Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Ln121taub_topdf_mb
Treatment Of Rosacea With Intense Pulsed Light Photorejuvenation Amy Forman Taub, MD, and Erin DeVita, CST Northwestern Memorial Physicians Group Center for Advanced Dermatology and Laser Surgery Abstract: Rosacea is a disease that affects millions of men and women. Signs and symptoms include facial erythema, flushing episodes and acneiform eruptions. Conventional treatment consists of topical and oral antibiotics, although many people have sub-optimal control of their flushing and erythema with medical therapy. Although the etiology of rosacea is unknown, the end result is a diffuse network of small telengiectasias. It would seem reasonable to use a laser targeting vascular lesions to treat rosacea. There are few reports of the use of lasers to treat rosacea. We investigated the use of intense pulsed light therapy for reduction of the symptoms and signs of rosacea. 30 consecutive patients (skin types I-III) underwent 1-5 treatments with intense pulsed light and were assessed for degree of reduction in erythema, severity of flushing episodes and severity of acne breakouts. The Vasculight Plus intense pulsed light source was utilized at the following parameters: a double pulse of 2.4 and 4.0 ms and a 20 ms delay time at a fluence of 32-38 J (570 filter) or 27-32J (560 filter). Results were determined by clinical evaluation by the treating physician and patient evaluation via questionnaire. 87% of patients rated their redness as better or much better and 79% thought their flushing improved. 64% said their breakouts improved. Complications were minimal and transitory. These results suggest intense pulsed light is an effective adjunctive treatment for the signs and symptoms of rosacea. Longer-term followup will be needed to determine the degree of maintenance therapy necessary to maintain a remission state in this chronic disease. Key words: rosacea, intense pulsed light, facial erythema, acneiform eruptions, flushing. Introduction 1. Rosacea is a chronic disease that affects millions of men and women. 2. Signs and symptoms include erythema, flushing episodes with or without trigger
3. Etiologic theories include bacteriologic, inflammatory, neurologic, and vascular
4. Conventional treatment with oral and topical antibiotics is often only partially
5. Panfacial treatment with an intense pulsed light source targeting the vascular
telengiectasias of rosacea was investigated for minimizing the erythema, flushing discomfort, and acneiform lesions of rosacea.
Patient #1: Left profile, before treatment. Patient #1: Left profile, after treatment. Methods 1. 30 consecutive patients presenting for treatment of resistant rosacea were enrolled in
the study. 2 did not complete their follow-up visits, so the 28 remaining were evaluated. 1-5 treatments were performed on these patients all of whom had skin types I-III.
2. The Vasculight Plus Intense Pulsed Light device was utilized with refrigerated gel. 3. The parameters were: 560 (at 27-32J) or 570 (at 32-36J) filter with 2.4/4.0 ms.
4. Patients were evaluated by digital photography, clinical assessment, and
Results
1. The mean duration of disease for these patients was 7.25 years. The patients’ age
range was 33-65, the average being 44. There were 26 females and 2 males.
2. The two principal motives cited for pursuing treatment were redness and flushing.
Other reasons given were the desire to wear less makeup and the wish to discontinue oral medications.
3. The main flare factors reported by patients were (in descending order): intense
emotion, exercise, sun, wind, red wine, other alcoholic beverage, spicy foods, white wine, hot beverages.
4. The average number of treatments was 3.7 and average time to follow up was 3.6
Patient #2: left profile, before treatment. Patient #2: Left profile, after treatment.Results II 1. 33% of patients thought their redness much better, 54% better and 18% felt they were
2. 33% of these patients thought their flushing episodes were much better and 46%
deemed them better. 25% felt they were the same.
3. 39% said their breakouts were much better, 25% better, and 25% the same. 4. Complications were minimal (purpura in one, peeling in one and hypopigmentation in
Discussion Patients with rosacea often get to a plateau in their medical treatment where they have controlled their acne and reduced their redness by one to a few shades -- but they continue to have some degree of background redness, fixed telengiectasias, and flushing episodes. When presented with an option to improve upon this, most are eager to try a new treatment. It is imperative to explain to patients that this is not a cure for rosacea and that rosacea is a chronic disease that will require ongoing treatment. I have found that this disease profoundly alters my patients’ self-perception and that they are often frustrated by the lack of treatment options. Men also perceive the signs of rosacea as putting the stigma of associated alcoholism on themselves, and are relieved to be rid of the redness. Currently we are experimenting with a Zimmer Cryo-5, an air-cooling device that improves the tolerance of this procedure, decreases potential complications and may enable us to perform higher intensity treatments and reduce the number of treatments necessary to induce remission.
Also, we do utilize a 1064 Laser (Vasculight) occasionally with a 6 mm spot size at a setting of a single 16 ms pulse with 95-110 Joules for larger diameter (0.5-2mm) vessels around the nose, for more rapid resolution. Conclusions Intense Pulsed Light therapy is a safe and effective treatment for the signs and symptoms of rosacea. Longer-term follow-up and further studies will be ne cessary to elucidate the exact role of lasers in the treatment of rosacea, which is a chronic disease. We propose that laser therapy can play a primary role in the induction of remission in rosacea. Ideally, we would determine how to maximize its efficiency and minimize exacerbations. We are planning a longer-term, quantitative prospective study to further elucidate this. References 1. Jansen T, Plewig G. Rosacea: classification and treatment. JR Soc Med 1997
2. Webster GF. Treatment of Rosacea. Semin Cutan Med Surg 2001 Sep;20(3):207-8. 3. Angermeier MC. Treatment of facial vascular lesions with intense pulsed light. J
4. Laughlin SA, Dudley DK. Laser therapy in the management of rosacea. J Cutan
5. Dahl MV, Katz HI, Krueger GG, Millikan LE, Odom RB et al. Topical
metronidazole maintains remissions of rosacea. Arch Dermatol 1998 Jun;134(6):679-83.
Northern College for Body Psychotherapy Directors: Training Consultant: Bill Cornell MA TSTA Jamie McDowell BA MSTAT Steff Oates BA TSTA Fellside Centre, Low Fellside, Kendal, Cumbria LA9 4NH Psychophysical Therapy Training Course – to begin October 2011 Running over six two-day trainings the course will appeal to practitioners wanting to incorporate attention to psychophysical asp

 Introduction
Introduction  Methods
Methods  Patient #2: Left profile, after treatment.
Results II
Patient #2: Left profile, after treatment.
Results II 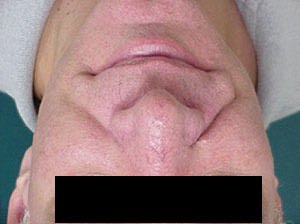
 Also, we do utilize a 1064 Laser (Vasculight) occasionally with a 6 mm spot size at a
Also, we do utilize a 1064 Laser (Vasculight) occasionally with a 6 mm spot size at a