Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Num.uni-sb.de
Changes in Linear Dynamics of Cerebrovascular System After Severe Traumatic Brain Injury
M. Müller, MD; O. Bianchi; S. Erülkü; C. Stock; K. Schwerdtfeger, MD;
for the Homburg Traumatic Brain Injury Group
Background and Purpose—We sought to describe the dynamic changes in the cerebrovascular system after traumatic brain
injury by transfer function estimation and coherence. Methods—In 42 healthy volunteers (meanϮSD age, 37Ϯ17 years; range, 17 to 65 years), spontaneous fluctuations of
middle cerebral artery blood flow velocity and of finger blood pressure (BP) were simultaneously recorded over a periodof 10 minutes under normocapnic and hypocapnic conditions to generate normative spectra of coherence, phase shift,and gain over the frequency range of 0 to 0.25 Hz. Similar recordings were performed in 24 patients with severetraumatic brain injury (Glasgow Coma Scale score Յ8; meanϮSD age, 50Ϯ20 years) serially on days 1, 3, 5, and 8 aftertrauma. Cranial perfusion pressure was kept at Ͼ70 mm Hg. Each blood flow velocity/BP recording was related to thepresence or absence of middle cerebral artery territory brain parenchyma lesions on cranial CT performed within a closetime frame. Results—In controls, hypocapnia decreased coherence (0.0 to 0.20 Hz), increased phase shift (0.0 to 0.17 Hz), and
decreased gain in the frequency range of 0.0 to 0.11 Hz but increased gain at frequencies of 0.20 to 0.25 Hz (PϽ0.01for all frequency ranges reported). In patients with traumatic brain injury, 102 investigations were possible. Comparedwith controls, coherence was increased in the frequency range Ͻ0.03 Hz and between 0.13 and 0.25 Hz in bothnormocapnia and hypocapnia, irrespective of the CT findings. Gain was unchanged in normocapnia and in the absenceof a CT lesion. Gain was decreased in hypocapnia at frequencies Ͼ0.12 Hz irrespective of the presence/absence of aCT lesion. Phase shift decreased rapidly between 0.06 and 0.13 Hz under hypocapnic conditions and under normocapnicconditions in the presence of a CT lesion (PϽ0.01). Conclusions—Use of spontaneous fluctuations of blood flow velocity and BP to assess the cerebrovascular system
dynamically requires consideration of the PaCO2 level. In different conditions, including severe traumatic brain injury, the cerebrovascular system behaves linearly only in parts of the investigated frequency range. (Stroke. 2003;34:1197- 1202.) Key Words: cerebral circulation Ⅲ head injury Ⅲ transfer Ⅲ ultrasonography, Doppler, transcranial
Cerebral autoregulation (CA) is the ability of the cerebro- mathematically the intact system and to consider deviations
vascular system to provide a constant cerebral blood
as an impairment of the system involved in CA. Tiecks et al5
flow (CBF) supply to the brain in the presence of spontaneous
modeled CBF velocity changes as a second-order linear
blood pressure (BP) changes between 50 and 150 mm Hg
differential equation describing response to a rapid BP drop
(mean arterial BP). With the use of transcranial Doppler
and classifying the state of CA according to the time required
ultrasound (TCD), the integrity of CA is usually assessed by
by CBF velocity to return to its level before the decline in BP.
2-point static measuring methods by which CBF velocity is
Using transfer function analysis, other groups consider CA a
measured at rest and after a challenge induced by either BP
frequency-dependent filter system influencing the relation-
changes, CO2, or acetazolamide application as stressor.1–3 In
ship between corresponding frequencies in BP as input and
recent years, the fast time resolution of TCD had made
CBF velocity as output.6–8,10,11 The filter characteristics and
possible the development of dynamic methods for this pur-
hence the behavior of the filtering system are described by
pose. These dynamic methods analyze the relationship be-
phase shift, gain, and coherence. Phase shift is a correlate of
tween CBF velocity changes and BP changes by using either
the time delay between CBF velocity and BP; the time delay
differential equations empirically4,5 or transfer function anal-
is low at high frequencies, indicating that BP changes are
ysis.6–9 The underlying hypothesis is to accurately model
transmitted to CBF velocity; the time delay is high at low
Received August 3, 2002; final revision received November 26, 2002; accepted December 9, 2002. From the Departments of Neurology (M.M., O.B., S.E.) and Neurosurgery (K.S.), Saarland University Hospital, Homburg/Saar, and Institute for
Applied Mathematics, Saarland University, Saarbrücken (C.S.), Germany.
Correspondence to Martin Müller, MD, Department of Neurology, Saarland University Hospital, Kirrberger-Strasse, D-66421 Homburg/Saar,
2003 American Heart Association, Inc. Stroke is available at http://www.strokeaha.org DOI: 10.1161/01.STR.0000068409.81859.C5 1197 1198 Stroke
frequencies, indicating that BP changes are delayed before
a direct comparison between normocapnic and hypocapnic condi-
they affect CBF velocity. The energy (gain) transmitted from
tions in 63 arteries. Because hypoventilation is usually not used in
BP to CBF velocity is increased by the system at high
the treatment of acute severe TBI, we did not investigatehypercapnia.
frequencies but is clearly decreased by the system at lowfrequencies. Coherence describes the constancy over time of
TBI Patients
the phase relationship between CBF velocity and BP. A low
All procedures involved in the investigation of the TBI patients were
coherence, as found in the low-frequency range, indicates low
approved by the local ethics committee. We included 24 patients (19
phase shift stability; a high coherence, as found at higher
male, 5 female; meanϮSD age, 50Ϯ20 years) with severe TBI
frequencies, indicates a very stable relationship. In the
(Glasgow Coma Scale score Յ8)17 whom we intended to investigate
frequency-dependent model, any loss of these filter charac-
repeatedly on days 1, 3, 5, and 8 after trauma using the same TCD
teristics, such as lack of time delay at low frequencies, lack of
device and the same probe holder and by feeding the arterial line
gain increase at higher frequencies, or high coherence at low
signal into the TCD device. All patients had received a SpiegelbergIII system to be used as an external ventricular drainage device and
frequencies, can then be interpreted as a loss of CA.
to measure intracranial pressure (ICP). With the ICP known, cerebral
A correlation exists between the dynamic CA assessment
perfusion pressure as the difference between mean arterial BP and
methods and the static methods,5–7,12,13 prompting sugges-
ICP was maintained at Ͼ70 mm Hg with the use of catecholamines
tions that the dynamic approach to assess CA may be
and/or mannitol when necessary; other vasoactive substances such as
clinically useful.6,8,14–16 However, clinical experience with
glyceryl trinitrate or nimodipine were not used. All patients received
the dynamic CA assessment methods is limited. The static
regular cranial CT scan follow-ups within a close time frame with theTCD studies. At the time of investigation, the actual ICP was noted,
CA assessment methods provide convincing between-method
and the actual PaCO was measured by blood gas analysis. TCD
comparisons. Such comparisons between different dynamic
recordings were possible on 44 MCAs; the remainder were excluded
models suggest that the dynamic approach to CA is poorly
for reasons such as lack of a temporal bone window or TCD probe
understood and provides only fair between-model reproduc-
movements due to patient movement. The recording time ranged
ibility.8 Such a result may lead to doubts regarding whether
between 6 and 10 minutes. Although CT scanning is only a fair
the dynamic approaches are truly able to test CA or may
method to assess the total traumatic lesion extent, it can provide firstinsights into the relationship between brain lesion size and CA
suggest that the different models investigate different aspects
disturbances. To compare the CA assessment results with the
of the system.8 The aim of our study was to characterize the
morphological CT findings, we classified the brain parenchyma of
changes in cerebrovascular system behavior after severe
each MCA territory in terms of whether or not a traumatic brain
traumatic brain injury (TBI) with the understanding that, if
lesion was present. A traumatic subarachnoid hemorrhage (SAH)
the observed changes are in agreement with similar obser-
was present in 32 of 102 possible comparisons. In each SAH-positive
vations in other diseases, such a model-dependent repro-
CT scan, the parenchyma in the MCA territory under consideration
ducibility would strengthen the assumption that the dy-
showed a traumatic lesion, leading us to relate the SAH to the injuredparenchyma in each case.
namic approach can reflect the behavior of the system thatcontrols CA. Data Preparation For all data analyses, Matlab R12 (The MathWorks Inc) was used. Subjects and Methods
The TCD device collects the input data with a frequency of 50 data
Normal Subjects
points per second. We reduced the amount of data by averaging 100
With their written informed consent, 42 healthy subjects (23 male, 19
data points to 1 new data point every 2 seconds. The new data points
female; meanϮSD age, 37Ϯ17 years; age range, 14 to 71 years)
were normalized to their means [eg, (x-mean)/mean], and linear
without any cerebrovascular risk factors or neurological diseases
trends were removed by subtracting the straight line of best fit. A
underwent simultaneous recordings of middle cerebral artery (MCA)
6-minute recording time was reduced to approximately 200 data
CBF velocity (Multi DopX4, DWL; 2-MHz probe) and of BP at the
points. To compare the recordings with a standard length of
finger tip (Ohmeda 2300 Finapres) with the use of TCD. End-tidal
observation time, the first 128 data points of each time sequence
PaCO was measured with Enhancer 3000sx equipment (Diversified
were used (corresponding to a time period of 256 seconds).
Diagnostic Products Inc). The volunteers were lying in the supine
To calculate the coherence and the transfer function between BP
position. The Doppler probes were mounted on a light metal
and CBF velocity, we used Welch’s averaged periodogram method,
transcranial Doppler probe holder provided by the manufacturer, and
by which input (BP) and output (CBF velocity) signal sequences are
both MCAs were identified according to commonly accepted crite-
divided into subsets of equal length (64 seconds; thus, the lowest
ria. Because of a poor temporal bone window on 1 side in 3
frequency resolution is approximately 0.015 Hz). With the use of
volunteers, only 1 MCA was investigated in these subjects, while in
Hanning windows, a data overlap of 50% between 2 consecutive
the other subjects both MCAs were investigated, resulting in a total
subsets was achieved. With the use of fast Fourier transformation,
of 81 insonated arteries under normocapnic conditions. When the
the power spectrum of BP [Gbpbp(f)] and of CBF velocity [Gvv(f)]
subjects signaled that they were comfortable with the setting, the
and the cross-spectrum between BP and CBF velocity [Gbpv(f)]
recording of CBF velocity and BP began. During the 10-minute
were calculated for each subset. The coherence function [Coh(f)]
recording period, end-tidal PaCO values were collected every 20
seconds and summarized as a mean over the whole time period. After10 minutes the recording was stopped, and the volunteers were asked
to breathe in a forced manner. When forced breathing had induced asteady state of fallen end-tidal PaCO that could be maintained
Coherence values ranged between 0 and 1; 0 indicates no correlation,
comfortably by the volunteers, they were asked to maintain the
and 1 indicates perfect stability of the phase shift between input (BP)
intensity of forced breathing, and the recording of CBF velocity and
and output (CBF velocity [V]). Transferred to CA, 0 indicates that
BP was started again for 10 minutes. The end-tidal PaCO values
cerebral perfusion lacks any relation to BP, and 1 indicates that CBF
were again collected every 20 seconds and are reported as the mean
velocity follows BP changes with a perfectly stable phase shift. Such
value. Nine subjects refused to hyperventilate in the setting, allowing
a constant pressure-dependent perfusion is considered a total loss of
Müller et al Posttraumatic Cerebrovascular System Dynamics 1199
CA. The complex transfer function [TF(f)] is estimated as follows:
from which the gain is calculated and the phase shift is extractedfrom the real and the imaginary part of TF(f). The software we usedcalculates TF(f) according to the linear model
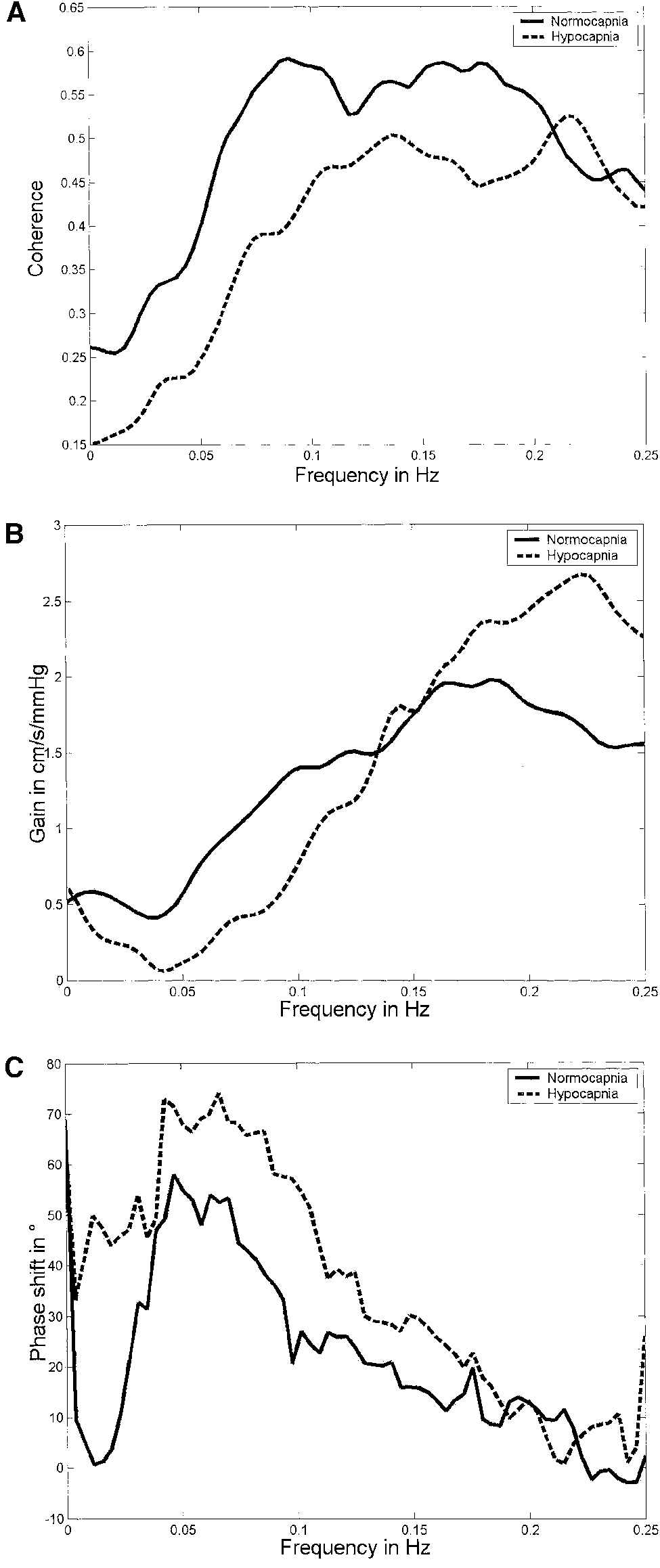
in which the output variable y(t)ϭ(V) is modeled by the lineartransfer function G applied to the input signal u(t)ϭ(BP). Statistical Analysis The data are reported as meanϮSD values. Transfer function and coherence results are plotted over the frequency range of 0 to 0.25 Hz. For simplicity of comparison, we plotted the curves of the mean values only. In the software we used, the frequency range contains 65 defined frequency points. At each frequency point, linear regression analysis was used to test for age and sex dependency for both normal subjects and TBI patients. To compare the effect of the PaCO2 changes within the controls, we used the paired t test. For compar- isons between controls and the different patient groups, we used the unpaired t test. We considered differences to be substantial when the t tests indicated significant differences over a broader frequency range with the understanding that a significant t test result at one or another frequency does not mean a physical finding. Thus, the reported limits of a frequency range indicate that all tests in the mentioned frequency range showed significant differences. We are aware that the testing includes multiple comparisons. To classify differences as substantial, we considered the level of significance for each t test as PՅ0.01. Normal Subjects Under normocapnia, end-tidal PaCO2 was 34Ϯ3 mm Hg and mean arterial BP was 88Ϯ9 mm Hg. Under hypercapnia, PaCO2 was lowered to 21Ϯ3 mm Hg, while mean arterial BP remained constant (89Ϯ9 mm Hg). Neither coherence, gain, nor phase shift showed a dependence on age or sex. Hypo- capnia substantially changed all 3 parameters: coherence (Figure 1A) was reduced in the frequency range between 0.0 and 0.20 Hz; gain (Figure 1B) decreased between 0.0 and 0.11 Hz but increased from 0.20 to 0.25 Hz; and phase shift (Figure 1C) was increased between 0.0 and 0.17 Hz (PϽ0.001 over each frequency range). TBI Patients Of the 24 patients, 5 were investigated once, 6 twice, 5 three times, and 8 four times. The trauma data were analyzed in terms of 3 considerations: first, we analyzed whether the patients were normocapnic or hypocapnic; second, recordings were summarized regarding whether or not a CT lesion was present, irrespective of the day of the recording; and third, the recordings were summarized at each day of recording, irre- spective of the CT findings. The 102 possible comparisons Figure 1. Changes of coherence (A), gain (B), and phase shift
were recorded on day 1 (nϭ29), day 3 (nϭ29), day 5 (nϭ25),
(C) during hypocapnia compared with normocapnia. Curves rep-
and day 8 (nϭ19). To classify normocapnia and hypocapnia,
resent mean values. Over a broad range of frequencies, coher-ence is significantly reduced and phase shift is increased. Gain
we used a threshold of PaCO2 of 36 mm Hg (hypocapnia,
is significantly reduced at Ͻ0.11 Hz but increased at Ͼ0.20 Hz.
Ͻ36.0 mm Hg). According to the actual PaCO2, 56 examina-tions were performed under normocapnic conditions and 46
cm in the presence of SAH. In each group (those without and
under hypocapnic conditions. A traumatic SAH was present
those with an SAH) there was 1 investigation during which a
in 17 investigations under normocapnic conditions and in 15
slight vasospasm according to Doppler criteria (mean flow
investigations under hypocapnic conditions. Mean MCA flow
velocity Ͼ120 cm/s) was present. In every instance cranial
velocity was 89Ϯ15 cm in the absence of SAH and 92Ϯ14
perfusion pressure was Ն70 mm Hg, and the maximum
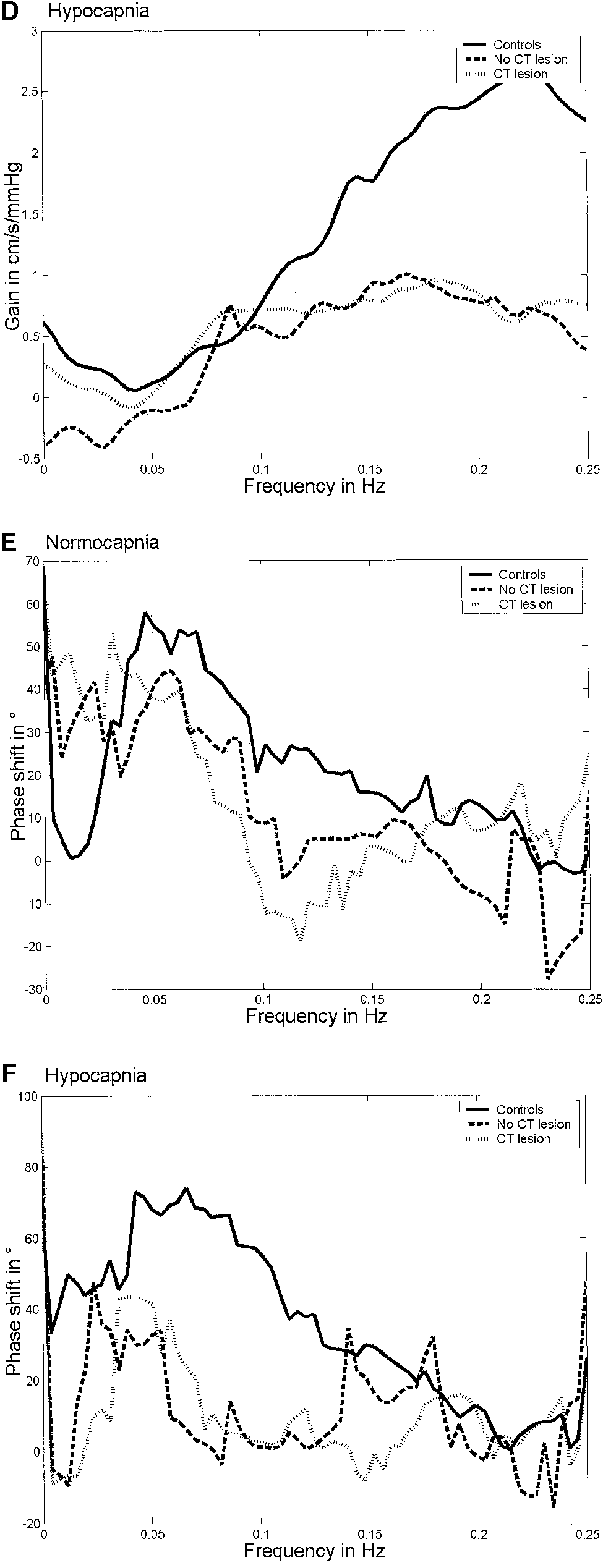
1200 Stroke Figure 2. Trauma-induced changes of coherence, gain, and phase shift compared with controls. Findings in the trauma patients are subdivided according to cranial CT results. For details of differences, see text. A, Coherence changes under normocapnic conditions. B, Coherence changes under hypocapnic conditions. C, Gain changes under normocapnic conditions. D, Gain changes under hypo- capnic conditions. E, Phase shift changes under normocapnic conditions. F, Phase shift changes under hypocapnic conditions. Müller et al Posttraumatic Cerebrovascular System Dynamics 1201
recorded ICP was 30 mm Hg. None of the CA assessment
peak of increase between 0.0 and 0.07 Hz, which corre-
results showed a correlation with age, mean arterial BP, ICP,
sponded to the gain peak of those patients without a CT lesion
cranial perfusion pressure, or patient outcome 1 month after
in normocapnia shown in Figure 2C. In hypocapnia, gain was
trauma. Despite the fact that the TBI patients were older than
substantially decreased between 0.13 and 0.25 Hz on days 1
the controls, we used the findings of the normal subjects as
to 5. On day 8 there was no difference between patients and
reference for comparison with the TBI patients because we
controls. In both normocapnia and hypocapnia, phase shift
and other investigators6 did not find the investigated linear
decreased substantially between 0.05 and 0.17 Hz on all days
except day 3 in normocapnia, on which phase shift was notdifferent from that of controls. The phase shift decline was of
Controls Versus Presence of CT Lesions,
the same shape as shown in Figure 2E and 2F. Irrespective of Day of Recording Figure 2 summarizes the substantial changes of coherence, Discussion
phase shift, and gain compared with controls with respect to
The cerebrovascular system regulates CBF or its first derivative
CBF velocity from the input power BP. We used the frequency-
In normocapnia (56 examinations, 35 with and 21 without
dependent filter model to describe changes in the linear behavior
a CT lesion; catecholamines were used in 21 recordings),
of this system. The major findings in the normal subjects may be
coherence was increased in the frequency range Ͻ0.03 Hz
described as follows: (1) a hypocapnia-induced linear behavior
and between 0.18 and 0.25 Hz, irrespective of the presence of
of coherence and phase shift changes over a wide frequency
a CT lesion. Under hypocapnic conditions (46 examinations,
range; this agrees with previously reported similar linearity
30 with and 16 without a CT lesion; catecholamines were
induced by hypercapnia6,7,13,18; and (2) a hypocapnia-induced
used in 19 recordings), coherence was increased between 0.0
S-shaped and hence nonlinear behavior of gain as an index of the
and 0.13 Hz and between 0.17 and 0.21 Hz when a lesion was
manner in which the system regulates the transmission of
not present; when a lesion was present, coherence was
energy. To our knowledge, such behavior has not been described
increased between 0.0 and 0.07 Hz and again between 0.11
previously. Zhang et al7 described, for hypercapnia, an increase
of gain in the frequency range between 0 and approximately 0.15
In hypocapnia (with and without a CT lesion) and in
Hz, an unchanged gain between 0.15 and 0.23 Hz, and an
normocapnia with a CT lesion, gain was reduced between
increased gain at Ͼ0.23 Hz, showing also a frequency range in
0.12 and 0.25 Hz. When a CT lesion was absent and the
which gain does not change. From the work of Panerai et al,19 it
patient was in a normocapnic state, gain was remarkably
can also be assumed that the cerebrovascular system can buffer
increased in the frequency range Ͻ0.05 Hz, while the gain in
sudden BP changes without changing its linearity and its linear
the faster frequency range did not differ from that of controls.
stability. However, such a buffering behavior argues for nonlin-
Phase shift was not different from that of controls over the
ear mechanisms within the system. The major finding in the TBI
whole frequency range when a CT lesion was not present
patients was the phase shift decrease between 0.05/0.06 Hz and
under normocapnic conditions. When a CT lesion was pres-
0.15 Hz. Similar phase shift decreases in this frequency range
ent, phase shift showed a rapid decline toward zero in the
have been reported for patients with severe carotid artery
frequency range between 0.05 and 0.16 and no difference in
disease,14 arteriovenous malformations,6 and spontaneous
the slower (Ͻ0.05 Hz) and the faster frequencies. In hypo-
SAH.20 In addition, the phase shift decreases in this frequency
capnia, phase shift was substantially decreased at Ͻ0.03 Hz
range have been shown to correlate significantly with impaired
and in the range between 0.06 and 0.13 Hz, irrespective of the
CO2 reactivity.6,14 One third of our investigations were per-
formed in the presence of a traumatic SAH. We cannot definitelyrule out that the similar phase shift behavior in our TBI patients
Controls Versus Day of Recording, Irrespective of
and in those with a spontaneous SAH20 is due to SAH-mediated
Presence of CT Lesions
mechanisms, but among them vasospasm did not play a role in
The 102 examinations were distributed with respect to day
and state of ventilation as follows: on day 1, 12 MCAs in
The changes in coherence and gain agree only in part with
normocapnia and 17 in hypocapnia; on day 3, 14 in normo-
the results found in TBI and in other diseases.11,14,15,21 It is
capnia and 15 in hypocapnia; on day 5, 16 in normocapnia
still undetermined whether systemic vasoconstrictors affect
and 9 in hypocapnia; and on day 8, 14 in normocapnia and 5
the behavior of the cerebral circulation.22 As stated above,
phase shift decreases comparable to our results were reported
Compared with controls, coherence was substantially in-
in patients with severe carotid artery disease14 or arterio-
creased over most of the frequencies under normocapnic and
venous malformations6 in which no vasoconstrictors were
hypocapnic conditions on day 1 (normocapnia, 0 to 0.25 Hz;
applied at the time of the TCD examination. This seems to
hypocapnia, 0.0 to 0.07 Hz and 0.13 to 0.21 Hz). On days 3
support the theory that vasoconstrictors do not affect CA
to 8, coherence was increased at Ͻ0.03 Hz in normocapnia
substantially. Regarding coherence, a possible explanation
and at Ͻ0.05 Hz in hypocapnia and showed a second
may be that the phase shift changes between 0.06 and 0.16 Hz
substantially increased peak occurring around 0.20 Hz, with
were too inhomogeneous to produce more consistent coher-
limits ranging between 0.13 and 0.25 Hz. Gain was neither
ence values. Thus, the question is whether the trauma induces
increased nor decreased on days 1, 5, and 8 under normocap-
phase shift changes, which interrupt the assumed linearity for
nic conditions. Only on day 3 did gain show a substantial
coherence found in the controls. Other possible explanations
1202 Stroke
for incongruent results include input power problems18; an
9. Kuo TB, Chern CM, Sheng XY, Wong WJ, Hu HH. Frequency domain
inhomogeneous population in which patients without CA
analysis of cerebral blood flow velocity and its correlation with arterialblood pressure. J Cereb Blood Flow Metab. 1998;18:311–318.
disturbances are included with those with loss of CA and the
10. Giller CA. The frequency-dependent behaviour of cerebral autoregu-
number of investigations for statistical analysis is low; or a
lation. Neurosurgery. 1990;27:362–368.
loss of linear stability of the system, a condition assumed to
11. Giller CA, Iacopino DG. Use of middle cerebral velocity and blood
be observed by Panerai et al,23 who demonstrated that the
pressure for the analysis of cerebral autoregulation at various frequencies:the coherence index. Neurol Res. 1997;19:634 – 640.
system behaved completely differently in TBI patients with
12. Newell DW, Aaslid R, Lam A, Mayberg TS, Winn R. Comparison of
ICP Ͼ20 mm Hg compared with TBI patients with ICP
flow and velocity during dynamic autoregulation testing in humans.
Ͻ20 mm Hg. Finally, the impressive phase shift changes
must be reconsidered when other mathematical models
13. Birch AA, Dirnhuber MJ, Hartley-Davies R, Iannotti F, Neil-Dwyer G.
Assessment of autoregulation by means of periodic changes in blood
emerge. Evidence is growing that parameters of resistance
pressure. Stroke. 1995;26:834 – 837.
and of storage capacity may have to be included into the
14. Hu HH, Kuo TB, Wong WJ, Luk YO, Chern CM, Hsu LC, Sheng W.
models or may be better targets to be controlled for than CBF
Transfer function analysis of cerebral hemodynamics in patients with
carotid stenosis. J Cereb Blood Flow Metab. 1999;19:460 – 465.
15. Czosnyka M, Smielewski P, Piechnik S, Steiner LA, Pickard JD. Cerebral
autoregulation following head injury. J Neurosurg. 2001;95:756 –763. Acknowledgments
16. Reinhard M, Hetzel A, Lauk M, Lucking CH. Evaluation of impaired
This study was supported by BMBF grant 01 KO 9707. For helpful
dynamic cerebral autoregulation by the Mueller manoeuvre. Clin Physiol.
comments on coherence functions, the authors thank Cole A. Giller,
MD, Department of Neurological Surgery, University of Texas,
17. Teasdale GM, Jennett B. Assessment and prognosis of coma after head
Southwestern Medical Center, Dallas.
injury. Lancet. 1974;2:81– 84.
18. Panerai RB, Deverson ST, Mahony P, Hayes P, Evans DH. Effect of CO2
References
on dynamic cerebral autoregulation. Physiol Meas. 1999;20:265–275.
19. Panerai RB, Dawson SL, Eames PJ, Potter JF. Cerebral blood flow
1. Widder P, Paulat K, Hackspacher J, Mayr E. Transcranial Doppler
velocity response to induced and spontaneous sudden changes in arterial
CO2-test for the detection of hemodynamically critical carotid artery
blood pressure. Am J Physiol. 2001;280:H2162–H2174.
stenoses and occlusions. Eur Arch Psychiatry Neurol Sci. 1986;236:
20. Lang EW, Diehl RR, Mehdorn HM. Cerebral autoregulation testing after
aneurysmal subarachnoid hemorrhage: the phase relationship between
2. Ringelstein EB, Sievers C, Ecker S, Schneider PA, Otis SM. Non-
arterial blood pressure and cerebral blood flow velocity. Crit Care Med.
invasive assessment of CO2-induced cerebral vasomotor response in
normal individuals and in patients with internal carotid artery occlusions.
21. Lang EW, Mehdorn HM, Dorsch NW, Czosnyka M. Continuous moni-
3. Müller M, Voges M, Piepgras U, Schimrigk K. Assessment of vasomotor
toring of cerebrovascular autoregulation: a validation study. J Neurol
reactivity by transcranial Doppler ultrasound and breath-holding: a com-
Neurosurg Psychiatry. 2002;72:583–586.
parison with acetazolamide as vasodilatory stimulus. Stroke. 1995;26:
22. Strebel SP, Kindler C, Bissonnette B, Tschaler G, Deanovic D. The
impact of vasoconstrictors on the cerebral circulation of anesthetized
4. Ursino M, Di Giammarco P. A mathematical model of the relationship
patients. Anesthesiology. 1998;89:67–72.
between cerebral blood volume and intracranial pressure changes: the
23. Panerai RB, Hudson V, Fan L, Mahony P, Yeoman PM, Hope T, Evans
generation of plateau waves. Ann Biomed Eng. 1991;19:15– 42.
DH. Assessment of dynamic cerebral autoregulation based on spon-
5. Tiecks FP, Lam AM, Aaslid R, Newell DW. Comparison of static and
taneous fluctuations in arterial blood pressure and intracranial pressure.
dynamic cerebral autoregulation measurements. Stroke. 1995;26:
Physiol Meas. 2002;23:59 –72.
24. Hughson RL, Edwardsd MR, O’Leary DD, Shoemaker JK. Critical anal-
6. Diehl RR, Linden D, Lücke D, Berlit P. Phase relationship between
ysis of cerebrovascular autoregulation during repeated head-up tilt.
cerebral blood flow velocity and blood pressure: a clinical test of auto-
regulation. Stroke. 1995;26:1801–1804.
25. Kirkham SK, Craine RE, Birch AA. A new mathematical model of
7. Zhang R, Zuckerman JH, Giller CA, Levine BD. Transfer function
dynamic cerebral autoregulation based on flow dependent feedback
analysis of dynamic cerebral autoregulation in humans. Am J Physiol.
mechanism. Physiol Meas. 2001;22:461– 473.
26. Mitis GD, Zhang R, Levine BD, Marmarelis VZ. Modelling of nonlinear
8. Panerai RB, Dawson SL, Potter JF. Linear and non-linear analysis of
physiological systems with fast and slow dynamics, II: application to
human dynamic autoregulation. Am J Physiol. 1999;277:H1089 –H1099.
cerebral autoregulation. Ann Biomed Eng. 2002;30:555–565.
The first World Conference on Breast Cancer acknowledged that higher levels of estrogen increased the risk of breast cancer. 27 out of 31 studies have found that even one abortion can increase the risk of developing breast cancer. Having a first child before the age of 18 years reduces the breast cancer risk dramatically. In first trimester miscarriages, the estradiol (estrogen) levels are usua
Topic: Structural Bioinformatics and Molecular DynamicsTHE EFFECT OF INHA FLEXIBILITY IN DOCKING SIMULATIONS WITHE Cohen1, K Machado1, O Norberto De Souza11Laborat´orio de Bioinform´atica, Modelagem e Simulac¸˜ao de Biossistemas - LABIO, Faculdadesde Inform´atica (PPGCC) e Biociˆencias (PPGBCM), PUCRS, Porto Alegre - RSMolecular docking is an important step of the rational drug desig
 Müller et al
Müller et al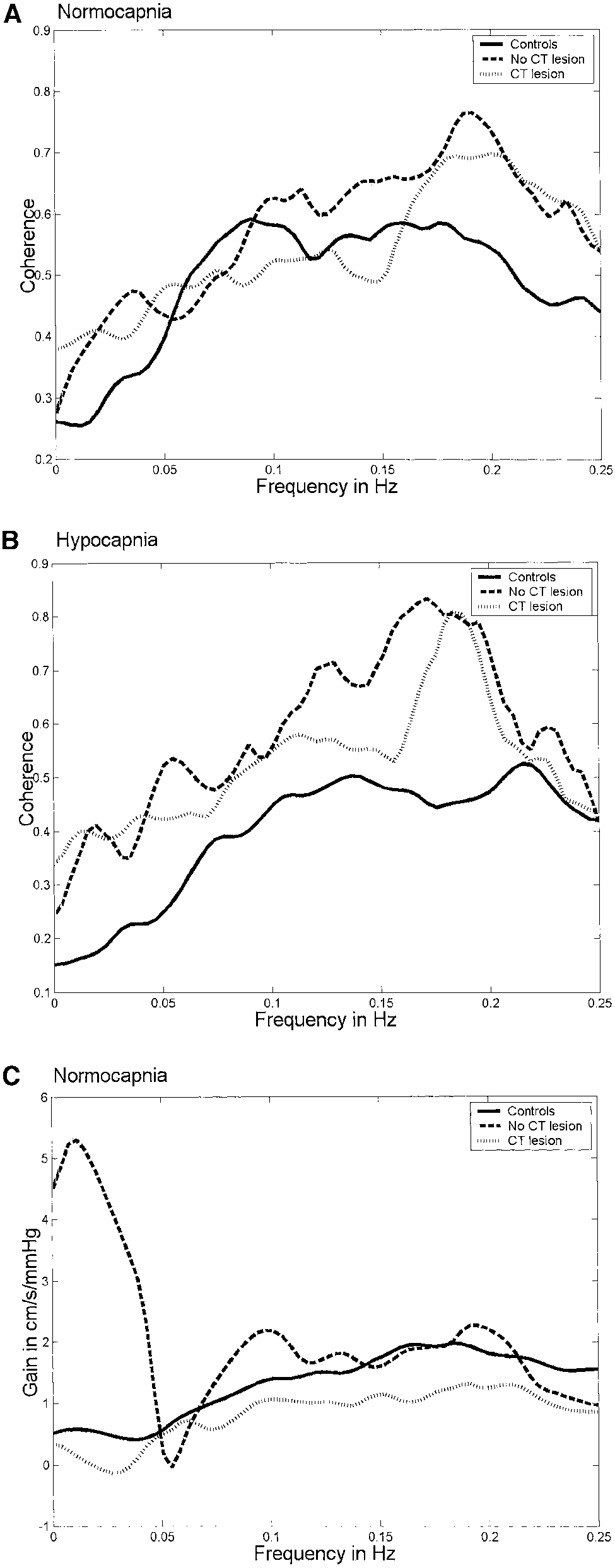
 1200
1200