on the morning of the procedure. A ran-
below). In this way, the method of bowel cleansing for
domized, investigator-blinded study reported superior
colonoscopy is selected individually in order to maxi-
bowel cleansing and patient tolerability with this regi-
mize safety, efficacy, and patient satisfaction.
Clinical Considerations
Many endoscopy centers utilize a patient education
An effective preparation for colonoscopy is one that
program when preparing patients for gastrointestinal
consistently produces high quality bowel cleansing that
endoscopy. The topics to be covered include a descrip-
is adequate for the detection of all adenomatous polyps.
tion of the procedure, possible adverse effects and com-
It must also be safe, and ideally, work quickly, without
plications, and preparation instruction. The impact of
producing gastrointestinal distress. None of the prod-
bowel preparation on the success of colonoscopy, and
ucts currently marketed for colonoscopy preparation
the importance of compliance with instructions should
meet all of these criteria. Although most are effective
be emphasized. This message may be communicated
when properly administered, they require 12 to 24 hours
through one-on-one sessions, group meetings, or self-
for adequate bowel cleansing, and a significant propor-
instruction using either a videotape or computer-based
tion of patients experience disturbing gastrointestinal
program. Communicating this information effectively to
side effects. Consequently, the choice of a purgative
the patient helps to alleviate fear and anxiety related to
regimen(s) and methods of administration vary consid-
the procedure. In a prospective study, an education pro-
erably among endoscopists. This section examines
gram reduced the rate of failed preparations among
strategies of colon cleansing and provides suggestions
ambulatory patients from 26% to 5%.15 A role for educa-
for improving the quality and safety of bowel prepara-
tional intervention in hospitalized patients has not yet
tion. Recommendations for colonoscopy preparation
within special patient populations is also presented.
BOWEL PREPARATION: ONE SIZE DOES NOT FIT ALL
Colon cleansing produces significant volume loss
Some endoscopists prefer to offer all patients a sin-
through the gastrointestinal tract that can result in
gle method of bowel preparation. The benefits of such
intravascular volume depletion. The fluid loss during
an approach include simplicity and an economy of time,
bowel preparation may exceed 2 to 3 L, based upon an
I N D E P E N D E N T LY D E V E L O P E D B Y M C M A H O N P U B L I S H I N G
assessment of hemodynamic parameters and indirectmeasures such as body weight, serum osmolality andhematocrit.17
between NaP and PEG formulations have been reportedin some studies.18-21 Decreases in systolic blood pressure(> 10 mm Hg from baseline) and/or postural tachycardia(> 10 beats/minute from baseline) have been described
in 10% to 35% of patients who completed a bowelcleansing regimen.18 In addition, the use of NaP prepara-
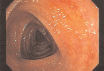
Figure 1. Images of the cecum during
tions is often associated with changes in serum elec-trolytes, including transient increases in phosphate and
colonoscopy demonstrate incomplete
sodium, and reductions in calcium and potassium. These
versus complete bowel cleansing.
changes generally remain within the normal range and
Image A demonstrates the cecum partially obscured by a thinlayer of ileal fluid and chyme. In contrast, the cecum in image B
are clinically asymptomatic. Serious electrolyte distur-
is optimally prepared for careful inspection of the mucosa.
bances, however, have been reported with both NaP22and PEG.23 Inadequate hydration is widely believed toplay an important role in such complications. Therefore,adequate hydration during bowel preparation should beemphasized, particularly in high-risk individuals, such asthe elderly, users of diuretics or other medications thatalter electrolyte levels, and patients with preexistingelectrolyte abnormalities. Patients should be advised toconsume at least 64 oz (approximately 2 L) of clear fluid
on the day prior to colonoscopy. The use of a carbohy-drate-electrolyte solution (e.g. Gatorade) has been
Figure 2. Typical images obtained
reported to improve patient hydration status, patient
during colonoscopy with successful
tolerance for the preparation, and the quality of bowel
bowel cleansing.
preparation.24 Patients should also be reminded to con-
Image A shows multiple, punctate red spots with central clear-
tinue hydration after colonoscopy; we advise that
ing—a diagnostic artifact of bowel preparation. These changes
patients consume at least 32 oz (4, 8-oz glasses) during
are readily distinguishable from active colitis (B), which is char-
the 8 hours following completion of the procedure.25
acterized by a diffuse inflammatory process.
The quality of colon preparation—especially in the
ascending colon—is closely related to the time between
including 1 of the doses taken the morning of the proce-
completion of the preparation and the examination.20,26
dure (8 pm and 6 am).29 Patients who received part of
Despite diet restriction for 24 hours, optimal cleansing
their preparation on the same day had better scores for
of the colon requires that at least part of the preparation
quality of cleansing than those who underwent prepara-
be ingested within 6 to 8 hours of the examination.
tion on the previous day (global rating good/excellent,
When more than 8 hours has elapsed, ileal contents
80% vs 68%, respectively). These and other studies pro-
begin to fill the colon, coating the wall of the ascending
vide convincing evidence that a split-dose regimen,
colon with a thin film of chyme that obscures mucosal
including 1 dose of laxative within 6 to 8 hours of exam-
ination, improves cleansing and imaging of the mucosa,
Split-dose regimens improve the efficacy of both NaP
especially within the right colon where flat polyps are
and PEG preparations. In a study using 3-L PEG plus
bisacodyl, a split-dose regimen (including 1 L on the day
For the purpose of studying the success of bowel
of procedure) gave a higher proportion of satisfactory
preparation, it is helpful to distinguish patients that are
preps (75% vs 66%) and better patient compliance with
scheduled for morning versus afternoon procedures.
lower rates of discontinuation.27 In another study, the
Patients undergoing a morning procedure should ingest
quality of bowel prep was compared using 2-L PEG
the first dose of cathartic between 4 and 6 pm and the
preparation administered either the day of (6 to 8 h
remainder between 3 and 5 am (depending on the time
before) or the evening before (13 to 16 h before) the pro-
of the procedure and the laxative selected). Patients
cedure.28 Colon preparation was better (93% vs 72%)
scheduled for afternoon procedures take their first dose
and more lesions were detected (2.8 vs 1.9) in the group
at 6 to 7 pm and the second dose at 6 to 7 am. Some
who received same-day bowel cleansing compared with
endoscopy units have modified their endoscopy sched-
the group who received cleansing the evening before
ule, booking all colonoscopies beginning at 12 noon. This
examination, respectively. A randomized trial compared
affords patients the convenience of taking the second
2 dosing regimens of NaP, 1 consisting of 2, 45-mL doses
dose of laxative at 6 to 7 am, rather than waking at 3 to
taken the evening before (3 pm and 8 pm) and the other
5 am. However, a recent study comparing the outcomes
I N D E P E N D E N T LY D E V E L O P E D B Y M C M A H O N P U B L I S H I N G
of morning versus afternoon colonoscopies reported
studies. A randomized controlled trial in octogenarians
significantly higher rates of incomplete procedures and
compared NaP with a 4-L PEG preparation.35 The quali-
lower rates of adequate bowel preparations in the after-
ty of preparation was similar in both groups, with a
noon.30 In our experience, many patients prefer to
good or excellent rating in 77% to 81% of patients
undergo colonoscopy in the morning, and most do not
receiving NaP or PEG. As anticipated, PEG produced
object to waking during the night to complete the
less change than NaP in the clinical parameters of dehy-
dration and laboratory tests. Fewer patients were
In Japan, the concept of split dosing has been taken
unable to complete the NaP preparation compared with
one step further with colon cleansing performed entire-
the PEG preparation, although the difference did not
ly on the morning of examination.31 Little or no diet
reach statistical significance. Overall, patients preferred
modification is required the day prior to colonoscopy.
NaP to PEG and were more willing to repeat this prepa-
Patients are instructed to begin the preparation around
ration again in the future. A second study, comparing
6 am with 2-3 L PEG. The preparation is considered
NaP with PEG in elderly patients reported that the over-
complete, usually within 3 hours, when the rectal efflu-
all quality of colon cleansing was comparable for both
ent is clear. Anecdotally, this preparation is reported to
preparations.36 Furthermore, patients who received
produce excellent cleansing. It remains to be established
NaP tolerated their preparation better than those who
whether a similar method of preparation would be
received PEG, although the difference was not statisti-
effective and tolerated by Western patients.
In some instances, the timing of bowel preparation
Patients With Inflammatory Bowel Disease. In gener-
may need to be altered in order to accommodate the
al, patients with inflammatory bowel disease can pre-
fasting requirements related to procedural sedation.
pare for colonoscopy using any of the standard bowel
There are no universally accepted guidelines on prepro-
purgatives. One exception is the patient with moderate
cedural fasting, and consequently, the literature contains
to severe diarrhea (more than 6 to 8 bowel movements
a variety of recommendations on this subject.
per day); for this patient, the dose of cathartic may be
Guidelines published by the American Society of
reduced or eliminated altogether. NaP preparations can
Anesthesiology state that patients should fast for a min-
produce aphthoid lesions in the colon, most prominent-
imum of 2 hours for clear liquids and 6 hours for light
ly within the rectum and sigmoid. This endoscopic
meal prior to sedation.32 On the other hand, an evi-
appearance is distinct and can be readily distinguished
dence-based review by American College of
from the endoscopic appearances of Crohn’s and ulcer-
Emergency Physicians33 states that “recent food intake
is not a contraindication for administering procedural
Pediatric Patients. In older children (12 years and
sedation and analgesia, but should be considered in
older), oral NaP solution at a dosage of 45 mL x 2 is
choosing the timing and target level of sedation.” A
probably the most widely used preparation.5 When used
recent position statement from the American
for younger children (6 to 11 years), the dose is often
reduced to 30 mL x 2. NaP is not recommended for chil-
“there is inadequate evidence to permit the develop-
dren ages 5 years and younger. A second method of
ment of absolute requirements for preprocedural fast-
preparation for children is a PEG-based formulation
ing, and the clinician should be guided by the practice
(MiraLAX) administered at a dose of 1.25-1.5 g/kg daily
parameters provided by various professional societies.”
for 4 days. In some instances, a laxative, such as
At the current time, until definitive evidence-based
bisacodyl, may be added to the regimen 1 day prior to
guidance is available, it is reasonable to recommend that
colonoscopy. The least commonly used preparation
patients undergoing colonoscopy with sedation remain
consists of either saline or phosphate enemas in combi-
fasting for a minimum of 2 hours before the procedure.
This requirement does not necessitate a change in the
In the pediatric population, there are inadequate data
use of a split-dose regimen for bowel preparation.
assessing efficacy and safety to recommend 1 regimenover another. The PEG-based preparations are generally
effective, but are often accompanied by abdominal
Elderly Patients. Persons 65 years and older comprise
bloating and vomiting.37 A modified PEG preparation
at least 20% of the patient population undergoing rou-
that is administered over 4 days appears to be better
tine colonoscopy. Older individuals are more likely to
tolerated, but has the potential for disrupting a child’s
have an incomplete preparation.1,35 The reasons for this
ability to attend school and participate in other activi-
are multifactorial and include an increased likelihood for
ties.38 Generally, oral NaP is better tolerated by children
constipation, reduced mobility, and difficulty complet-
than PEG, although hyperphosphatemia is often
ing the preparation. Elderly patients using NaP are also
observed. Practice recommendations for bowel prepa-
more likely to manifest hyperphosphatemia as a result
ration in children undergoing colonoscopy vary. A
of impaired renal function, co-morbid illness, and con-
recent consensus statement prepared by a joint task
force within the United States5 concluded that NaP, PEG,
The efficacy, safety, and tolerability of various purga-
and phosphate enema/senna preparations were all “safe
tives in older individuals have been evaluated in several
and will adequately prepare the child’s colon for
I N D E P E N D E N T LY D E V E L O P E D B Y M C M A H O N P U B L I S H I N G
colonoscopy.” The authors caution, however, that “incertain circumstances, such as bowel preparation in chil-
Box. Key Points
dren, … it may be advisable to adhere to PEG-basedsolutions because of the risks for occult physiologic dis-
1. The choice of bowel cleansing regimen for
turbances that may potentially contraindicate the use of
colonoscopy should be based upon the patient’s
NaP-based regimens.” For example, the FDA-approved
age, health status, comorbid diseases, and personal preference.
package insert of one manufacturer of NaP (CB Fleet),cautions against the use of oral NaP “in children under
2. A split dose bowel cleansing regimen that
includes 1 dose of laxative within 6 to 8 hours of
the age of 18 years.” Regardless of the regimen selected,
the examination improves the quality of bowel
it is important to provide children with adequate hydra-
cleansing, especially within the ascending colon.
tion during the process of bowel preparation. A carbo-
hydrate-electrolyte solution designed specifically for
demonstrated superior efficacy and tolerability to
children is often helpful for this purpose.
polyethylene glycol (PEG)-based preparations for
Patients With Lower Gastrointestinal Bleeding. In
colonoscopy preparation. NaP is an acceptable
most circumstances, patients undergoing colonoscopy
purgative for bowel cleansing in suitable patients;
for hematochezia must be prepared quickly.39 Colon
however, its use should be avoided in patients
transit is hastened by the presence of blood, and in most
with impaired renal function, congestive heart failure, advanced liver disease, and hypercalcemia.
cases, bowel cleansing can be completed within 2 to 3hours using 0.5 to 2 L of PEG solution. Patients who are
4. All purgatives have been associated with
serious adverse events. The risk for complications
unresponsive or mechanically ventilated may receive
the PEG solution through a nasogastric tube.
appropriate bowel cleansing regimen for each
Patients With a History of Inadequate Preparation or
patient and highlighting the importance of
Chronic Constipation. There are no studies to provide
adherence to preparation instructions.
the clinician with guidance for preparation of the patient
5. The importance of adequate hydration during and
with chronic constipation or a history of inadequate
after bowel preparation should be emphasized for
bowel cleansing during a previous colonoscopy.
Measures that have been recommended include: 1)extending the period of diet modification from 24 hoursto 48 hours; 2) adding oral bisacodyl or senna to a PEGor NaP regimen; and 3) increasing the total volume of
colonoscopy: efficacy, tolerability and safety - A CanadianAssociation of Gastroenterology position paper. Can J
PEG from 4 L to 6 L, with administration split over 48
hours (usually 1 to 2 L on day 1, and 3 to 4 L on day 2).
5. Wexner SD, Beck DE, Baron TH, et al. A consensus document on
In addition, adequate hydration will help to improve the
bowel preparation before colonoscopy: prepared by a task force
from The American Society of Colon and Rectal Surgeons(ASCRS), the American Society for Gastrointestinal Endoscopy(ASGE), and the Society of American Gastrointestinal and
Conclusion
Endoscopic Surgeons (SAGES). Gastrointest Endosc.
A substantial number of colonoscopies are subopti-
6. Ell C, Gruss H-J. Results of a randomised, multi-centre, single-blind
mal because of inadequate bowel preparation. This
trial to compare the efficacy, acceptability and safety of a new 2-
figure ranges from 17% to 30% in randomized trials and
litre gut cleansing solution versus a standard 4-litre PEG+E solu-
is probably higher in clinical practice. Several patient
tion. Gastrointest Endosc. 2004;59:AB125[Abstract S1555].
characteristics have been associated with poor bowel
Bitoun A, Ponchon T, Barthet M, Coffin B, Dugue C, Halphen M. Results of a prospective randomised multicentre controlled trial
preparation, including history of constipation, inpa-
comparing a new 2-L ascorbic acid plus polyethylene glycol and
tient status, use of antidepressants, and noncompli-
electrolyte solution vs. sodium phosphate solution in patients
ance with bowel preparation instructions.40,41 An
undergoing elective colonoscopy. Aliment Pharmacol Ther. 2006;24:1631-1642.
awareness of these factors, combined with strategies
8. Clark LE, DiPalma JA. Safety issues regarding colonic cleansing
designed to optimize the results of purgative regimens
for diagnostic and surgical procedures. Drug Saf.
and an emphasis on patient education and compli-
ance, will maximize the efficiency of colonoscopy and
9. Linden TB, Waye JD. Sodium phosphate preparation for
colonoscopy: onset and duration of bowel activity. Gastrointest
10. Rex DK, Schwartz H, Goldstein M, et al. Safety and colon-cleansing
References
efficacy of a new residue-free formulation of sodium phosphate
Froehlich F, Wietlisbach V, Gonvers JJ, Burnand B, Vader JP.
tablets. Am J Gastroenterol. 2006;101:2594-2604.
Impact of colonic cleansing on quality and diagnostic yield of
11. Markowitz GS, Stokes MB, Radhakrishnan J, D’Agati VD. Acute
colonoscopy: the European panel of appropriateness of gastroin-
phosphate nephropathy following oral sodium phosphate bowel
testinal endoscopy European multicenter study. Gastrointest
purgative: an underrecognized cause of chronic renal failure. J Am
2. Tan JJ, Tjandra JJ. Which is the optimal bowel preparation for
12. Rex DK, Balaban DH, Bond JH, et al. Oral sodium phosphate solu-
colonoscopy - a meta-analysis. Colorectal Dis. 2006; 8:247-258.
tion for bowel preparation: literature review and recommendations
3. Belsey J, Epstein O, Heresbach D. Oral bowel preparation for
of an industry-sponsored advisory panel regarding safe and effec-
colonoscopy. Aliment Pharmacol Ther. 2007;25:373-384.
4. Barkun A, Chiba N, Enns R, et al. Commonly used preparations for
www.phosphosoda.com/professionals/pdf/OSPS_document.pdf.
I N D E P E N D E N T LY D E V E L O P E D B Y M C M A H O N P U B L I S H I N G
13. DeLegge M, Kaplan R. Efficacy of bowel preparation with the use
28. Chiu HM, Lin JT, Wang HP, Lee YC, Wu MS. The impact of colon
of a prepackaged, low fibre diet with a low sodium, magnesium
preparation timing on colonoscopic detection of colorectal neo-
citrate cathartic vs. a clear liquid diet with a standard sodium
plasms - a prospective endoscopist-blinded randomized trial. Am
phosphate cathartic. Aliment Pharmacol Ther. 2005;21:1491-1495.
J Gastroenterol. 2006;101:2719-2725.
14. Keeffe EB. Colonoscopy preps: what’s best? Gastrointest Endosc.
29. Parra-Blanco A, Nicolas-Perez D, Gimeno-Garcia A, et al. The tim-
ing of bowel preparation before colonoscopy determines the qual-
15. Abuksis G, Mor M, Segal N, et al. A patient education program is
ity of cleansing, and is a significant factor contributing to the
cost-effective for preventing failure of endoscopic procedures in a
detection of flat lesions: a randomized study. World J
gastroenterology department. Am J Gastroenterol.
30. Sanaka MR, Shah N, Mullen KD, Ferguson DR, Thomas C, McCullough
16. Chorev N, Chadad B, Segal N, et al. Preparation for colonoscopy in
AJ. Afternoon colonoscopies have higher failure rates than morning
hospitalized patients. Dig Dis Sci. 2007;52:835-839.
colonoscopies. Am J Gastroenterol. 2006;101:2726-2730.
17. Holte K, Nielsen KG, Madsen JL, Kehlet H. Physiologic effects of
31. Chiu HM, Lin JT, Wang HP, Lee YC, Wu MS. Response to Parra-
bowel preparation. Dis Colon Rectum. 2004;47:1397-1402.
Blanco et al. (author reply) Am J Gastroenterol. 2007;102:908-909.
18. Vanner SJ, MacDonald PH, Paterson WG, Prentice RS, Da Costa
32. Practice guidelines for preoperative fasting and the use of phar-
LR, Beck IT. A randomized prospective trial comparing oral sodi-
macologic agents to reduce the risk of pulmonary aspiration:
um phosphate with standard polyethylene glycol-based lavage
application to healthy patients undergoing elective procedures: a
solution (GoLYTELY) in the preparation of patients for
report by the American Society of Anesthesiologist Task Force on
colonoscopy. Am J Gastroenterol. 1990;85:422-427.
Preoperative Fasting. Anesthesiology. 1999;90:896-905.
19. Cohen SM, Wexner SD, Binderow SR, et al. Prospective, random-
33. Godwin SA, Caro DA, Wolf SJ, et al. Clinical policy: procedural
ized, endoscopic-blinded trial comparing precolonoscopy bowel
sedation and analgesia in the emergency department. Ann Emerg
cleansing methods. Dis Colon Rectum. 1994;37:689-696.
20. Mathus-Vliegen EM, Kemble UM. A prospective randomized blind-
34. Cohen LB, Delegge MH, Aisenberg J, et al. AGA Institute review
ed comparison of sodium phosphate and polyethylene glycol-
on endoscopic sedation. Gastroenterology. 2007;133:675-701.
electrolyte solution for safe bowel cleansing. Aliment PharmacolTher. 2006;23:543-552.
35. Seinela L, Pehkonen E, Laasanen T, Ahvenainen J. Bowel prepara-
tion for colonoscopy in very old patients: a randomized prospec-
21. Hwang KL, Chen WT, Hsiao KH, et al. Prospective randomized
tive trial comparing oral sodium phosphate and polyethylene gly-
comparison of oral sodium phosphate and polyethylene glycol
col electrolyte lavage solution. Scand J Gastroenterol.
lavage for colonoscopy preparation. World J Gastroenterol.
22. Fine A, Patterson J. Severe hyperphosphatemia following phos-
36. Thomson A, Naidoo P, Crotty B. Bowel preparation for
phate administration for bowel preparation in patients with renal
colonoscopy: a randomized prospective trial comparing sodium
failure: two cases and a review of the literature. Am J Kidney Dis.
phosphate and polyethylene glycol in a predominately elderly
population. J Gastroenterol Hepatol. 1996;11:103-107.
23. Nagler J, Poppers D, Turetz M. Severe hyponatremia and seizure
37. da Silva MM, Briars GL, Patrick MK, Cleghorn GJ, Shepherd RW.
following a polyethylene glycol-based bowel preparation for
Colonoscopy preparation in children: safety, efficacy, and toler-
colonoscopy. J Clin Gastroenterol. 2006;40:558-559.
ance of high- versus low-volume cleansing methods. J PediatrGastroenterol Nutr. 1997; 24:33-37.
24. Barclay RL, Depew WT, Vanner SJ. Carbohydrate-electrolyte rehy-
dration protects against intravascular volume contraction during
38. Pashankar DS, Uc A, Bishop WP. Polyethylene glycol 3350 without
colonic cleansing with orally administered sodium phosphate.
electrolytes: a new safe, effective, and palatable bowel prepara-
Gastrointest Endosc. 2002;56:633-638.
tion for colonoscopy in children. J Pediatr. 2004;144:358-362.
25. Lichtenstein GR, Cohen LB, Uribarri J. Bowel preparation for
39. Green BT, Rockey DC, Portwood G, et al. Urgent colonoscopy for
colonoscopy: importance of adequate hydration. Aliment
evaluation and management of acute lower gastrointestinal hem-
orrhage: a randomized controlled trial. Am J Gastroenterol. 2005;100:2395-2402.
26. Church JM. Effectiveness of polyethylene glycol antegrade gut
lavage bowel preparation for colonoscopy - timing is the key! Dis
40. Ness RM, Manam R, Hoen H, Chalasani N. Predictors of inadequate
bowel preparation for colonoscopy. Am J Gastroenterol. 2001;96:1797-1802.
27. El Sayed AM, Kanafani ZA, Mourad FH, et al. A randomized single-
blind trial of whole vs. split-dose polyethylene glycol-electrolyte
41. Harewood GC, Sharma VK, de Garmo P. Impact of colonoscopy
solution for colonoscopy preparation. Gastrointest Endosc. 2003;
preparation quality on detection of suspected colonic neoplasia.
AUTHOR DISCLOSURES—Dr. Cohen has served on the advisory board and speakers’ bureau of Salix Pharmaceuticals. Dr. Tennyson has
DISCLAIMER—This review is designed to be a summary of information, and represents the opinions of the author. Although detailed,
the review is not exhaustive. Readers are strongly urged to consult any relevant primary literature, the complete prescribing informa-
tion available in the package insert of each drug, and the appropriate clinical protocols. No liability will be assumed for the use of this
review, and the absence of typographical errors is not guaranteed. Copyright 2007, McMahon Publishing, 545 West 45th Street, 8th
Floor, New York, NY 10036. Printed in the USA. All rights reserved, including right of reproduction, in whole or in part, in any form.
I N D E P E N D E N T LY D E V E L O P E D B Y M C M A H O N P U B L I S H I N G
PRINTER-FRIENDLY VERSION AT GASTROENDONEWS.COM •
Patient Guide to PREPARING FOR COLONOSCOPY
reparing for colonoscopy involves cleaning your bowel completely so that your physician
has a clear view during the exam. This process is very important because if everything
Phas not been removed from your intestines, the procedure could take longer, there is a
greater risk for complications, the physician may not be able to finish the colonoscopy prop-
erly, and you might have to do it all over again sooner than normal. To ensure that your
colonoscopy is completed properly, follow all your doctor’s instructions. Helpful Tips
There are different methods to clean out your colon, and your doctor will tailor one for you
that he or she has found works. To make sure you and your doctor choose the right method
for you, tell your doctor of your current medications, any drug or food allergies, and if you
have ever had heart problems, kidney disease, ascites, fluid or electrolyte abnormalities,
chronic constipation, or an incomplete colonoscopy. Remember to follow your doctor’s
instructions exactly so your procedure is completed as smoothly as possible.
Why do I have to drink so much fluid for the colonoscopy?
You may be given liquid electrolytes or something similar to drink before your colonoscopy.
It will be a lot to drink and it may not taste very good; but, it is important to drink the entire
preparation to thoroughly clean your colon, avoiding any problems during the procedure
and making sure you do not have to do it again any time soon.
Why do I have to eat and drink differently?
Your doctor may give you a list of low-fiber foods to eat for one to three days before your
colonoscopy. Make sure to stick to eating foods on this list as much as possible. Your doctor
will also ask you not to eat anything after a certain time before your test and to drink plenty
of clear, nonalcoholic fluids. Doing so will make cleaning your colon more complete,
as well as keep you hydrated and safe from any problems with the preparation for the
colonoscopy and the colonoscopy itself. RESOURCES www.mayoclinic.com/health/colonoscopy/CO00009
Centers for Disease Control and Prevention
www.cdc.gov/cancer/colorectal/basic_info/screening www.gastro.org/wmspage.cfm?parm1=861
TRIGEMINAL NEURALGIA ASSOCIATION TEXAS SUPPORT GROUPS NEWSLETTER JULY 2006 SAN ANTONIO SUPPORT GROUP MEETING – DATE CHANGE The San Antonio Support Group will meet next on August 1 not August 8 as originally planned. Jonathan White, M.D. with UT Southwestern in Dallas will be the guest speaker. For more details, please check the meeting flyer. FORT WORTH
Prédica del 29 de diciembre de 2006 en la Iglesia de la Adoración en el Monte Schoenstatt Queridos hermanos en el sacerdocio, queridos amigos de la Familia de Schoenstatt: El 29 de diciembre de hace 32 años consagré mi vida como sacerdote a la Madre Tres Veces Admirable y comenzó así mi camino sacerdotal en la Familia de Schoenstatt. En este día vengo hasta aquí e
 PRINTER-FRIENDLY VERSION AT GASTROENDONEWS.COM •
PRINTER-FRIENDLY VERSION AT GASTROENDONEWS.COM •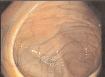

 assessment of hemodynamic parameters and indirectmeasures such as body weight, serum osmolality andhematocrit.17
between NaP and PEG formulations have been reportedin some studies.18-21 Decreases in systolic blood pressure(> 10 mm Hg from baseline) and/or postural tachycardia(> 10 beats/minute from baseline) have been described
in 10% to 35% of patients who completed a bowelcleansing regimen.18 In addition, the use of NaP prepara-
Figure 1. Images of the cecum during
assessment of hemodynamic parameters and indirectmeasures such as body weight, serum osmolality andhematocrit.17
between NaP and PEG formulations have been reportedin some studies.18-21 Decreases in systolic blood pressure(> 10 mm Hg from baseline) and/or postural tachycardia(> 10 beats/minute from baseline) have been described
in 10% to 35% of patients who completed a bowelcleansing regimen.18 In addition, the use of NaP prepara-
Figure 1. Images of the cecum during PRINTER-FRIENDLY VERSION AT GASTROENDONEWS.COM •
PRINTER-FRIENDLY VERSION AT GASTROENDONEWS.COM •