Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Hhd.fullerton.edu
Evaluation of Dynamic Balance Among Community-Dwelling Older Adult Fallers: A Generalizability Study of the Limits of Stability Test Sean Clark, PhD, Debra J. Rose, PhD
ABSTRACT. Clark S, Rose DJ. Evaluation of dynamic
difficulties and are often at increased risk for falls when per-
balance among community-dwelling older adult fallers: a gen-
forming ADLs that require dynamic postural control. Decre-
eralizability study of the Limits of Stability Test. Arch Phys
ments in dynamic postural control have been attributed to both
age and pathology-associated changes in spatial and temporal
Objective: To establish reliability estimates of the 75%
parameters associated with movements of the COG within the
Limits of Stability® Test (75% LOS test) when administered to
stability region. Compared with younger adults, healthy older
community-dwelling older adults with a history of falls.
adults exhibit smaller voluntary COG excursions, reach max-
Design: Generalizability theory was used to estimate both
imal lean more slowly, and exhibit less postural control once
the relative contribution of identified error sources to the total
they have reached maximum lean.2,3 Dynamic postural control
measurement error and generalizability coefficients. A random
is even further compromised as a result of underlying pathol-
effects repeated-measures analysis of variance (ANOVA) was
ogy and/or physical deconditioning in older adult populations.4
used to assess consistency of LOS test movement variables
The ability to quantify reliably age- and/or pathology-associ-
ated declines in dynamic postural control has implications for
Setting: A motor control research laboratory in a university
both the early identification of individuals at risk for falls and
for the evaluation of treatment interventions. Participants: Fifty community-dwelling older adults with 2
Recent advances in computerized forceplate technology
have provided researchers and clinicians a way to quantify
Main Outcome Measures: Spatial and temporal measures
objectively an individual’s performance during various dy-
of dynamic balance derived from the 75% LOS test included
namic balance tasks. One dynamic balance assessment test
average movement velocity, maximum center of gravity
increasingly reported in the clinical and research literature is
(COG) excursion, end-point COG excursion, and directional
the Limits of Stability® Test (LOS test). The LOS test provides
spatial and temporal measures (eg, movement velocity, maxi-
Results: Estimated generalizability coefficients for 2 testing
mum excursion, directional control) of COG movements as a
days ranged from .58 to .87. Total variance in LOS test mea-
person volitionally leans to various positions in space. Previous
sures attributable to inconsistencies in day-to-day test perfor-
investigators5-7 have used these temporal and spatial measures
mance (Day and Subject ϫ Day facets) ranged from 2.5% to
from the LOS test to elucidate dynamic balance capabilities in
8.4%. The ANOVA results indicated that no significant differ-
both healthy and patient populations. Although sophisticated
ences were observed in the LOS test variables across the 2
measures of dynamic postural control can be derived from
performance on the LOS test, the clinical value of these move-
Conclusions: The 75% LOS test administered to older adult
ment-related variables depends on their reliability.8
fallers on 2 consecutive days provides consistent and reliable
The reliability of the LOS test has been studied both in
young populations and in healthy older adult populations.7,9-11
Key Words: Accidental falls; Balance; Elderly; Rehabilita-
However, previous investigators,9-11 with the exception of
Clark et al,7 based their reliability estimates on performance
2001 by the American Congress of Rehabilitation Medi-
variables that are no longer available on current versions of the
cine and the American Academy of Physical Medicine and
LOS test software.a Potential problems associated with the
calculations of the original LOS test movement variables (ie,movement time, path sway, target sway, distance error) may
THE ABILITY TO CONTROL intentional movements of have produced biases in previous reliability estimates of the
the center of gravity (COG) when leaning or performing
LOS test. For example, earlier test versions required that sub-
weight-shifting activities is critical to the successful perfor-
jects actually reach each of the 8 test targets to receive a
mance of various functional tasks associated with activities of
performance score. Failure to reach the target resulted in a
daily living (ADLs).1 Many older adults, however, experience
default score of 8 seconds in the case of the movement timevariable, and subsequently an inaccurate estimate of the per-formance variables. The current LOS test movement variablesno longer require that subjects actually reach the target, pro-
From the Department of Movement Science, Gordon College, Wenham, MA
viding a more accurate assessment of dynamic postural con-
(Clark); and Center for Successful Aging, California State University, Fullerton,
Although the study by Clark7 indicates that the LOS test,
Accepted in revised form May 30, 2000.
performed at either 75% or 100% of maximum limits of sta-
No commercial party having a direct financial interest in the results of the research
supporting this article has or will confer a benefit upon the author(s) or upon any
bility, is reliable when administered to healthy older adults on
organization with which the author(s) is/are associated.
2 separate occasions, clinical measurements and the treatment
Reprint requests to Sean Clark, PhD, Dept of Movement Science, Gordon College,
of balance-related disorders are almost exclusively performed
255 Grapevine Rd, Wenham, MA 01984, e-mail: sclark@faith.gordon.edu.
with patient populations or with individuals at risk for falls.
0003-9993/01/8204-5839$35.00/0doi:10.1053/apmr.2001.21859
Differences in movement strategies between older adults with
Arch Phys Med Rehabil Vol 82, April 2001 GENERALIZABILITY OF DYNAMIC BALANCE, Clark
and without a history of falls during dynamic postural tasksmay have implications for the consistency and/or stability (ie,reliability) of dynamic balance measures. Consequently, inves-tigators must be cautious when generalizing reliability esti-mates of the LOS test from older adults with no prior history offalls to those who have experienced repeated falls.
The present study sought to estimate the reliability of the
LOS test when administered to older adults experiencing dis-turbances in balance and gait. The 75% LOS test was selectedbecause it is likely to more than adequately challenge thepostural control system in a group of older adults experiencingdisorders of balance and gait. Subjects
Fifty older adults (35 women, 15 men; age range, 62–90yr;
mean age Ϯ standard deviation, 77.5 Ϯ 6.6yr) volunteered toparticipate in the present study. These subjects were a subgroup
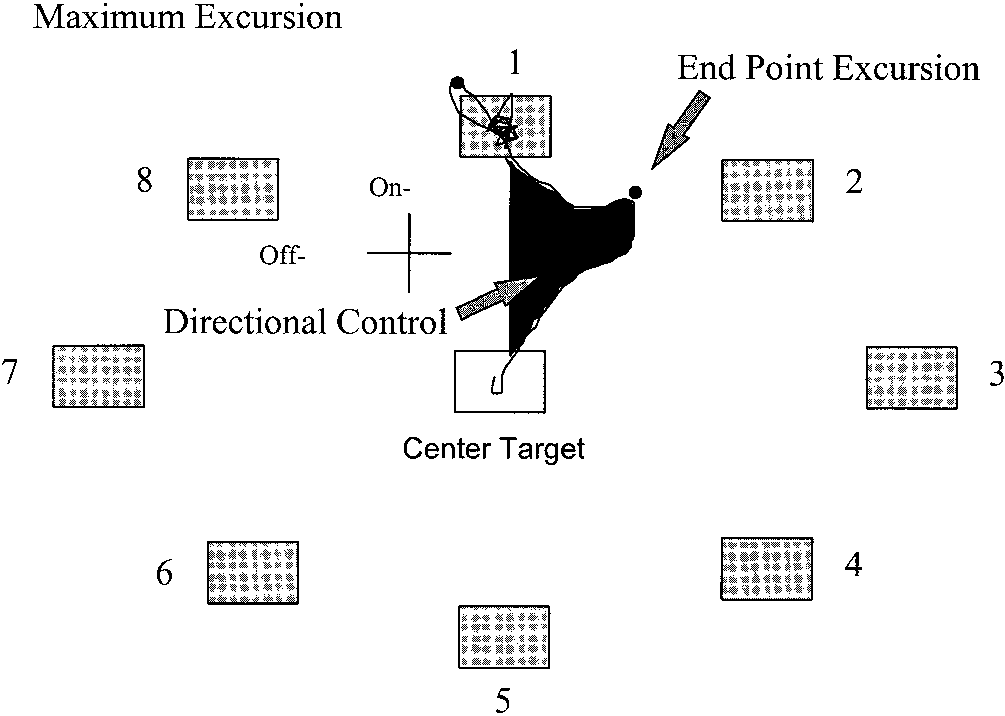
Fig 1. Target set-up and dynamic balance measures for the LOS
selected from a larger sample of community-dwelling older
adults (n ϭ 75) recruited to participate in a balance interventionprogram. Participants for the intervention program were solic-ited through newspaper advertisements and presentations tophysician groups within the community. Once enrolled in the
individual being tested. The video screen provided an on-
balance intervention program, individuals completed a com-
screen visual display of the test set-up as well as concurrent
prehensive background and medical history questionnaire. The
visual biofeedback of the subject’s COG position. The on-
primary investigators reviewed the questionnaires and 50 older
screen test set-up (fig 1) consisted of 8 visual targets (ie, small
adults were identified as meeting the specific selection criteria
squares) displayed in a circular fashion positioned at 75% of
for the present study. These inclusion criteria included: having
the subject’s theoretic limits of stability. The appropriate 75%
had 2 or more falls within the previous year; living indepen-
LOS test target locations for each subject were derived by
dently in the community (ie, noninstitutionalized setting); hav-
using the PRO Balance Master software.12 Calculations of the
ing no known medical diagnosis that might account for balance
limits of stability target locations were based on the subject’s
difficulties (eg, Parkinson’s disease, stroke, multiple sclerosis);
predicted COG height (ie, derived from standing height) and
having no known cognitive impairments; not currently taking
previously determined maximum COG sway angles.12
any medications known to adversely affect balance or to com-
Before testing, subjects were informed that the on-screen
pensate for balance-related problems (eg, Antivert [meclizine
COG cursor (ie, visual biofeedback) moved in response to the
hydrochloride], certain classes of psychotropic drugs); and
movements of their body COG. They were then encouraged to
normal or corrected vision (eg, glasses, contact lens). Addi-
produce movements of the cursor by leaning the body away
tionally, participants had to be able to ambulate without an
from the midline. This 3- to 5-minute familiarization period
assistive device and to maintain an upright stance indepen-
provided subjects with an opportunity to explore movements of
dently for a minimum of 2 minutes. Before participating in the
the on-screen COG cursor to promote an understanding of the
investigation, each participant signed an informed consent doc-
relationship between movements of the cursor and the actual
ument approved by the university’s institutional review board.
Testing procedures as described in the PRO Balance Master
Instrumentation
operators manual were initiated by having subjects position theCOG cursor in the center target.12 Subjects were subsequently
Spatial and temporal measures of dynamic postural control
instructed to move the COG cursor as quickly and directly as
were obtained from each subject’s LOS test performance on the
possible in the direction of the highlighted target as soon as the
PRO Balance Master® system,a version 6.11. The PRO Bal-
start signal appeared on the screen.12 The start signal was in the
ance Master system has 4 symmetrically positioned force trans-
form of a small blue circle that moved from the center target to
ducers that measure vertical pressures applied by a standing
the highlighted test target. Once subjects moved the position of
person to the support surface. These vertical pressure data were
the COG cursor either within the test target or as close to it as
used to derive anteroposterior and mediolateral coordinates of
possible (ie, reached maximal lean), they were instructed to
the center of pressure, which were subsequently used to cal-
hold their position as still as possible until the blue circle and
culate the spatial and temporal characteristics of the projected
start signal disappeared from the screen. The subject then
COG movements. The forceplate system was also interfaced
repositioned the COG cursor in the center target and waited for
with a model 486 PC computer to acquire and store test data.
the start signal for the next highlighted target. The standardLOS test protocol required participants to lean out toward each
Procedures
of the 8 targets in a sequential clockwise direction.
A standard 75% LOS test was administered on the PRO
During the test, subjects were required to stand with their
Balance Master on 2 consecutive days. During each testing
arms by their sides and to maintain their feet in the standard-
session, subjects were assisted onto the force platform and
ized foot position. A reference grid superimposed on the force
asked to maintain an upright stance with their arms resting by
plate allowed for careful monitoring of the feet during the
their sides and their feet in a standardized foot position as
testing procedures. If the subject lost balance while leaning (eg,
recommended by the equipment manufacturer.12 A video
took a step) or shifted foot position during testing, his/her feet
screen was positioned at eye level, directly in front of the
were repositioned and the trial was repeated. Also, as a pro-
Arch Phys Med Rehabil Vol 82, April 2001 GENERALIZABILITY OF DYNAMIC BALANCE, Clark
tective measure against potential falls, subjects wore a properly
of days) from which balance measures could have been ob-
fitted safety harness during all testing procedures.
tained. Similarly, the 8 test targets were identified as a randomrepresentative sample of all possible target or spatial positions
Dependent Variables
located at 75% of the subject’s theoretic limits of stability.
After identification of each of the facets in the measurement
The following spatial and temporal measures of dynamic
design, a fully crossed 50 ϫ 2 ϫ 8 (Subjects ϫ Day ϫ Targets)
balance were derived for each of the 8 test targets comprising
the LOS test: average movement velocity (MV), directional
(ANOVA) was performed. This analysis technique provided
control (DC), end point excursion (EE), and maximum excur-
calculated mean square values for each source of measurement
sion (ME). MV, expressed in degrees per second, quantified the
variation in the design (ie, each facet and their interactions).
speed at which a subject was able to displace the COG (ie,
Variance components for the object of measurement (ie, sub-
lean) during the first sustained movement excursion toward the
jects), Day (D), Target (T), Subject by Day (S ϫ D), Subject by
test target. The degree to which the COG was controlled during
Target (S ϫ T), Day by Target (D ϫ T), and the Subject by
the first sustained movement excursion was expressed as DC.
Day by Target interaction combined with the residual random
The DC value was derived from the amount of on-axis move-
error (S ϫ D ϫ T-E) were then estimated based on the
ment of the COG relative to off-axis COG movement and was
expected mean squares and calculated mean squares for each
expressed as a percentage of the total on-axis movement. EE
source of variance. When negative variance components were
and ME provided measures of the distance each participant was
obtained, a 0 value was substituted for the negative value and
able to lean through his/her theoretic limits of stability. EE
the 0 value was used for any further calculations involving
indicated the on-axis distance the COG was displaced from the
center target during the first sustained movement excursion
After identification of the various facets and calculations of
toward the test target. The ME data quantified the maximal
the variance components, a G study was performed. In the G
distance that COG was displaced from the center target in the
study, the relative contribution of each variance component to
on-axis direction of the test target. Both EE and ME were
the total measurement error was determined.14,16,19 These esti-
expressed as a percentage of the test target distance (ie, 75%
mates of the percentage of variance attributed to subjects, D, T,
limits of stability). Each limits of stability variable provided
S ϫ D, S ϫ T, D ϫ T, and S ϫ D ϫ T-E indicated which
specific information regarding the subject’s ability to control
measurement condition(s) were contributing to the variability
intentional movements of his/her COG to the 8 predetermined
positions in space (ie, to the 8 on-screen visual targets). See
Decision study.
figure 1 for a graphic illustration of DC, ME, and EE.
tion of the G study. The D study enables the investigator todetermine the optimal measurement design. Specifically, the D
Data Analysis
study yields generalizability coefficients (G coefficients) that
Reliability estimates across the 2 test days and 8 test targets
reflect the reliability or generalizability of the measures for a
were determined for each of the 75% LOS test movement
specified measurement design.15-17 The calculated G coefficient
variables. Analyses of both measurement consistency and gen-
serves as a reliability index and can be interpreted as a reli-
eralizability were conducted by using a fully crossed 50 ϫ 2 ϫ
ability coefficient across the universe(s) of the various facets
8 (Subjects ϫ Day ϫ Target) random effects repeated-mea-
included in the study.14-17 In the present investigation, G coef-
sures design. The GENOVA computer program, version 2.2,
ficients were calculated across the universe of days and targets
where the Day facet was varied across the 2 days and the
Generalizability analysis.
Target facet was generalized across the 8 targets.
sessments, a patient’s test score may be viewed as a sample
Measurement consistency.
score from the universe (ie, infinite distribution) of possible
ally recognize that some variability in test scores occurs when
scores under the specific measurement protocol used.14-17 Con-
conducting repeated evaluations, the magnitude of the ob-
sequently, a test score may be influenced by multiple sources of
served differences in these scores should not be statistically or
measurement error. Differences between the observed score
clinically significant.17,21,22 Because a reliable measurement
and the expected or universe score (ie, true score) may be
system, by definition, provides consistent test scores that are
attributed to measurement errors associated with the specific
free from error across multiple evaluations, investigators inter-
conditions or “facets”—ie, raters, days, trials— under which
ested in establishing reliability estimates must evaluate the
the testing was performed.14,16,18 Generalizability analysis en-
consistency of test results obtained from repeated assessments.
ables the researcher to identify and estimate the relative con-
In the present study, measurement consistency (ie, differences
tribution of various sources of measurement error within a
in mean scores) of the 4 LOS test movement variables across
single model (ie, generalizability study [G study]); and to
the 2 days of testing and the 8 targets was assessed by per-
determine the optimal measurement schedule for controlling
forming tests of statistical significance for the calculated quasi
measurement error and for increasing reliability (ie, decision
F ratios based on the mean squares from the random effects
study [D study]).14-18 A more detailed review of generalizabil-
ANOVA output.23 To prevent the inflation of type I error, the
alpha level of significance was adjusted to p Ͻ .01. Tukey’s
Generalizability study.
post hoc comparisons of means were conducted when signifi-
quired the identification of each source of error or “facet” that
cant differences were observed in either the Day and/or Target
may have contributed to the variability in the subjects’ scores.
main effects. Post hoc comparisons were also conducted at an
Each facet was then identified as either a random or fixed
adjusted alpha level of p Ͻ .01.
measurement effect. In the present investigation, days and
Absolute reliability.
targets were identified as random facets. That is, these facets
solute reliability of the measures, the standard error of the
were identified as being a random representative sample of all
measurement (SEM) was calculated for each LOS test move-
possible observations of that facet.18,19 The 2 testing days in the
ment variable. Each SEM was derived as the positive square
present measurement design were considered to be representa-
root of the absolute error variance for each of the respective
tive of a random selection of all possible test days (ie, universe
LOS test movement variables.14,18,19 The calculated SEM val-
Arch Phys Med Rehabil Vol 82, April 2001 GENERALIZABILITY OF DYNAMIC BALANCE, Clark Table 1: Mean Values for Days Collapsed Across 8 Targets Table 3: Variance Components and Percentage of Variation for ME
NOTE. Data presented as means Ϯ standard deviation.
ues reflect the amount of error that can be expected in the
target 5 were also significantly larger than the DC values for
Measurement Consistency
Table 1 contains mean values and standard deviations for
each LOS test performance variable for the 2 days of testingcollapsed across the 8 test targets. Nonsignificant F ratios for
G study results, including the estimated variance compo-
the Day main effect in each ANOVA result indicated that LOS
nents and the percentages of variation for each facet, are
test performance as measured by each of its 4 movement
presented in tables 2–5. As indicated in these tables, the total
variables was consistent across the 2 days of testing. In contrast
variation in LOS test performance attributed to the Day facet
to the findings for the Day effect, variability in LOS test
was less than 1% for each of the LOS test movement variables
performance across the 8 test targets was determined to be
examined. These findings indicate that the contributions of the
statistically significant for all 4 LOS test movement variables
Day variance to the total measurement error for each LOS test
examined. The ANOVA results for the Target main effect
variable were negligible. Moreover, a summation of the Day
indicated significant differences in MV (F
facet with both the S ϫ D and D ϫ T interactions yielded
percentage variance values that ranged from only 2.55% to
8.39% across the 4 LOS test variables. Collectively, the G
Follow-up Tukey post hoc comparisons were conducted
study findings indicate that the total variance in LOS test
independently for each LOS test movement variable to identify
performance associated with administering the 75% LOS test
which target differences contributed to the significant Target
on 2 separate days was minimal (Ͻ9%).
main effect. Post hoc analysis for MV indicated that the COG
In comparison to variance estimates for the Day facet, vari-
excursions toward the forward and rear targets (targets 1 and 5,
ability in LOS test performance attributed to differences across
respectively) were significantly slower than the COG excur-
the 8 test targets accounted for a larger proportion of the total
sions toward all other targets. Results from post hoc compar-
measurement error in each LOS test movement variable (tables
isons for EE indicated that initial COG excursions within the
2–5). Approximately 5% (ME) to 14% (DC) of the total vari-
75% theoretic limits of stability were also significantly smaller
ation in the LOS test measures was attributable to the Target
for targets 1 and 5 when compared with both the lateral targets
facet. Additionally, the S ϫ T interaction yielded estimated
(targets 3, 7) and the forward diagonal targets (targets 2, 8).
variance values that ranged from approximately 8% (MV) to
Additionally, EE values for the rear diagonal targets (targets 4,
16% (ME). The larger variance estimates associated with the
6) were significantly smaller than values for the right forward
S ϫ T interaction indicated that subjects varied in their abilities
target (target 2). Post hoc analyses further revealed that ME
to control COG movements to the different test targets.
values were significantly larger for target 2 than for all other
The largest proportion of measurement variability in each of
test targets, except the right lateral target (target 3). Also, ME
the LOS test movement variables was attributed to the residual
values for target 3 were significantly larger than ME values for
error variance (S ϫ D ϫ T-E). The S ϫ D ϫ T-E interaction
the rear target (target 5). Finally, post hoc comparisons for DC
contributed between 39.91% (ME) and 53.26% (MV) to the
indicated that COG movement control when leaning toward
total variation in the dependent variables examined (see tables
targets 4 and 6 was poorer (ie, significantly larger) than that
2–5). These results indicated that a large percentage of the
observed for all other targets, except for target 5. DC values for
variability in the LOS test was associated with (1) the highestorder interaction term (ie, S ϫ D ϫ T), (2) sources of mea-
Table 2: Variance Components and Percentage of Variation for MV Table 4: Variance Components and Percentage of Variation for EE Arch Phys Med Rehabil Vol 82, April 2001 GENERALIZABILITY OF DYNAMIC BALANCE, Clark Table 5: Variance Components and Percentage of
small samples or samples that fail to represent the population
Variation for DC
adequately may be a concern in generalizability analyses be-cause they may include potential inaccuracies or instabilities in
the variance estimates.26 Although formulas for sample size
estimates are not readily found in the generalizability theory
literature, previous investigators25,27,28 have reported that sam-
ples of 30 to 50 participants are appropriate when using intra-
class correlation analyses to establish test reliability. Given that
generalizability theory is an extension of the intraclass reliabil-
ity model, the inclusion of 50 subjects in the present study is
consistent with both suggested intraclass correlation sample
size estimates and sample sizes previously reported in G stud-ies.7,19
surement error or facets not identified in the present investiga-
Generalizability Analysis
tion, or (3) random measurement error.
Similar to the work of Clark et al,7 reliability in the present
investigation was estimated by using generalizability analysis.
Unlike reliability estimates from classical test theory, general-
D Study results for each of the 4 LOS test movement
izability analysis provides researchers and clinicians with es-
variables are presented in table 6. As indicated in this table, a
timates of both the magnitude and the relative contribution of
single administration of the 75% LOS test (ie, 8 targets)
identified sources of measurement error.14,15,18 This informa-
yielded estimated G coefficients ranging from .44 (DC) to .80
tion helps investigators determine a measurement protocol that
(ME), whereas, G coefficients derived for the present measure-
provides optimal, adequate, and/or cost-effective reliability
ment protocol (8 targets, 2 test days) ranged from .58 (DC) to
.87 (ME). The calculated G coefficient for DC indicated a
Day facet.
Generalizability analysis in the present investi-
moderate reliability estimate24; whereas the G coefficients for
gation provided estimates of the total variance in LOS test
the MV, ME, and EE measures yielded high reliability esti-
movement scores attributable to differences or inconsistencies
mates when generalized across the complete LOS test and 2
in day-to-day test performance. Estimates of the Day variance
are valuable for researchers and clinicians because variation inday-to-day performance contributes to measurement error and
Standard Error of Measurement
consequently may have negative implications on the reliability
Calculations of the SEM values for each of the 4 LOS test
of measures. Variance estimates derived for the Day facet in
movement variables were based on the estimated variance
the present investigation indicated, however, that when the
components derived from the G study implementing the full
75% LOS test is administered to older adult fallers, little
measurement protocol (8 test targets, 2 days of testing). The
variation is evident in performance scores across days. Our
calculated mean score for each of the 2 test days and the
findings ranged from 2.5% to 8.4%. Clark7 reported similar
respective SEM values for each movement variable are pre-
findings. The investigators reported that the Day facet was a
sented in table 1. Comparison of the SEM values with the
relatively small source of measurement error (2%–12%) when
calculated mean scores for test days indicated that the SEM
administering the 75% LOS test to a sample of healthy com-
values were relatively small for each of the reported LOS test
munity-dwelling older adults. Additionally, findings from both
investigations indicate that the LOS test movement variablesare reliable across repeated evaluations. The implications for
DISCUSSION
practitioners are that, though variation in scores during re-
The present investigation was prompted by the need to
peated evaluations of the 75% LOS test is expected, the extent
establish reliability estimates of the 75% LOS test when con-
of differences in movement variables is statistically and pre-
ducted with independent community-dwelling older adults with
a history of falls. Although the reliability of this test has
Target and Subject by Target facets.
previously been established when conducted with healthy com-
mates attributed to the subjects by targets interaction indicated
munity-dwelling older adults,6 no attempt has been made to
that subjects differed in their LOS test performance scores as a
determine the reliability of the 75% LOS test when conducted
function of the 8 LOS test targets. These differences or incon-
with older adults who experience disorders of balance and gait.
sistencies in the subjects’ performance may be attributed to the
Results of the present analyses indicate that the spatial and
inability of some subjects to move the COG to various posi-
temporal measures of COG movement for the LOS test con-
tions in space located at 75% of their theoretical limits of
ducted at 75% of the subject’s theoretic limits of stability
stability. Age-related declines in the voluntary excursions of
provide consistent and reliable measures of dynamic balance
the COG to various regions within the limits of stability have
when performed by independent community-dwelling older
been previously identified.2,3 Consequently, the 8 target posi-
adults with a history of falls. The reported G coefficients for the
tions of the 75% LOS test derived from the subject’s theoretic
4 LOS test movement variables when generalized across 2 daysof testing and 8 limits of stability targets ranged from moderateto high. Additionally, results of the ANOVA indicated that the
Table 6: Coefficients for Days and 8 Targets
measures of dynamic balance derived from the LOS test wereconsistent across the 2 test days.
Caution is often advised when interpreting or generalizing
reliability estimates because issues may exist regarding both
the size and homogeneity of the subject sample.25 The use of
Arch Phys Med Rehabil Vol 82, April 2001 GENERALIZABILITY OF DYNAMIC BALANCE, Clark
maximum stability limits may have exceeded the actual limits
sessment scores do not overlap (ϮSEM) with scores obtained
of stability of some older adult subjects.
during the preintervention evaluations.
Variability in the LOS test measures associated with the
Target facet and the Subject by Target interaction may also be
Clinical Implications
attributed to differences in the selection of postural strategies
The present investigation provides clinicians with estimates
for producing displacements of the COG. Although subjects in
of the relative contribution of several error sources associated
the present study were encouraged to produce movements of
with LOS test performance. A clinician’s knowledge of these
the COG cursor by leaning or rotating about the ankle joints
relative variance contributions affords the opportunity to mod-
(ie, use an ankle strategy), some subjects may have explored
ify a measurement protocol to minimize measurement error and
the effectiveness of different postural strategies for producing
obtain acceptable levels of reliability when administering the
displacements of the COG cursor. For example, a subject may
75% LOS test to independent community-dwelling older adults
have adopted an ankle strategy to produce COG movements to
with a previous history of falls. For example, a clinician can
the mediolateral targets, but may have selected a hip strategy
conclude from the present findings that the residual error vari-
for COG excursions to the anteroposterior targets. Several
ance is a significant source of measurement error. It is possible,
possible explanations to account for the exploration of postural
therefore, to reduce this residual error variance by standardiz-
strategies during the LOS test could be forwarded, including:
ing both testing instructions and procedures and by providing
adopting a biomechanically “safer” strategy (ie, hip strategy)
sufficient practice time for patients to understand the relation-
for situations of perceived instability or fear of falling; com-
ship between their movements and the movement of the COG
pensating for self-perceived cognitive and physical demands
cursor. Also, by recognizing the relatively low variance esti-
associated with implementing only an ankle strategy; and/or
mates associated with the Day facet, a clinician may determine
limitations in movement strategies because of undiagnosed
that 3 days of testing is not more cost effective than 2 days,
according to generalizability estimates. Unexplained Variance CONCLUSIONS
In the present investigation, the unexplained variance com-
The 75% LOS test administered to older adult fallers on 2
ponent (S ϫ D ϫ T-E) accounted for the largest percentage of
consecutive days is a reliable test of dynamic balance. The G
variability in each of the LOS test movement variables. A
coefficients for the MV, ME, and EE measures indicated high
portion of this measurement variability may be attributable to
reliability estimates when generalizing across the 2 days of
random measurement error. Possible sources of random mea-
testing. Performance scores for the test’s 4 LOS test movement
surement error in the present investigation include inherent
variables were consistent across the 2 test days. A minimum of
electrical noise in the PRO Balance Master system, distur-
2 testing days (or 2 administrations of the test on the same day)
bances in the testing environment, subject’s motivation level,
is recommended to obtain reliable and consistent measures of
and misinterpretations of the COG visual biofeedback.
dynamic balance when administering the 75% LOS test to
Variability attributed to the S ϫ D ϫ T-E interaction may
independent community-dwelling older adults with a history of
also be attributable to sources of measurement error not iden-
tified in the present measurement design. That is, the presentdesign only calculated variance estimates for the object of
References
measurement (ie, subjects), the Day facet, the Target facet, and
1. Topp R, Mikesky A, Thompson K. Determinants of four func-
tional tasks among older adults: an exploratory regression analy-
the Subject, Day, and Target interaction effects. Additional
sis. J Orthop Sport Phys Ther 1998;27:144-53.
sources of measurement error in the present investigation may
2. Schieppati M, Hugon M, Grasso M, Nardone A, Galante M. The
have included the subject’s age and biomechanic factors (eg,
limits of equilibrium in young and elderly normal subjects and in
muscular strength, joint range of motion), which can limit
parkinsonians. Electroencephalogr Clin Neurophysiol 1994;93:
3. Blaszczyk JW, Lowe DL, Hanseb PD. Ranges of postural stability
Absolute Reliability
and their changes in the elderly. Gait Posture 1994;2:11-7.
4. Rose DJ, Dickin C. Postural instability and age-related changes in
Results from G study provide practitioners and researchers
dynamic limits of stability. J Sport Exerc Psychol 1999;21:S93.
with information regarding the relative variance contributions
5. Hamman RG, Mekjavic I, Longridge NS. Training effects during
attributed to each of the various sources of measurement error
repeated therapy sessions of balance training using visual feed-
included in the design. Although this information is valuable,
back. Arch Phys Med Rehabil 1992;73:738-44.
especially when optimizing a measurement protocol, absolute
6. Rose DJ, Clark S. Can the control of bodily orientation be signif-
differences in the measures are unknown. For the practitioner,
icantly improved in a group of older adults with a history offalling? J Am Geriatr Soc 2000;48:275-82.
the SEM or absolute differences in measures is an important
7. Clark S, Rose DJ, Fujimoto K. Generalizability of the limits of
and practical component of measurement reliability.17 That is,
stability test in the evaluation of dynamic balance among older
the practitioner is often concerned with how closely the ob-
adults. Arch Phys Med Rehabil 1997;78:1078-84.
tained score on a test reflects the true score for that test. The
8. Shephard NT, Telian SA, Smith-Wheelock M, Raj A. Vestibular
SEM value provides the expected range about the observed
and balance rehabilitation therapy. Ann Otol Rhinol Laryngol
score in which the true score lies. The calculated SEM values
reported in the present and previous investigations were rela-
9. Brouwer B, Culham EG, Liston RA, Grant T. Normal variability of
tively small compared with the mean scores. Thus, when ad-
postural measures: implications for the reliability of relative balance
ministering the 75% LOS test to older adult fallers and non-
performance outcomes. Scand J Rehabil Med 1998;30:131-7.
10. Henderson NE, Overby AS, Panzer VP. Internal consistency and
fallers, the practitioner can expect the true score to lie within a
stability of balance measures among different age groups [ab-
limited range of the observed score. Additionally, the small
stract]. In: Proceedings of the 12th International Congress of the
SEM values may also be beneficial when evaluating the effec-
World Federation for Physical Therapy; 1995 June 25-30; Wash-
tiveness of a balance intervention program. Specifically, a
ington (DC). Alexandria (VA): American Physical Therapy As-
criterion for an effective program is that postintervention as-
Arch Phys Med Rehabil Vol 82, April 2001 GENERALIZABILITY OF DYNAMIC BALANCE, Clark
11. Hageman PA, Leibowitz M, Blanke D. Age and gender effects on
21. Mitchell SK. Interobserver agreement, reliability and generaliz-
postural control measures. Arch Phys Med Rehabil 1995;76:961-5.
ability of data collected in observational studies. Psychol Bull
12. NeuroCom International Inc. Balance Masters operators manual.
Clackamas (OR): NeuroCom International; 1993.
22. Thomas JR, Nelson JK. Introduction to research in health, phys-
13. Crick JE, Brennan RL. GENOVA: a general purpose analysis of
ical education, recreation and dance. Champaign (IL): Human
variance system [computer program]. Dorchester (MA): Univ
Massachusetts at Boston, Computer Facilities; 1984.
23. Myers JL, Wells AD. Research design and statistical analysis.
14. Morrow JR Jr. Generalizability theory. In: Safrit MJ, Wood TM,
24. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing
editors. Measurement concepts in physical education and exercise
rater reliability. Psychol Bull 1979;86:240-8.
science. Champaign (IL): Human Kinetics; 1989. p 73-96.
25. Morrow JR Jr, Jackson AW. How significant is your reliability?
15. Shavelson RJ, Webb NM, Rowley GL. Generalizability theory.
26. Smith P. A confidence interval approach for variance component
16. Shavelson RJ, Webb NM. Generalizability theory: a primer. New-
estimates in the context of generalizability theory. Educ Psychol
17. Portney LG, Watkins MP. Foundations of clinical research: ap-
27. Donner A, Eliasziw M. Sample size requirements for reliability
plications to practice. Norwalk (CT): Appleton & Lange; 1993.
18. Brennan RL. Elements of generalizability theory. Iowa City (IA):
28. Baumgartner TA. Norm-referenced measurement: reliability. In:
American College Testing Program; 1983.
Safrit MJ, Wood TM, editors. Measurement concepts in physical
19. Roebroeck ME, Hariaar J, Lankhorst GJ. The application of
education and exercise science. Champaign (IL): Human Kinetics;
generalizability theory to reliability assessment: an illustration
using isometric force measurements. Phys Ther 1993;73:386-401.
20. Cardinet J, Tourneur Y, Allel L. Extension of generalizability
Supplier
theory and its applications in educational measurement. J Educ
a. NeuroCom International, Inc, 9570 SE Lawnfield Rd, Clackamas,
Arch Phys Med Rehabil Vol 82, April 2001
ELENCHI SOGGETTI INTERESSATI ALLE ATTIVITA' ESPROPRIATIVE PROVINCIA DI BERGAMO COMUNE DI CARAVAGGIO AGRICOLA LUIGI DEFENDI S.S. prop. per 1/1, BAVARO Angelo nato a MILANO il 07/11/1965 prop. per 1/4, FAVA Gianluca nato a CINISELLO BALSAMO il PART. 10760 12/09/1966 prop. per 1/4, ZIGLIOLI Maria Grazia Emilia PART. 11966 nata a CARAVAGGIO il 19/02/1967, prop. per 1/4
Ahmed RL, Prizment A, Lazovich D, Schmitz KH, Folsom AR (2008) Lymphoedema and quality of life in breast cancer survivors: the Iowa Women's Health Study. Journal of Clinical Oncology 26(35):5689-5696 Alentorn-Geli E, Padilla J, Moras G, Haro C, Fernandez-Sola J (2008) Six Weeks of Whole-Body Vibration Exercise Improves Pain and Fatigue in Women with Fibromyalgia. The Journal of Alternative and Com
 GENERALIZABILITY OF DYNAMIC BALANCE, Clark
GENERALIZABILITY OF DYNAMIC BALANCE, Clark