Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Jhn_692 209.218
Vulnerable patients with a fractured neck of femur:nutritional status and support in hospital
M. Nematy,* M. Hickson,* A.E. Brynes,* C.H.S. Ruxton & G.S. Frost*
*Nutrition and Dietetic Research Group, Imperial College London, Hammersmith Hospitals Trust, London W12 0HS, UK; Schoolof Biosciences, University of Westminster, London W1W 6UW, UK
Malnutrition has serious consequences for
recovery and increases the risk of complications in hospital patients.
Fractured neck of femur (NOF) patients may be particularly at risk
because of their old age and frail state of health. We conducted an
observational study to evaluate the nutritional state and the nutri-
tional support, which was provided to this group during their stay in
Tel.: 020 8383 3048/014 8368 9384fax: 020 8383 3379
Twenty-five consecutive people admitted to an ortho-
paedic ward with a fractured NOF at Charing Cross Hospital, London
hospital, elderly, fractured neck offemur, hospital malnutrition,
were recruited. Anthropometric measures, biochemical indices,
nutritional status, nutritional support.
3 days dietary intake and dietetic referral rates were collected.
Patients had a significantly lower body mass index (BMI)
compared with the mean BMI for sex and age in an elderly UKpopulation (21.97 ± 1.06 versus 26.73 ± 0.03 kg m)2; P < 0.005). They took just 58.6% of their energy requirements in hospital(4219 ± 319 versus 7199 ± 202 kJ mean)1 daily intake over 3 days inweek 2). Using the hospitals own nutritional risk assessment tool 56%of patients were found to be at risk of malnutrition on admission,which increased to 68% after 2–3 weeks. Of these 64% were referredto a dietitian and were given nutritional supplements. Nutritionalassessment revealed that their nutritional status worsened duringstay.
This group of patients with fractured NOF is likely to
be malnourished on admission and to show a rapid deterioration inits nutrition status during admission. Energy needs were not met inup to 50% of patients. These results reinforce the need to screen,supplement and monitor fractured NOF patients.
currently accounting for 16% of the population
with an estimated rise to 20% by 2021 (Office of
Elderly people, aged over 65 years, are the fastest
national statistics, 2000). Falls are more common
growing section of the population in the UK,
in older age groups; one study estimated that 50%
Ó The British Dietetic Association Ltd 2006 J Hum Nutr Dietet, 19, pp. 209–218
of people over 80 years fall, compared with only
nutritional supplements are used in most hospitals
30% of people over 65 years (Vellas et al., 1992).
but their effectiveness varies (Milne et al., 2005),
Malnutrition has been suggested to increase the
probably because of reasons of palatability, prac-
risk of falls (Lumbers et al., 2003); to increase
ticality and also the influence of poor appetite.
recovery time and to account for a proportion of
This observational study was conducted to
disability and death in the elderly (Hayes et al.,
evaluate the nutritional status of a group of elderly
1996). The incidence of malnutrition in hospital-
patients admitted to an orthopaedic ward with a
ized over-80s is high (Corish & Kennedy, 2000).
fractured NOF and their nutritional support dur-
Therefore elderly orthopaedic in-patients are at
particular risk of a suboptimal nutritional status. This high risk of malnutrition in hospitalized
elderly is supported by a previous study, whichsuggested the nutritional intake of elderly female
patients recovering from a fractured neck of femur(NOF) is often inadequate (Older et al., 1980). We
This was a prospective study and local ethics
have previously presented insufficient energy in-
committee approval was obtained (RREC 3439/
take in patients with fractured NOF in abstract
2003). Patients who could read the information
sheet and acknowledged that they understand the
Clearly, early identification and treatment of
study gave written informed consent, and relatives
undernourished patients with fractured NOF who
gave assent prior to enrolment for those with
are at risk of poor nutritional status are essential
impaired vision. The inclusion criteria were male
(Beck & Ovesen, 1998). However, in practice it is
and female patients aged 65 years and over, with a
very difficult to re-feed sick and elderly patients.
fractured NOF resulting from a fall, who were
Oral supplements are predominantly suitable for
admitted to the orthopaedic wards at Charing
elderly people compared with nasogastric or ent-
eral feeds, as they are not invasive and are easy to
use. However, there may be problems with the
• Those unable to give informed consent and who
motivation and capability of older people to take
did not have relatives who could give assent.
oral supplements and therefore, supplements may
• NOF fracture following pathological conditions
not be consumed in sufficient amounts. One study
or road traffic accidents as these patients may have
showed that even if supplements are prescribed,
had associated complications that exaggerated or
staff may forget to give them to patients or, if they
complicated the assessment of nutritional status.
are given, they may not be consumed (Peak et al.,
• Those who were admitted for elective surgery
1998). A recent study identified patients who were
not meeting their estimated energy requirements,
• Patients who were enrolled in another concur-
then used supplements to achieve this goal.
However, the energy intake (EI) only increased to
The study was performed in accordance with the
a median of 67% of estimated requirements, sug-
gesting that insufficient supplements were con-sumed (Miller et al., 2005a).
One study has shown that, even with additional
feeding support, older patients did not eat enough
Nutritional and medical data were collected from
to achieve an adequate weight gain or nutritional
patients, charts, medical notes, nurses‘ files, care
status (Hickson et al., 2004). Possibly this failure
staff, dietitians, occupational therapists, physio-
to respond to feeding support is due to suppressed
therapists and the medical team. Parameters cor-
appetite; no matter how much assistance and
encouragement is given, if the appetite is poor,
anthropometrics [mid-arm circumference (MAC),
intake is unlikely to improve. At present,
height or demi-span, weight and body mass index
Ó The British Dietetic Association Ltd 2006 J Hum Nutr Dietet, 19, pp. 209–218
Nutritional status in fractured neck of femur patients
(BMI)] biochemical indices (albumin, total pro-
of infection, period of fasting and the need for
tein, C-reactive protein and haemoglobin) and
help with eating and drinking). In combination,
dietary intake were recorded. At the first visit it
these factors enable patients to be categorized as
was established which type of accommodation the
either high risk of malnutrition, moderate risk,
patient had been admitted from (own home,
sheltered housing, residential home and nursinghome), whether they lived alone, their alcohol
consumption and smoking status, their mobilitybefore admission, whether they were taking
Mid-arm circumference was assessed on admis-
medication or any food supplement, their previous
sion to the orthopaedic ward using standard pro-
history of falls and their general medical history.
tocols (Jensen et al., 1981; Gibson, 1993), by one
Subjects were followed-up, until discharged
researcher. After their operation, patients were
from hospital, to identify: malnutrition risk during
weighed using a chair scale (Weighcare, Marsden,
stay, referral to a dietitian, prescribed drugs
UK). The demi-span was measured to estimate
including antibiotics, Waterlow score change,
standing height in order to compute BMI (Bassey,
pressure sores occurrence, dietary supplement
use, physiotherapy mobility assessment, malnu-trition risk on discharge, and date and destination
The Elderly Mobility Scale (EMS) was seriallyperformed in patients with fractured NOF by
physiotherapists. This is a valid tool with good
Dietary intake was recorded over 3 days during
inter-rater reliability that could be readily applied
week 2 after the operation, using unweighed
during daily clinical work for measurement of
food records completed at ward level. Nurses
mobility of hospitalized elderly people (Prosser &
were given instructions on how to complete the
Canby, 1997). This scale scores between 0 (corre-
records and these were checked daily by the
sponding to complete dependence) to 20 (corre-
researcher. Where possible food charts were
sponding to complete independence). The EMS is
verified with the patient to make sure of
based on scoring seven actions including, (i) lying
to sitting, (ii) sitting to lying, (iii) sit to stand,
brought in by relatives. Mean daily energy and
(iv) stand, (v) gait, (vi) timed walk (6 m) and
nutrient intake was calculated from the food
records using the Dietplan5 computerized foodtables (Forestfield Software Ltd, West Sussex,
UK). Estimation of the total energy requirementof patients at the time of their food record was
The data were analysed using SPSS 12.0 for Win-
calculated by estimating basal metabolic rate
dows. All data were checked for normality and
(BMR) (Schofield, 1985), adding a stress factor
presented as mean and standard error of the
of 20% (to account for the increased energy
mean. An independent 2-tailed t-test was per-
requirements because of surgical correction of
formed to compare the nutritional parameters’
the fractured NOF) and adding another 10–25%
variables between patients and National Diet and
(based on the level of mobility in the ward) to
Nutritional Survey findings (Finch et al., 1998).
allow for rehabilitation, physical activity and
Paired t-tests were used to compare EI and energy
diet-induced thermogenesis. Malnutrition risk
requirements in each malnutrition risk group.
was also recorded from the hospital’s own
Analyses of variance with Bonferonni corrections
screening tool (Peak et al., 2000). This tool is
for multiple testing were used to compare EIs and
based on changes in dietary intake, weight and
energy deficits between the three malnutrition risk
other risk factors (pressure sore status, presence
Ó The British Dietetic Association Ltd 2006 J Hum Nutr Dietet, 19, pp. 209–218
consent. Demographics of patients, their past
medical history, mobility data, residence at time ofadmission and discharge, whether they lived alone
and length of stay in hospital are shown in Table 1.
Thirty-six patients were approached to take part. Of
Mean age was 85.3 ± 1.5 years, supporting previ-
these 25 were recruited and all completed the study.
ous studies which show an increased risk of NOF
A further eight patients were confused and unable to
fracture in the over 80s. The most common secon-
give informed consent and three refused to give
to an orthopaedic ward at Charing CrossHospital, London
*Nutrition risk was established using the local risk assessment tool, which incorporates dietaryintake, recent weight loss and other factors affecting intake or requirements. Elderly mobility scale runs from 0 to 20 with 20 corresponding to complete independence,anthropometric data shown are related to admission. MAC, muscle arm circumference; BMI, body mass index; COPD, chronic obstructive pulmonarydisease.
Ó The British Dietetic Association Ltd 2006 J Hum Nutr Dietet, 19, pp. 209–218
Nutritional status in fractured neck of femur patients
Table 2 Profile of BMI categories used to diagnose malnu-
females, who lived alone in their own home and
trition in patients with fracture neck of femur admitted to anorthopaedic ward (n ¼ 25)
were able to walk without an aid before the frac-ture. On discharge from hospital this picture
altered dramatically with only 44% of subjects able
Pain killers were used commonly during the
first week post-surgery. Antibiotics (cefuroxime,
ceftazidime, chloramphenicol, gentamicin and
nitrofurantoin) were prescribed for related com-
plications (urinary tract infections, conjunctivitis
*Suggested cut-off for people older than 75 years.
Commonly used cut-off in many prevalence studies. àWHO definition.
Table 1 shows the anthropometric profile of sub-
malnutrition risk assessment tool. The results for
jects. Compared with nationally representative
biochemical indices, food intake during week 2,
data from the UK National Diet and Nutritional
referral rates to the dietitian and the number of
Survey (Finch et al., 1998). Our patient group had
deaths in hospital are also given. Malnutrition risk
a significantly lower BMI (21.97 ± 1.06 versus
was high at admission with 56% (14 of 25) of
26.73 ± 0.03 kg m)2, P < 0.005). BMI is not the
patients either at moderate or high risk and this
best indicator of malnutrition risk, however it can
picture worsened during the stay to 68% (17 of 25).
offer a guide when used in combination with other
The food intake data collected in the second week
factors. There is no consensus in the literature as
revealed that mean daily EI was 59% of estimated
yet regarding the most appropriate cut-off point
energy requirements (4219 ± 319 kJ day)1 versus
for malnutrition risk in older people. However,
increasing evidence suggests that the BMI range
The biochemistry showed a picture of an acute
associated with the lowest risk of mortality is
phase response following the fracture and surgery
higher than previously thought in the over 75s
with C-reactive protein (CRP) rising and albumin
(Beck & Ovesen, 1998; Stevens, 2000) . For this
and total protein falling. Haemoglobin levels also
reason, we examined our data with respect to three
possible cut-off points and this analysis is shown
The screening tool used in this study recom-
mends that all high-risk patients are referred to
• 18.5 kg m)2, the WHO definition of the lower
the dietitian whereas moderate-risk patients are
limit for normal weight (World Health Organisa-
put on a nutrition care plan which incorporates
nurse-led interventions (such as giving ‘build-up’
• 20 kg m)2, the usual value used throughout the
drinks and encouraging intake at meal times).
literature to recognize malnourished elderly;
No data were collected on whether appropriate
• 24 kg m)2, suggested as the most appropriate
care plans were instigated for moderate-risk
cut-off to identify the elderly at-risk patient (Beck
patients in our study. However, referrals to the
dietitian were recorded showing that four of 11
The data show wide differences in the incidence
(36%) high-risk patients were not referred. Of
of ‘malnutrition’ depending on the cut-off used.
the seven patients referred to the dietitian (allwere from the high risk group), all were given astandard high-energy diet during week 2–4
(extra snacks and fortified choices on the menu).
Table 3 describes the nutritional assessment of
In addition to this, four were prescribed supple-
mented drinks and one was given a nasogastric
Ó The British Dietetic Association Ltd 2006 J Hum Nutr Dietet, 19, pp. 209–218
Table 3 Changes in the malnutrition risk, biochemical indices and energy intakes of fractured neck of femur patients during ahospital stay
*Assessed using the Hammersmith Hospital Nutrition Screening Tool (O’Flynn et al., 2005).
nutritionally at risk group (n ¼ 17) andthe not at risk group (n ¼ 8) of patients
BMI, body mass index; MAC, muscle arm circumference; CRP, C-reactive protein. Values pre-sented here are mean ± SEM.
feed. Of all 25 patients, five were prescribed irontablets by their doctor.
Comparison between the at risk group (n ¼ 17)
and the not at risk group (n ¼ 8) revealed that theformer demonstrated a significantly lower mean
weight, BMI, MAC and higher CRP on admissionand a significant lower EI during week 2 of stay
Figure 1 shows energy deficit and differences in
EI between the three risk groups. EI fell across thegroups with the lowest intakes seen in the ‘high
risk’ group (P ¼ 0.05 between the ‘not at risk’ and‘high risk’ groups). Paired t-tests showed that EI in
each risk group was significantly less than esti-
mated energy requirements, but there were no
significant differences between the energy deficits
Figure 1 Energy deficit (MJ day)1) in each malnutrition group
of patients with fractured neck of femur. Solid bar, mean
Within 9 months of entry to the study nine
energy intake; stripped bar, estimated energy requirement
patients had died. Seven of these were from the
(EER); mean energy intake in not at risk versus high risk +,P ¼ 0.05. Energy intake in each group was significantly less
‘high risk’ group, one from the ‘moderate risk’
than EER *,P < 0.005, P ¼ 0.001 and P ¼ 0.02 versus EER
group and one was from the ‘not at risk’ group.
Ó The British Dietetic Association Ltd 2006 J Hum Nutr Dietet, 19, pp. 209–218
Nutritional status in fractured neck of femur patients
from surgery for a fractured NOF. This would
serve to lower estimated energy requirements in
The mean length of stay in this group of emer-
gency surgical patients was 36.2 ± 4.7 days. This
Although we aimed to collect malnutrition
is significantly longer than the 5 days average for
status on discharge for this cohort it proved
surgical patients admitted to this hospital. The
extremely difficult. Patients were moved around
mean score of 8.4 on the EMS on discharge sug-
the hospital and often transferred out to rehabil-
gests that patients were highly dependent on
itation centres with little or no warning. Thus, our
mobility aids and devices and would require
data for this period are not reliable enough to
ongoing physiotherapy and occupational therapy,
present. Nevertheless the data presented here
represent convincing evidence that a more activeand aggressive approach to nutritional support inthis patient group is justified. Our data do show
that independence is compromised after hip frac-
This study confirms that hip fracture patients are
ture and this may further affect patients’ abilities
an elderly and particularly frail group and that the
to eat and drink, or shop and cook, once dis-
event of a hip fracture alters dramatically the
prognosis and level of independence of the indi-
It should also be noted that our study group is
vidual. We have also shown that the nutritional
not truly representative of the usual geriatric
status of such patients can deteriorate dramatic-
patient population as we were unable to recruit
ally during the first 1–2 weeks of their hospital
cognitively impaired patients. Such patients are
stay, due in part to a severely reduced food intake,
more likely to be malnourished and have a greater
as shown by the food intake data. Even with a well-
risk of deteriorating nutritional status.
established and monitored screening tool in place
Furthermore, evidence shows that following a
a third of the patients in this study who merited
period of restricted intake and weight loss, older
dietetic referral were not referred. It is not known
adults are less likely to compensate by eating more
whether the mortality figures in our study were
and regaining weight. Roberts et al. (1994) dem-
influenced by this failure to address malnutrition,
onstrated that young men quickly regained weight
although other studies have clearly demonstrated
by eating more whereas old men did not adapt and
that the risk of mortality increases when nutri-
continued to restrict their EI, further exacerbating
tional status is poor (Kagansky et al., 2005).
weight loss. Every effort was made to record all the
Energy needs were not met in up to 50% of
food and drinks which patients consumed how-
patients. The energy requirements for these pa-
ever there might be a few instances of under-
tients to maintain weight were estimated by taking
reporting. All the patients in our study ate less
into account additional energy needs postopera-
than their estimated requirements, thus even the
tively and current activity levels. Although 36% of
patients with the best recovery may continue to
lose weight once discharged. This would contrib-
(BMI < 20 kg m)2), we did not adjust their energy
ute to longer-term mortality and loss of inde-
requirements to include a factor for gaining
weight. This was because of the difficulty in
The mechanisms controlling appetite and this
meeting requirements to simply maintain weight.
lack of adaptation to poor intake observed with
Attempting to gain weight at this stage may be
ageing have yet to be fully elucidated but, in this
considered unrealistic. In addition, bed rest im-
patient group, the reasons for the poor food intake
pacts on energy expenditure and, thus energy
are likely to be linked to both physiological and
requirements. (Miller et al., 2005b) reported that
pathological factors. Patients often have a lower
resting metabolic rate was lower in the late post-
food intake because of pain, nausea, confusion,
operative period (day 10–42) compared with the
immobility and drug side-effects, at a time when
early postoperative period in patients recovering
they have increased energy requirements. Factors
Ó The British Dietetic Association Ltd 2006 J Hum Nutr Dietet, 19, pp. 209–218
relating to hospital food provision will also play a
some of the patients in rehabilitation centres may
role, such as lack of choice, unfamiliar foods and
also have returned home given time. A similar low
mealtimes, unpleasant environmental factors, eat-
rate of recovery to independence was shown by
ing alone and lack of assistance. Possibly physio-
Delmi et al. (1990) who reported 50–60% of patients
logical factors associated with appetite suppression
returning to their own home. These data suggest
also play an important role. Hickson et al. (2004)
that the major trauma of a hip fracture and subse-
highlighted the difficulties of improving the intake
quent surgical repair may hasten the end of a per-
of acutely ill elderly patients during a hospital stay.
Additional support at mealtimes was given to
Nutrition assessment of our patients suggested
patients in this study, yet no significant changes in
that their nutritional status was poor prior to
weight or nutritional status were seen. A similar
admission to hospital. Quite how prevalent mal-
finding was seen in the study of Delmi et al. (1990).
nutrition was in this patient group depends on the
Daily oral supplements were given to 27 elderly
classification of malnutrition risk used. We have
patients with fractured NOF for 32 days but, despite
clearly shown that different BMI cut-off points
adequate energy provision, nutritional require-
dramatically alter the number of potentially mal-
ments were not met during the hospital stay.
Appetite may be the limiting factor, perhaps
(<18.5 kg m)2) gives the lowest incidence of
exacerbated by the dulling of taste and smell which
malnutrition risk, but the data for this cut-off
point were derived mainly from young healthy
A range of neural and endocrine factors control
adults. The usual value of <20 kg m)2 provides an
appetite. Appetite reduction during ageing is
incidence of malnutrition risk of 36%, comparable
possibly related to gastric distension (Sturm et al.,
with many published studies (McWhirter & Pen-
2004) and changes in gut hormone release (Cum-
nington, 1994; Corish & Kennedy, 2000). The no-
mings et al., 2001; Le Roux & Bloom, 2005). There
vel value of 24 kg m)2 suggests that 72% of the
is an intriguing possibility that regulatory appetite
patients are at risk of malnutrition (Stevens, 2000).
peptides may be changed by acute illness resulting
The range of 23.5–24.9 kg m)2 was the BMI cate-
in a depressed appetite (Nematy et al., 2005).
gory with the lowest hazard ratio among those
Much work is still needed to understand appetite
>75 years, with the lowest mortality relating to the
regulation in general but particularly in this
high end of this BMI range (Stevens, 2000). Thus,
if the data of Stevens (2000) can be confirmed, the
Our other findings reflect those of other studies. A
prevalence of malnutrition in our patient group
systematic review has reported that the mean age of
was extremely high. It is also similar to the inci-
hip fracture patients is usually over 80 years (Av-
dence found with the nutrition screening tool,
enell & Handoll, 2003). A study on 114 hip fracture
where 56% of patients were at risk on admission.
patients showed 49% had a history of hypertension
Further work is needed to reach a consensus on
(Van et al., 1998) comparable with our finding of
the ‘normal’ BMI range, which is most appropriate
60%. It is not known if patients who had fractured
NOF secondary to fall underwent orthostatic
The main weakness of this study is the small
hypotension or transient ischaemic attacks. Tinetti
sample size and the lack of data from the end of
et al. (1986) who studied fall risk index for elderly
the hospital stay. Further work is required to
patients based on number of chronic disabilities
verify these findings and additional research is
reported that a postural drop in blood pressure was
needed to investigate ways to treat the nutritional
correlated with falls. Several studies have demon-
deficits in this patient group. Perhaps the most
strated an association between malnutrition and an
promising new information will come from work
increased risk of complications (Sullivan et al.,
investigating appetite control during ageing, dis-
1990) and extended length of stay (Paillaud et al.,
2000), which support our finding of 36.2 days. Our
The main implication of this work is to highlight
study found 44% returned their own home, but
the importance of early nutritional assessment in
Ó The British Dietetic Association Ltd 2006 J Hum Nutr Dietet, 19, pp. 209–218
Nutritional status in fractured neck of femur patients
this patient group and the urgent need for timely
Bassey, EJ. (1986) Demi-span as a measure of skeletal size.
intervention. Dietitians working with fractured
NOF patients should seek to ensure that all
Beck, A.M. & Ovesen, L. (1998) At which body mass index
and degree of weight loss should hospitalized elderly
patients are screened early after admission and
patients be considered at nutritional risk? Clin. Nutr. 17,
given appropriate nutritional support. It may be
more effective and time-saving to instigate a policy
Corish, C.A. & Kennedy, N.P. (2000) Protein-energy
requiring supplementation in all NOF in-patients
undernutrition in hospital in-patients. Br. J. Nutr. 83,
over 80 years during the first 2 weeks of their
Cummings, D.E., Purnell, J.Q., Frayo, R.S., Schmidova, K.,
Wisse, B.E. & Weigle, D.S. (2001) A preprandial rise inplasma ghrelin levels suggests a role in meal initiation in
Delmi, M., Rapin, C.H., Bengoa, J.M., Delmas, P.D., Vasey,
Patients with a fractured NOF were likely to be
H. & Bonjour, J.P. (1990) Dietary supplementation in
malnourished on admission and showed a rapid
elderly patients with fractured neck of the femur. Lan-cet. 335, 1013–1016.
deterioration in their nutrition status during
Finch, S., Doyle, W. & Lowe, C. (1998) National Diet and
hospital stay. There was failure to meet energy
Nutrition Survey: People aged 65 years and over, Vol. 1.
needs by as much as 50%. ‘Patchy’ screening
Report of the Diet and Nutrition Survey. London: H.M.
resulted in a low number of referrals for dietetic
care and consequently exacerbated nutrient defi-
Gibson, R.S. (1993) Nutritional Assessment. Oxford: Oxford
cit. These results reinforce the need to screen,
Hayes, W.C., Myers, E.R., Robinovitch, S.N., Van Den, K.A.,
supplement and monitor fractured NOF patients.
Courtney, A.C. & McMahon, T.A. (1996) Etiology and
There is also a need to understand the metabolic
prevention of age-related hip fractures. Bone. 18 (Suppl.
processes and appetite regulation in this extremely
Hickson, M., Bulpitt, C., Nunes, M., Peters, R., Cooke, J.,
Nicholl, C. & Frost, G. (2004) Does additional feedingsupport provided by health care assistants improve
nutritional status and outcome in acutely ill olderin-patients?–a randomised control trial. Clin. Nutr. 23,
CR conceived the study and CR, GF, MH, were
responsible for designing the study. MN was
Jensen, T.G., Dudrick, S.J. & Johnston, D.A. (1981) A com-
responsible for recruiting patients, data collection,
parison of triceps skinfold and upper arm circumferencemeasurements as taken in standard and supine positions.
analysis, statistical analysis and manuscript pre-
JPEN J. Parenter. Enteral. Nutr. 5, 519–521.
paration. GF, AB and MH, supervised the data
Kagansky, N., Berner, Y., Koren-Morag, N., Perelman, L.,
collection and analysis. All authors read and
Knobler, H. & Levy, S. (2005) Poor nutritional habits are
predictors of poor outcome in very old hospitalizedpatients. Am. J. Clin. Nutr. 82, 784–791.
Le Roux, C.W. & Bloom, S.R. (2005) Peptide YY, appetite
and food intake. Proc. Nutr. Soc. 64, 213–216.
Lumbers, M., New, S.A., Gibson, S. & Murphy, M.C. (2003)
We thank orthopaedic staff at Charing Cross hospital
Nutritional status in elderly female hip fracture patients:
for facilitating recruitment and collecting and record-
comparison with an age-matched home living group
ing data from patients. The authors would like to
attending day centres. Br. J. Nutr. 85, 733–740.
thank the University of Westminster for the clinical
McWhirter, J.P. & Pennington, C.R. (1994) Incidence and
research grant that supported this work.
recognition of malnutrition in hospital. BMJ. 308, 945–948.
Miller, M.D., Daniels, L.A., Bannerman, E. & Crotty, M.
(2005a) Adherence to nutrition supplements amongpatients with a fall-related lower limb fracture. Nutr.
Avenell, A. & Handoll, H.H. (2003) A systematic review
of protein and energy supplementation for hip frac-
Miller, M.D., Daniels, L.A., Bannerman, E. & Crotty, M.
ture aftercare in older people. Eur. J. Clin. Nutr. 57,
Ó The British Dietetic Association Ltd 2006 J Hum Nutr Dietet, 19, pp. 209–218
longitudinally following hip fracture compared to pre-
malnutrition to plan and target nutritional support
dictive equations: is an injury adjustment required?. Br.
strategies. Proc. Nutr. Soc. 59, 139A.
Prosser, L. & Canby, A. (1997) Further validation of the
Milne, A.C., Potter, J. & Avenell, A. (2005) Protein and
Elderly Mobility Scale for measurement of mobility of
energy supplementation in elderly people at risk from
hospitalized elderly people. Clin. Rehabil. 11, 338–343.
Roberts, S.B., Fuss, P., Heyman, M.B., Evans, W.J., Tsay, R.,
Rasmussen, H., Fiatarone, M., Cortiella, J., Dallal, G.E. &
Nematy, M., Hickson, M., Brynes, A., Ruxton, C. & Frost, G.
Young, V.R. (1994) Control of food intake in older men.
(2004) A pilot survey to investigate the nutritional status
of patients with a fractured neck of femur and level of
Schofield, W.N. (1985) Predicting basal metabolic rate, new
nutritional support provided during treatment. In Pro-
standards and review of previous work. Hum. Nutr.
ceedings of The Nutrition Society (0029–6651) 063(01B),
77A, September. 2004. Ref type: Abstract. CABI Pub-
Stevens, J. (2000) Impact of age on associations between
weight and mortality. Nutr. Rev. 58, 129–137.
Nematy, M., O’Flynn, J.E., Wandrag, L., Brynes, A.E., Brett,
Sturm, K., Parker, B., Wishart, J., Feinle-Bisset, C., Jones,
S.J., Patterson, M., Ghatei, M.A., Bloom, S.R. & Frost,
K.L., Chapman, I. & Horowitz, M. (2004) Energy intake
G.S. (2005) Changes in appetite related gut hormones in
and appetite are related to antral area in healthy young
intensive care unit patients: a pilot cohort study. Crit.
and older subjects. Am. J. Clin. Nutr. 80, 656–667.
Sullivan, D.H., Patch, G.A., Walls, R.C. & Lipschitz, D.A.
Office of national statistics. (2000) Regional Trends 35: 2000
(1990) Impact of nutrition status on morbidity and
mortality in a select population of geriatric rehabilita-
O’Flynn, J., Peake, H., Hickson, M., Foster, D. & Frost, G.
tion patients. Am. J. Clin. Nutr. 51, 749–758.
(2005) The prevalence of malnutrition in hospitals can
Tinetti, M.E., Williams, T.F. & Mayewski, R. (1986) Fall risk
be reduced: results from three consecutive cross-sec-
index for elderly patients based on number of chronic
tional studies. Clin. Nutr. 24, 1078–1088.
disabilities. Am. J. Med. 80, 429–434.
Older, M.W., Edwards, D. & Dickerson, J.W. (1980) A nu-
Van Hoang, H., Silverstone, F.A., Leventer, S., Wolf-Klein,
trient survey in elderly women with femoral neck frac-
G.P. & Foley, C.J. (1998) The effect of nutritional status
on length of stay in elderly hip fracture patients. J. Nutr.
Paillaud, E., Bories, P.N., Le Parco, J.C. & Campillo, B.
(2000) Nutritional status and energy expenditure in el-
Vellas, B., Baumgartner, R.N., Wayne, S.J., Conceicao, J.,
derly patients with recent hip fracture during a 2-month
Lafont, C., Albarede, J.L. & Garry, P.J. (1992) Relation-
follow-up. Br. J. Nutr. 83, 97–103.
ship between malnutrition and falls in the elderly. Nu-
Peak, H.J., Evan, S., Chambers, A., Riches, C. & Frost, C.G.
(1998) Nutritional supplementation: how much do
World Health Organisation (1995) Physical status: the Use
people drink?. Proc. Nutr. Soc. 57, 94A.
and Interpretation of Anthropometry. Geneva: Report of
Peak, H., Evans, S., Maltby, A.A., Bartram, J. & Frost, G.
(2000) Determining the incidence of hospital trust
Ó The British Dietetic Association Ltd 2006 J Hum Nutr Dietet, 19, pp. 209–218
KemiForsøget Gert Bergstein, kemistyrelsen coffein (trivialnavn) dss. thein (triv.), 1,3,7-trimethyl-7 H -purin-2,6(1 H ,3 H )-dion [58-08-2] I sidste nr. af LMFK-bladet forsøgte jeg at in-troducere KemiForsøget. Det var mit håb, at det kunne være et fast punkt i bladet, men det vil afhænge af bidrag fra jer læsere. Jeg har ik-ke fået nogen bidrag, men vil give det en chan-ce
Dannielle Tegeder 118 Union Street 7B, Brooklyn, N.Y. 11231 (917) 885-7857 dmtegeder@gmail.com ______________________________________________________________________ Education MFA, School of the Art Institute of Chicago, IL BFA, State University of New York at Purchase, NY Amsterdam School of Fine Arts, the Netherlands Solo Exhibitions Solo Project, Montclair Art Mu
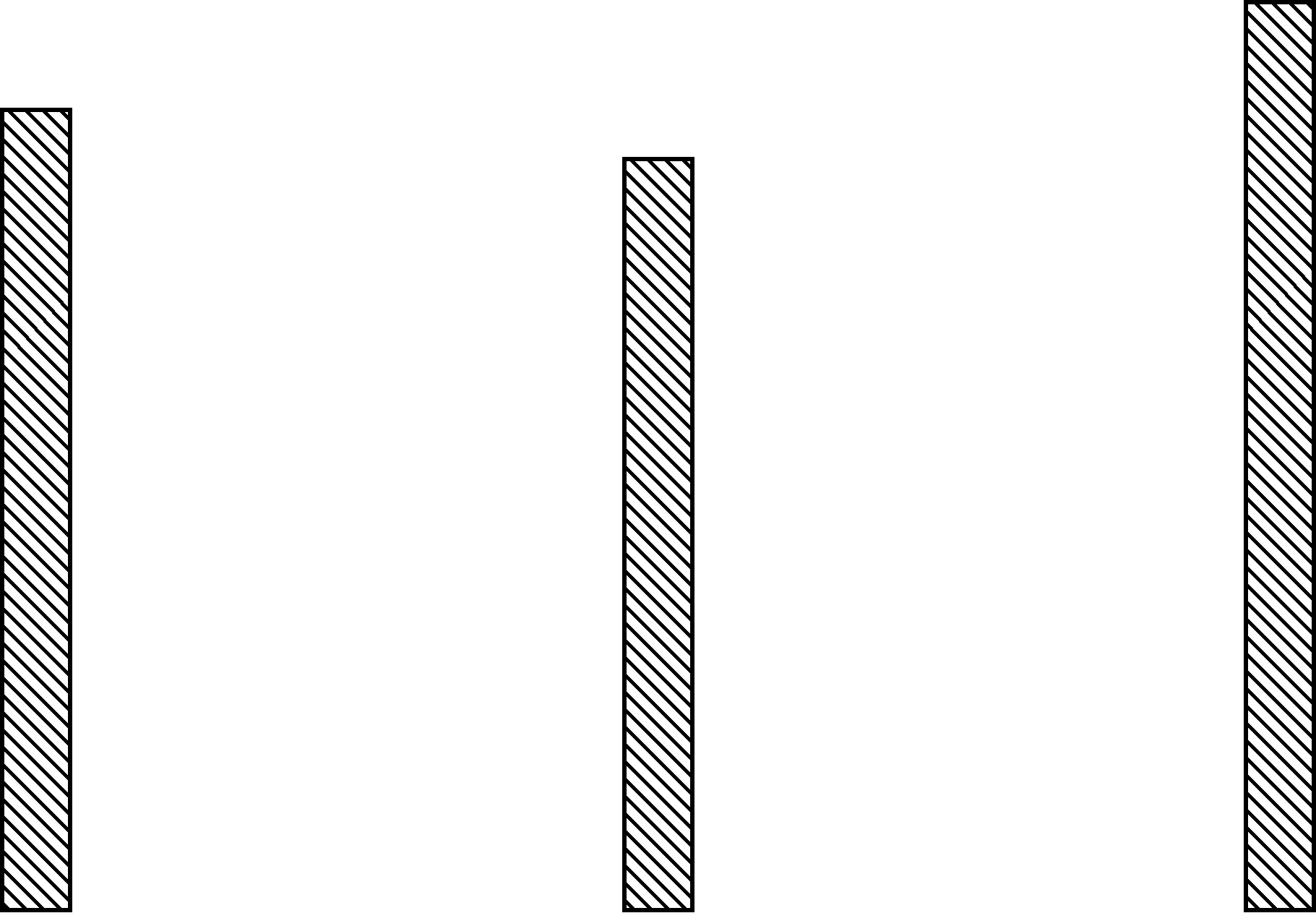 Table 3 Changes in the malnutrition risk, biochemical indices and energy intakes of fractured neck of femur patients during ahospital stay
*Assessed using the Hammersmith Hospital Nutrition Screening Tool (O’Flynn et al., 2005).
Table 3 Changes in the malnutrition risk, biochemical indices and energy intakes of fractured neck of femur patients during ahospital stay
*Assessed using the Hammersmith Hospital Nutrition Screening Tool (O’Flynn et al., 2005).