Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Pii: s0022-5347(05)65769-2
Copyright 2001 by AMERICAN UROLOGICAL ASSOCIATION, INC.®
LONG-TERM USE OF TAMSULOSIN TO TREAT LOWER URINARY
TRACT SYMPTOMS/BENIGN PROSTATIC HYPERPLASIA
CLAUDE C. SCHULMAN, TYCHO M. T. W. LOCK, JEAN-MARIE BUZELIN, FRANK BOEMINGHAUS,
MEMBERS OF THE EUROPEAN TAMSULOSIN STUDY GROUP
From the Erasmus University Hospital, Brussels, Belgium, Academisch Ziekenhuis Utrecht, Utrecht, The Netherlands, Hoˆtel Dieu Nantes,Nantes, France, Urologische Klinik, Neuss, Germany, University Hospital of Wales, Cardiff, United Kingdom, and Pa¨lja¨t-Ha¨me Central
Purpose: The long-term efficacy and safety of 0.4 mg. tamsulosin once daily were assessed in
patients with lower urinary tract symptoms/benign prostatic hyperplasia treated for up to 4years.
Materials and Methods: A total of 516 patients were enrolled from 2 European open label
studies that were extensions of 3 double-blind controlled studies.
Results: Significant improvement in maximum urine flow and total Boyarsky symptom score
during the controlled trials was sustained throughout the extension study for up to 4 years inpatients who remained on therapy. The increase in mean maximum urine flow from baseline was1.2 to 2.2 ml. per second (p Ͻ0.001) and it remained 11.5 to 12 ml. per second during followup. Total Boyarsky symptom score was decreased from baseline by 4.1 to 4.7 points (p Ͻ0.001). Theincidence of treatment responders, defined as a 25% or greater decrease in total symptom score,remained stable throughout the 4-year period. Increasing the dose of tamsulosin from 0.4 to 0.8mg. seemed to have no substantial additional benefit. During the 4 years of treatment 26% ofpatients had side effects that were considered possibly or probably drug related. However, only5% of patients discontinued treatment because of drug related side effects. No clinically signif-icant changes in blood pressure or pulse rate occurred during the study.
Conclusions: Long-term treatment with tamsulosin is safe and well tolerated in patients with
lower urinary tract symptoms/benign prostatic hyperplasia. Improved efficacy was sustainedduring 4 years of followup.
KEY WORDS: prostate; prostatic hyperplasia; receptors, adrenergic, alpha-1; urination disorders
␣1-Adrenoceptor antagonists are recommended as the
study6 was an extension of 2 randomized, double-blind, pla-
main pharmacological treatment for patients with benign
cebo controlled phase III studies comparing 0.4 mg. tamsu-
prostatic hyperplasia (BPH) presenting with lower urinary
losin once daily with placebo.7, 8 The other open label study
tract symptoms.1 However, there is a relative paucity of
(unpublished data) was an extension of a randomized,
long-term data on the maintenance of efficacy of ␣1-
double-blind phase III study comparing 0.4 mg. tamsulosin
adrenoceptor antagonists. For doxazosin and terazosin long-
once daily with 2.5 mg. alfuzosin 3 times daily.9 Patients who
term efficacy and safety have been previously shown.2, 3 How-
elected to continue tamsulosin treatment after completion of
ever, results were based on an interim analysis and the
the controlled studies were recruited into the extension study
number of patients who were effectively treated for 3 and 4
as soon as possible after the controlled trials. The protocol of
the long-term extension studies indicated that open label
Several long-term studies with a duration of between 1 and
tamsulosin treatment should be continued for at least 1 year
3 years have already confirmed the good efficacy and safety
and maximally 4. This final analysis includes patients re-
profile of 0.4 mg. tamsulosin once daily.4–6 We present a finalpooled analysis of 2 European open label long-term tamsulo-
maining in the study for up to 4 years. The study started in
sin studies in which all patients had the option of continuing
May 1992 and the last patient completed the study in July
for up to 4 years. In addition, the efficacy and safety of 0.8 mg.
1997. Patients from 87 centers in 10 European countries
tamsulosin in cases of a less than optimal response to 0.4
mg. tamsulosin were evaluated. To our knowledge this
Inclusion and exclusion criteria. Patients who successfully
report provides the largest followup of the long-term effi-
completed the controlled studies and elected to participate in
cacy and safety of an ␣1-adrenoceptor antagonist in a large
a long-term open label tamsulosin study were enrolled in the
number of patients in which all patients had the option of
extension studies. All those who entered the open label ex-
tension studies had already fulfilled the inclusion criteria ofthe controlled trials, that is 4 to 12 ml. per second maximum
urine flow for a voided volume of 120 ml. or greater, diagnosis
This pooled analysis involved 2 European open label stud-
of benign prostatic enlargement, total Boyarsky symptom
ies of the efficacy and safety of 0.4 mg. tamsulosin once daily
score greater than 6 points, a complete set of evaluations
for lower urinary tract symptoms/BPH. The first open label
available at the clinic visit at the end of the controlled stud-ies, and urinalysis, biochemistry and hematology results
Accepted for publication May 25, 2001.
within the normal range. All patients provided gave informed
Supported by Yamanouchi Europe B. V.
LONG-TERM TAMSULOSIN USE FOR URINARY TRACT SYMPTOMS
consent for participation. All exclusion criteria have been
A total of 831 patients were randomized to the controlled
Study design and assessments. Patients were treated with
studies, of whom 768 (92%) completed the trials. Of these 768
open label 0.4 mg. tamsulosin as a modified release capsule
patients 516 (67%) elected participation in the long-term
once daily after breakfast. The dose of tamsulosin could be
extension studies. Table 1 lists patient demographics and
increased to 0.8 mg. from visit 3 (week 26) and thereafter in
baseline characteristics, which are in accordance with those
the long-term studies if efficacy was not considered optimal
normally reported in clinical trials of ␣1-adrenoceptor antag-
and no significant side effects probably or possibly related to
tamsulosin were reported. Patients were assessed at study en-
Table 2 shows the number of patients who withdrew from
rollment at visit 1, at 2 weeks at visit 2 and then at 12-week
the study before visits 6 (before 1 year), 10 (before 2 years), 14
intervals for the remainder of the study. At each 12-week visit
(before 3 years) and 18 (before 4 years). The most common
the patient completed the Boyarsky symptom score and free
reasons for withdrawal were insufficient therapeutic re-
flow studies were performed. At visits 6 at 48 weeks, 10 at 96
sponse, drug related and other side effects and other unspec-
weeks, 14 at 144 weeks and 18 at 192 weeks or the last visit
ified reasons. At most visits between 1% and 6% of patients
when a patient withdrew early from the trial physical exami-
withdrew from the study. However, at visit 6 the number of
nation and abdominal ultrasound were performed, the investi-
patients who withdrew was disproportionately large (77 or
gator noted the global efficacy of the medication on a scale of
15%). In the protocol this visit was defined as the point to
0 —worse to 3—much improved and the patient completed a
which all patients were treated with tamsulosin with the
option of continuing tamsulosin therapy thereafter if study
Efficacy assessments. The primary parameters for assess-
participation was still desired. After 4 years a third of the
ing efficacy were changes in maximum urine flow and total
patients remained in the study. Table 3 shows that the dis-
Boyarsky symptom score. Other efficacy parameters wereobstructive voiding, irritative filling, and individual symp-
continuation rate varied among geographic areas. It was
tom scores, quality of life questionnaire and investigator
lowest where tamsulosin had not been commercially avail-
global assessment of efficacy. In addition, the number of
able until July 1997, the date of the last visit in this series,
patients with a clinically significant response to tamsulosin
such as Belgium and some Nordic countries (Denmark, Nor-
was determined, defined as a 25% or greater decrease in total
Boyarsky symptom score. Furthermore, patients with a max-
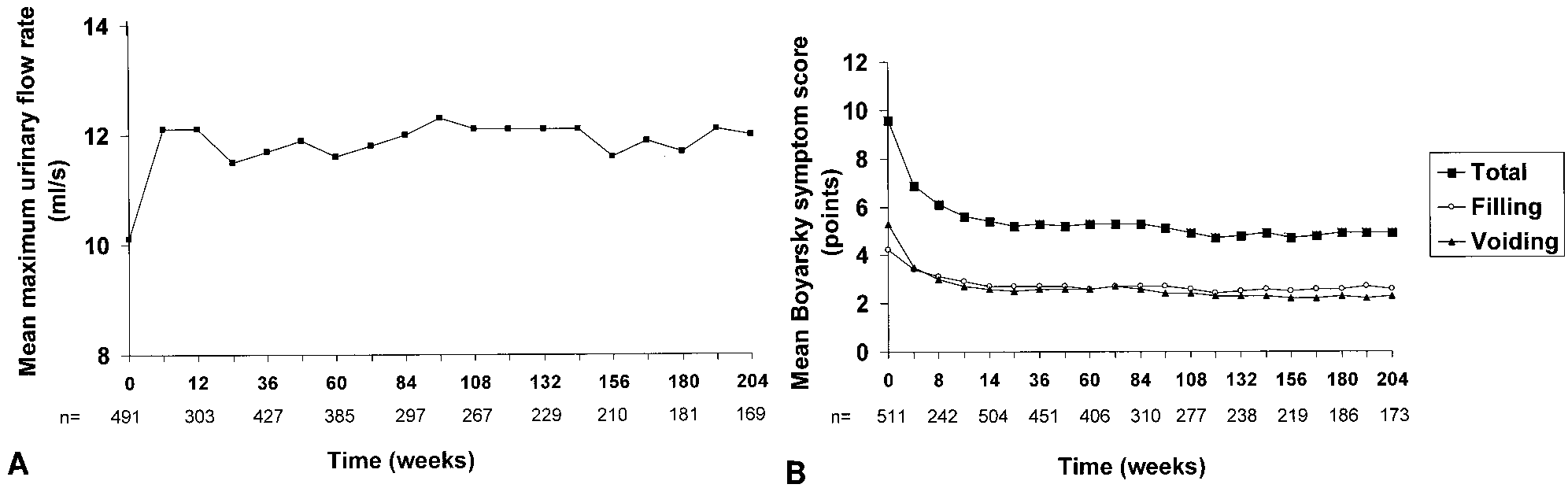
Changes in maximum urine flow and total symptom score.
imum urine flow response, defined as a 30% or greater, or 3
Figure 1, A shows mean maximum urine flow with time in
ml. per second or greater improvement over baseline, were
patients treated with tamsulosin for up to 204 weeks (4
years). At baseline mean maximum urine flow was 10.1 ml.
Efficacy was assessed on an intent-to-treat population, in-
per second. Already after 4 weeks at the initial assessment in
cluding all patients who received at least 1 dose of tamsulosin
the placebo controlled studies a maximum increase was
in the long-term extension study and who for whom followup
achieved that was sustained for up to 4 years of tamsulosin
efficacy data were available for at least 1 visit after extension
treatment. The increase in mean maximum urine flow from
study enrollment. The safety population included all patients
baseline was between 1.2 and 2.2 ml. per second (12% and
who received at least 1 dose of study medication in the
22%, p Ͻ0.001 versus baseline at each time point). Mean
long-term extension study. Safety assessments included
maximum urine flow remained predominantly between 11.5
monitoring all reported side effects as well as side effects
and 12 ml. per second throughout followup.
considered possibly or probably drug related by the investi-
Figure 1, B shows that the mean total Boyarsky symptom
gator plus vital signs and laboratory determinations. Within
score improved significantly compared with baseline from 6.9
group changes from baseline were assessed using the paired
to 9.6 points (p Ͻ0.001) after 4 weeks, which was the first
Student t test. All tests were 2-sided with significance con-
assessment in the controlled studies. This improvement
reached a maximum of 5.4 points after 14 weeks and wassustained for the remainder of tamsulosin treatment (p
Ͻ0.001 versus baseline at each time point). The mean de-crease in total symptom score from baseline ranged between
TABLE 1. Baseline characteristics of patients in the long-term study
4.1 and 4.7 points (43% and 49%) from 14 weeks of treatmentand thereafter. Irritative filling and obstructive voiding
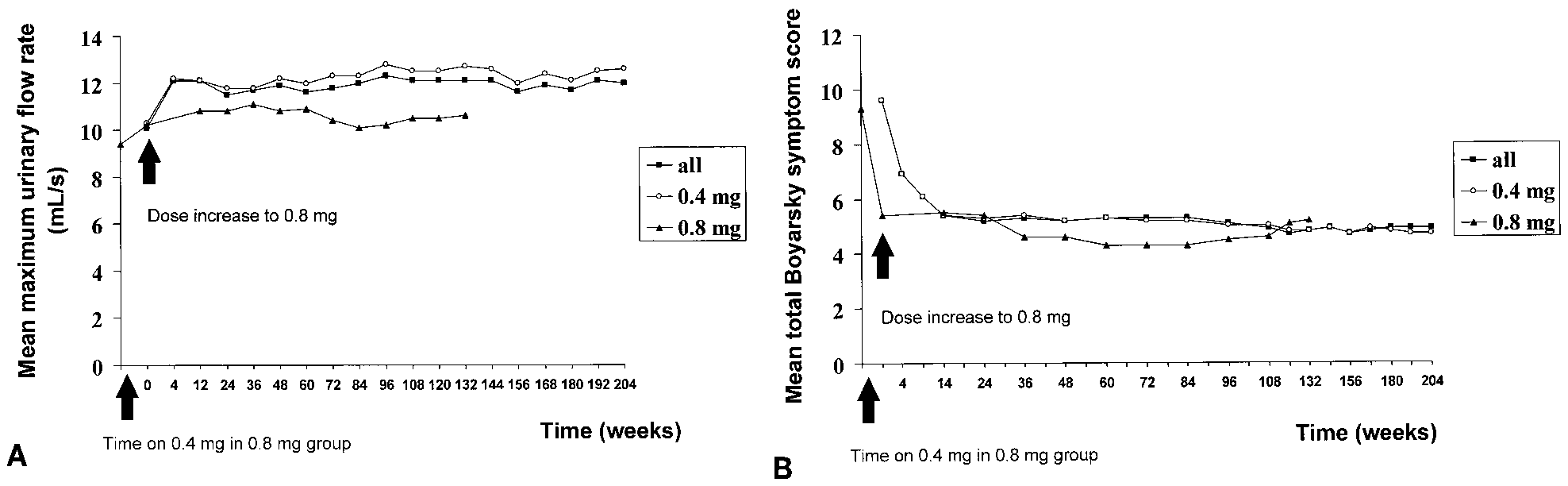
scores were significantly decreased from baseline at all visits. Changes in maximum urine flow and total symptom scorewith 0.8 mg. dose. Of the 512 patients in the intent-to-treat
population 421 (82%) remained on the 0.4 mg. dose, whereas
Mean digital rectal examination gm. prostate
in 91 (18%) the dose was increased to 0.8 mg. The group on
0.4 mg. tamsulosin had efficacy comparable to that in the
Mean ultrasound ml. prostate vol. Ϯ SD (No. pts.)
total population. Mean total symptom score decreased by 4.2
Mean Boyarsky symptom score Ϯ SD (No. pts.)
to 4.8 points (44% to 50%), while maximum urine flow in-
Mean ml./sec. max. urinary flow Ϯ SD (No. pts.)
creased by 1.2 to 2.1 ml. per second (11% to 20%). Meanmaximum urine flow at baseline in patients who changed to
TABLE 2. Cumulative number of patients who withdrew before each visit
* Some patients withdrew for more than 1 reason.
LONG-TERM TAMSULOSIN USE FOR URINARY TRACT SYMPTOMS
TABLE 3. Cumulative number of patients who withdrew before each
ment to a maximum of 79% and then remained more or less
visit according to geographic area
stable for the remainder of the trial. During this period theincidence of symptom score respondents was 74% to 81% (fig.
3, A). The incidence of those considered maximum urine flow
respondents was between 30% and 36% (fig. 3, B). When a
maximum urine flow response was defined as an increase of
3 ml. per second or greater, the rate was similar (28% to
35%). The mean total quality of life questionnaire score de-
creased 6.5 points from a baseline of 20.2 (Ϫ32%, p Ͻ0.001). Tolerability. During the 4 years of treatment 76% of pa-
tients had cumulatively at least 1 side effect, defined as anyevent occurring after the start of treatment or any event thatoccurred before tamsulosin was initiated but had increased
0.8 mg. was lower than in those who remained on 0.4 mg. (9.4
in intensity during treatment. However, only 26% of patients
versus 10.3 ml. per second). The mean maximum urine flow
had side effects that were considered by the investigator as
achieved with 0.4 mg. in these patients was less than in those
possibly or probably related to tamsulosin treatment (table
who remained on 0.4 mg. (10.2 versus 12.7 ml. per second).
4). The only drug related side effects in at least 3% of patients
The additional improvement in maximum urine flow at the
were dizziness in 5.8% and abnormal ejaculation in 4.3%.
0.8 mg. dose was minimal (range 0.2 to 0.7 ml. per second,
Overall 86 patients (17%) discontinued treatment before 4
years because of side effects (tables 2 and 4). Study with-
Total symptom score at baseline was comparable in the
drawal was considered possibly or probably drug related by
groups (0.8 and 0.4 mg. groups (9.3 and 9.6, respectively).
the investigator in 26 cases (5%). The most common side
Also, the effect of the 0.4 mg. dose in the 0.8 mg. group was
effects in at least 5 patients (1% or greater) that led to the
comparable to that in the 0.4 mg. group (decrease 3.8 and
discontinuation of treatment were urinary retention in 17
about 4.2 points, respectively, fig. 2, B). Increasing the dose
(3.3%, none considered drug related), prostatic disorder in 7
to 0.8 mg. had no substantial additional effect on the total
(1.4%, 1 considered drug related), dizziness in 5 (1%, all
symptom score. There was an increase of 0.1 points during
considered drug related) and impotence in 5 (1%, 3 consid-
ered drug related). A total of 117 patients (23%) had serious
Treatment responders and quality of life. Figure 3 shows
side effects during tamsulosin treatment for up to 4 years. In
the incidence of patients considered to have a total Boyarsky
addition, 2 patients died, including 1 from cardiac arrest and
symptom score response (25% or greater improvement) at
1 in a motor vehicle accident. The deaths were not related to
each time point. The number of total symptom score respon-
tamsulosin according to the investigator. Serious side effects
dents increased over the initial 14 weeks of tamsulosin treat-
that were considered drug related, such as urinary inconti-
FIG. 1. Long-term tamsulosin treatment. A, mean maximum urinary flow with time. At baseline and during treatment SD was 32 and 3.6
to 4.7 ml. per second, respectively. B, mean Boyarsky symptom score with time. At baseline and during treatment SD was 3 and from 2.6to 3.5 points during treatment, respectively. Versus baseline at all time points p Ͻ0.001.
FIG. 2. A, mean maximum urinary flow with time. B, mean total Boyarsky symptom score with time. At baseline and 12 weeks 89 patients,
24 weeks 74, 36 weeks 59, 48 weeks 54, 60 weeks 47, 72 and 84 weeks 44, 96 to 120 weeks 34 to 39 and 132 weeks 28.
LONG-TERM TAMSULOSIN USE FOR URINARY TRACT SYMPTOMS
FIG. 3. Treatment responders during long-term tamsulosin treatment. A, 25% or greater decrease in total Boyarsky symptom score from
baseline. B, 30% or greater increase in maximum urinary flow (Qmax) from baseline.
TABLE 4. Cumulative incidence of all reported and drug related
standing diastolic blood pressure compared with baseline. In
side effects in 515 patients treated with tamsulosin for up to 4
addition, no clinically relevant changes in laboratory param-
Our analysis shows that the efficacy of 0.4 mg. tamsulosin
once daily is sustained up to 4 years. Patients respond rap-
idly to tamsulosin and the improvement in symptoms that is
achieved within a few weeks is sustained during long-term
treatment. The improved maximum urine flow and decreased
symptom score are comparable to those in short-term
During this long-term extension study only 18% of patients
who did not respond optimally to 0.4 mg. tamsulosin and did
not report any drug related side effects had a dose increase to
0.8 mg. However, this dose increase seems not to have had a
substantial additional benefit based on improvements in
symptom score and maximum urine flow. Previously others
have also observed equal efficacy of 0.4 and 0.8 mg. tamsu-losin.4, 5, 10 The only statistically significant difference in the2 groups was a larger decrease in symptom score in the 0.8
nence, angina pectoris, penis disorder, cerebrovascular acci-
mg. group in 1 study. However, this difference was already
dent and dizziness, developed in only 5 patients (1%). The
evident after 1 week of tamsulosin treatment when patients
most common serious side effect in at least 5 patients (1% or
in the 0.8 mg. group were still on the 0.4 mg. dose.5 This
greater) were urinary retention in 17 (3.3%), prostatic disor-
finding indicates that the different effect on total symptom
der in 9 (1.7%), angina pectoris in 7 (1.4%) and prostatic
score was more likely caused by differences in the response in
carcinoma in 7 (1.4%). Of the 12 cases of urinary retention
patient groups than by differences in the response to the 0.4
that were severe enough to require hospitalization (acute
urinary retention), 5 (1%) developed within 1 and 7 (1.4%)
Throughout the study period, tamsulosin was well toler-
ated and the good safety profile was maintained up to 4
Table 5 shows standing and systolic blood pressure, and
years. Side effects considered to be probably or possibly re-
pulse rate at baseline and end point. Tamsulosin induced a
lated to tamsulosin were reported in 26% of cases. Only 5% of
small but statistically significant change in supine and
patients discontinued treatment due to these side effects.
TABLE 5. Supine and standing systolic and diastolic blood pressure, and pulse rate in patients treated with tamsulosin for up to 4 years
LONG-TERM TAMSULOSIN USE FOR URINARY TRACT SYMPTOMS
The most commonly reported drug related side effects were
urine flow and total Boyarsky symptom score were already
dizziness in 5.8% of cases and abnormal ejaculation in 4.3%.
significant after 4 weeks, when the initial assessment was
Other drug related side effects often associated with ␣1-
made in the controlled studies, and they were sustained for
adrenoceptor antagonists occurred at an incidence of less
up to 4 years of followup in patients who remained in the
than 3%. The incidence of drug related side effects in this
study. The safety profile also remained favorable during this
series was greater than in short-term 12-week placebo-
controlled studies.8 Since in open label long-term studies no
Ismar Healthcare NV assisted with manuscript editing.
placebo group is included, it is difficult to evaluate the inci-dence of side effects because the cumulative incidence ofcommon side effects tends to increase with time.
In European and American clinical trials abnormal ejacu-
lation was the only side effect that was or was not drug
1. Denis, L., McConnell, J., Yoshida, O. et al: Recommendations of
related that occurred more often with 0.4 mg. tamsulosin
the International Scientific Committee: the evaluation and
once daily than placebo (4.5% to 11% of cases).5, 8, 10 Abnor-
treatment of lower urinary tract symptoms (LUTS) suggestive
mal ejaculation, reported predominantly as retrograde ejac-
of benign prostatic obstruction. In: Proceedings of the 4th
ulation and decreased or absent ejaculate volume, is probably
International Consultation on Benign Prostatic Hyperplasia
related to the mode of action of ␣1-adrenoceptor antagonists,
(BPH); 1997 Jul 2–5. Edited by L. Denis, K. Griffiths, S. Khoury et al. Plymouth: Health Publication, p. 669, 1998
that is the relaxation of smooth muscle in the bladder neck,
2. Lepor, H., Kaplan, S. A., Klimberg, I. et al: Doxazosin for benign
vas deferens and seminal vesicles. Direct comparative trials
prostatic hyperplasia: long-term efficacy and safety in hyper-
of tamsulosin and alfuzosin9, 11 or terazosin12, 13 have shown a
tensive and normotensive patients. Multicenter Study Group.
comparable rate of abnormal ejaculation. Generally it is a
J Urol, 157: 525, 1997
well tolerated side effect. In this long-term extension study
3. Lepor, H.: Long-term efficacy and safety of terazosin in patients
only 1 patient (0.2%) discontinued treatment due to abnor-
with benign prostatic hyperplasia. Terazosin Research Group.
Urology, 45: 406, 1995
Acute urinary retention is the major complication of lower
4. Lepor, H.: Long-term evaluation of tamsulosin in benign pros-
urinary tract symptoms/BPH and in this study it was re-
tatic hyperplasia: placebo-controlled, double-blind extension of phase III trial. Tamsulosin Investigator Group. Urology, 51:
ported as a side effect. It may be considered an end point of
lower urinary tract symptoms/BPH treatment that should be
5. Narayan, P. and Lepor, H.: Long-term, open-label, phase III
prevented. The incidence of acute urinary retention during
multicenter study of tamsulosin in benign prostatic hyperpla-
watchful waiting or in placebo arms of clinical trials is low at
sia. Urology, 57: 466, 2001
1% to 1.5% yearly.14–16 In this long-term study 17 patients
6. Schulman, C. C., Cortvriend, J., Jonas, U. et al: Tamsulosin:
(3.3%) in 4 years were hospitalized due to acute urinary
3-year long-term efficacy and safety in patients with lower
retention. This incidence is comparable to that documented
urinary tract symptoms suggestive of benign prostatic obstruc-
for finasteride in a 4-year study17 and it warrants further
tion: analysis of a European, multinational, multicenter, open-
label study. European Tamsulosin Study Group. Eur Urol, 36:
After 4 years of tamsulosin treatment 34% of patients were
7. Abrams, P., Schulman, C. C. and Vaage, S.: Tamsulosin, a se-
still participating in the study. The discontinuation rate was
lective alpha 1C-adrenoceptor antagonist: a randomized, con-
comparable at most visits except at visit 6 (1 year). The much
trolled trial in patients with benign prostatic obstruction
higher withdrawal rate at this visit was attributable to the
(symptomatic BPH). European Tamsulosin Study Group. Br J
fact that patients were required to participate in the study
Urol, 76: 325, 1995
for at least 1 year. Often patients withdraw from open label
8. Chapple, C. R., Wyndaele, J. J., Nordling, J. et al: Tamsulosin,
studies because they no longer desire frequent visits and
the first prostate-selective ␣ -adrenoceptor antagonists. A
associated assessments, especially when the product be-
meta-analysis of two randomized, placebo-controlled, multi-
comes commercially available. This factor was clearly re-
centre studies in patients with benign prostatic obstruction
flected in the high discontinuation rate in all geographic
(symptomatic BPH). European Tamsulosin Study Group. Eur
areas in which tamsulosin became commercially available
Urol, 29: 155, 1996
9. Buzelin, J.-M., Fonteyne, E., Kontturi, M. et al: Comparison of
during the study period. Therefore, the number of patients
tamsulosin with alfuzosin in the treatment of patients with
who remain on long-term therapy in practice may be higher
lower urinary tract symptoms suggestive of bladder outlet
obstruction (symptomatic benign prostatic hyperplasia). Euro-
The most important side effects of ␣1-adrenoceptor antag-
pean Tamsulosin Study Group. Br J Urol, 80: 597, 1997
onists are dizziness, asthenia and postural hypotension. In
10. Narayan, P. and Tewari, A.: A second phase III multicenter
the group of ␣1-adrenoceptor antagonists 0.4 mg. tamsulosin
placebo-controlled study of 2 dosages of modified release tam-
and alfuzosin have the lowest degree of these side effects.18
sulosin in patients with symptoms of benign prostatic hyper-
However, alfuzosin has a more pronounced effect on blood
plasia. United States 93-01 Study Group. J Urol, 160: 1701,
pressure than tamsulosin, especially in elderly patients.19
The current study also indicates no clinically significant
11. Ho¨fner, K., Claes, H., De Reijke, T. M. et al: Tamsulosin 0.4 mg
daily: effect on sexual function in patients with lower urinary
change in blood pressure and a lower incidence of side effects
tract symptoms suggestive of benign prostatic obstruction. Eur
often associated with ␣1-adrenoceptor antagonists, such as
Urol, 36: 335, 1999
dizziness and asthenia, for tamsulosin than in other open
12. Lee, E. and Lee, C.: Clinical comparison of selective and non-
label studies of terazosin and doxazosin.2, 3 This finding con-
selective ␣1A-adrenoceptor antagonists in benign prostatic hy-
firms direct comparative data showing fewer vasodilatory
perplasia: studies on tamsulosin in a fixed dose and terazosin
drug related side effects for tamsulosin than equieffective
in increasing doses. Br J Urol, 80: 606, 1997
doses of terazosin.12, 13, 20 Overall tamsulosin has efficacy
13. Na, Y. J., Guo, Y. L., Gu, F.-L.: Clinical comparison of selective
comparable comparable to that of other ␣1-adrenoceptor an-
and non-selective alpha1A-adrenoceptor antagonists for blad-
tagonists but a much better safety profile.
der outlet obstruction associated with benign prostatic hyper- plasia: studies on tamsulosin and terazosin in Chinese pa- tients. Chinese Tamsulosin Study Group. J Med, 29: 289, 1998
14. Jacobsen, S. J., Jacobsen, D. J., Girman, C. J. et al: Natural
history of prostatism: risk factors for acute urinary retention.
Long-term treatment with tamsulosin is safe and well tol-
J Urol, 158: 481, 1997
erated in patients with lower urinary tract symptoms/BPH.
15. Wasson, J. H., Reda, D. J., Bruskewitz, R. C. et al: A comparison
Improvement in the primary efficacy parameters, maximum
of transurethral surgery with watchful waiting for moderate
LONG-TERM TAMSULOSIN USE FOR URINARY TRACT SYMPTOMS
symptoms of benign prostatic hyperplasia. Veterans Affairs
18. Djavan, B., Marberger, M.: A meta-analysis on the efficacy and
Cooperative Study Group on Transurethral Resection of the
tolerability of alpha1-adrenoceptor antagonists in patients
Prostate. N Engl J Med, 332: 75, 1995
with lower urinary tract symptoms suggestive of benign pros-
16. Barry, M. J., Fowler, F. J., Jr., Bin, L. et al: The natural history
tatic obstruction. Eur Urol, 36: 1, 1999
of patients with benign prostatic hyperplasia as diagnosed by
19. de Mey, C., Terpstra, I.: Orthostatic effects of alfuzosin twice
North American urologists. J Urol, 157: 10, 1997
daily vs. tamsulosin once daily in the morning. J Urol, suppl.,
17. McConnell, J. D., Bruskewitz, R., Walsh, P. et al: The effect of
163: 220, abstract 978, 2000
finasteride on the risk of acute urinary retention and the need
20. De Mey, C., Michel, M. C., McEwen, J. et al: A double-blind
for surgical treatment among men with benign prostatic hy-
comparison of terazosin and tamsulosin on their differential
perplasia. Finasteride Long-Term Efficacy and Safety Study
effects on ambulatory blood pressure and nocturnal orthostatic
Group. N Engl J Med, 338: 557, 1998
stress testing. Eur Urol, 33: 481, 1998
Lowe’s argument for dualism from mental causation Philosophia 33 (2005), p. 319-329 Abstract. E.J. Lowe has argued for dualism by trying to show that decisions are not only not identical to physical properties, but not even grounded in and reducible to them. His argumeknt does not warrant the conclusion. First, psychological evidence suggests that the scenario on which Lowe bases his cas
 LONG-TERM TAMSULOSIN USE FOR URINARY TRACT SYMPTOMS
TABLE 3. Cumulative number of patients who withdrew before each
ment to a maximum of 79% and then remained more or less
visit according to geographic area
stable for the remainder of the trial. During this period theincidence of symptom score respondents was 74% to 81% (fig.
LONG-TERM TAMSULOSIN USE FOR URINARY TRACT SYMPTOMS
TABLE 3. Cumulative number of patients who withdrew before each
ment to a maximum of 79% and then remained more or less
visit according to geographic area
stable for the remainder of the trial. During this period theincidence of symptom score respondents was 74% to 81% (fig.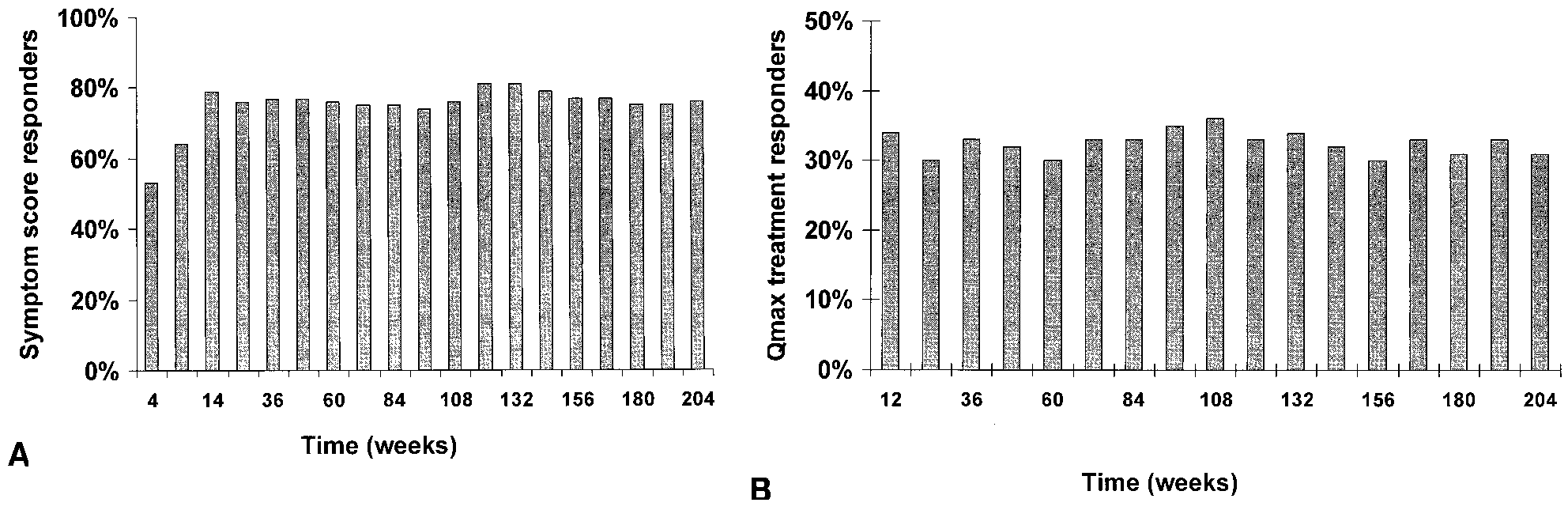 LONG-TERM TAMSULOSIN USE FOR URINARY TRACT SYMPTOMS
FIG. 3. Treatment responders during long-term tamsulosin treatment. A, 25% or greater decrease in total Boyarsky symptom score from
baseline. B, 30% or greater increase in maximum urinary flow (Qmax) from baseline.
LONG-TERM TAMSULOSIN USE FOR URINARY TRACT SYMPTOMS
FIG. 3. Treatment responders during long-term tamsulosin treatment. A, 25% or greater decrease in total Boyarsky symptom score from
baseline. B, 30% or greater increase in maximum urinary flow (Qmax) from baseline.