Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Microsoft word - painques revision.doc
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
Name: _____________________________________ Date: ____________ Birthdate: ________
Who referred you? ______________________________________________ Phone: __________
Who is your treating physician now? ________________________________ Phone: __________
Describe the pain you have right now (e.g. aching, burning, sharp, etc:) Where is it? What is it like?
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
When did the pain begin? __________________________________________________________
If it began with an injury, please describe: _____________________________________________
______________________________________________________________________________
______________________________________________________________________________
Employer when injured: ___________________________________________________________
Position: _______________________________________________________________________
How long employed? ______________ Last day worked: ____________ Still employed? Y N
Have you had pain or injury in this part of your body before? Y N (If yes, describe:) ___________
______________________________________________________________________________
Ever had any other injuries before? Y N (If yes, describe & give dates:) _____________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Total number of surgeries for your pain: ___________
How many times have you been to the Emergency Room in the past 6 months because of pain? __
How many times have you been Hospitalized in the past 12 months because of pain?___________
Rate your usual pain on a scale of 0 to 10 by putting an "x" on the line:
( ) Several times a month ( ) Once a month
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
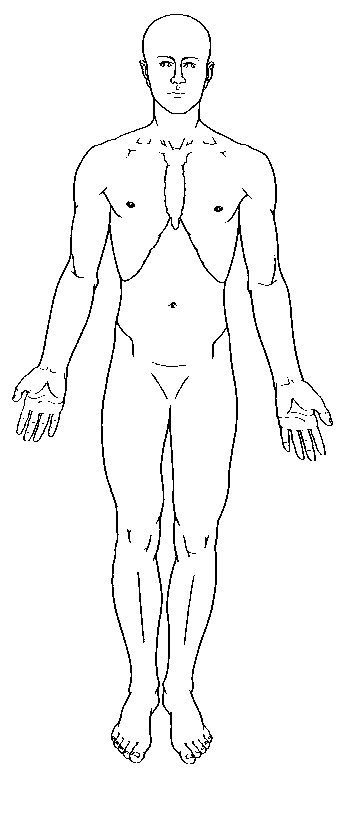
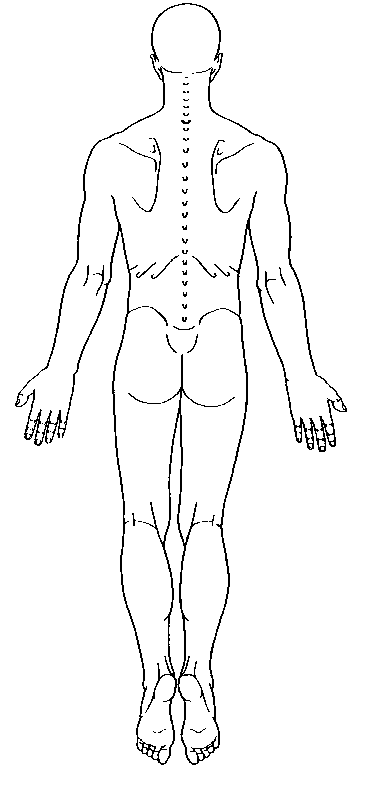
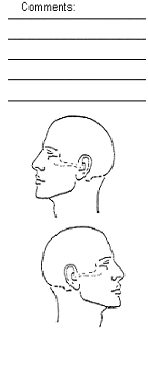
PLEASE MARK THE AREAS ON YOUR BODY WHERE YOU FEEL THE DESCRIBED
SENSATIONS: Use the following symbols. Marks areas of radiation. Include all affected areas.
Show main pain areas, use arrows to show spread.
PLEASE USE ANY OTHER MARKINGS FOR OTHER TYPES OF PAIN.
How often does your pain interfere: work
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
What makes your pain worse?
____ Pain is continuous & activities don't affect _____ Lying on stomach
____ Cough or sneeze _____ Certain positions or movements:
____ Straining or bowel movement ___________________________________
What eases or reduces your pain?
____ Clenching your teeth or making a fist _____ Manipulation (massage, chiropractic,etc)
PLEASE CHECK THE TYPE OF TREATMENTS YOU HAVE HAD AND THE RESULTS:
Treatment Who Provided Treatment?
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
Treatment Who Provided Treatment?
What do you believe is the cause of your pain? _________________________________________
______________________________________________________________________________
______________________________________________________________________________
What do you do to manage your pain?________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Please describe any episodes of pain which were extremely frightening or in which you lost control:
______________________________________________________________________________
H:\Data\Our Documents\Jim\painques.doc/jm
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
Have there been times when your pain was mild or gone? When? Please describe: ___________
______________________________________________________________________________
Is anyone in your family or friends able to help you with your pain? Who? ____________________
Describe how: ___________________________________________________________________
How likely is it that your pain can be removed or cured? (Circle one):
Do you have particular fears or concerns about the future? (e.g. becoming paralyzed, crippled,
needing further surgery, losing emotional control, being unable to support family, etc.) Please list: _
______________________________________________________________________________
______________________________________________________________________________
Any other treatments you would like to try? ____________________________________________
______________________________________________________________________________
____ Cigarettes, Pipe, Nicotine Chew (Number per day:_______________________)
____ Coffee, Tea, Cola or soda with Caffeine (Total number of cups per day:_______________)
____ Weight control medication . (Type and amount per day:____________________________)
____ Speed, Meth, Cocaine, Uppers, Cross-tops (Type & amount/day:______________________)
____ Downers, Barbs, Ludes, Tranqs (Type & amount/day:_______________________________)
Type and duration: _______________________________________________
PRIOR to your injury or pain, did you exercise?
Type and duration: _______________________________________________
H:\Data\Our Documents\Jim\painques.doc/jm
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
PLEASE CHECK ANY MEDICATIONS YOU TAKE OR HAVE USED PREVIOUSLY FOR PAIN, ETC:
Put a "+" by those that help, "0" by those that don't help, "--" by those that make it worse. Use Medication Medication Now Before Narcotics: Sleeping Aid: Anti-inflammatories: Antidepressants:
Celexa, Lexapro (Citalopram, Escitalopram)
H:\Data\Our Documents\Jim\painques.doc/jm
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
Medication Medication Now Before Anti-inflammatories: Antidepressants: Tranquilizers: Muscle Relaxers:
H:\Data\Our Documents\Jim\painques.doc/jm
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
Medication Medication Now Before Tranquilizers: Anti-Convulsants: Migraine Medications: Over the counter: Other medications for pain:
H:\Data\Our Documents\Jim\painques.doc/jm
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
Please List ALL Drugs You Are Currently Taking:
1._____________________________________________________________________________
2._____________________________________________________________________________
3._____________________________________________________________________________
4._____________________________________________________________________________
5._____________________________________________________________________________
6._____________________________________________________________________________
7._____________________________________________________________________________
8._____________________________________________________________________________
9._____________________________________________________________________________
10.____________________________________________________________________________
ALLERGIES: ___________________________________________________________________ MEDICAL HISTORY: (Please list approximate dates and where)
MEDICAL CONDITIONS OR SERIOUS ILLNESS: ______________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
SURGERIES: ___________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
INJURIES:______________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
OTHER HOSPITALIZATIONS: ______________________________________________________
______________________________________________________________________________
______________________________________________________________________________
WHEN WAS YOUR LAST COMPLETE MEDICAL EXAM? ________________________________
CHEST XRAY? ____________________________________________________________
PAP SMEAR (Women only)?__________________________________________________
MAMMOGRAM? ___________________________________________________________
PROSTATE EXAM (Men only)?________________________________________________
HIV test/Hepatitis screen? ____________________________________________________
H:\Data\Our Documents\Jim\painques.doc/jm
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
FAMILY HISTORY:
CHECK FOLLOWING IF ANY FAMILY MEMBERS ARE AFFECTED. PLEASE NOTE WHO IS
Mother's age ______________ Alive?__________ Father's age___________ Alive?_________
Spouse's/Partner's name, age and health _____________________________________________
SOCIAL HISTORY:
Single? _______ Married?_______ Partnered?_______ Divorced?_______ Widowed?______
Number of children ______________ Their ages and sex ________________________________
________________________________ Number of children still living with you________________
Current occupation:_______________________________________________________________
Full Time______ Part Time______ Hours/Wk______ Time Loss______ Compensation:$ ____
Grade completed in school_______ Degree & School ___________________________________
Previous work experience (briefly): ___________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Religious preference ______________________________________________________________
Religious background _____________________________________________________________
Service organizations _____________________________________________________________
H:\Data\Our Documents\Jim\painques.doc/jm
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
RECENT HEALTH STATUS:
CHECK ANY OF THE FOLLOWING THAT APPLY TO YOU IN THE PAST 3 TO 6 MONTHS.
Explanations or anything else important to your health ___________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
______________________________________________________________________________
Is there anything else you would like to tell the doctor today? ______________________________
______________________________________________________________________________
_______________________________________________________________________________
_______________________________________________________________________________
H:\Data\Our Documents\Jim\painques.doc/jm
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
Disability Questionnaire Are you applying for disability benefits or are you currently disabled? Yes ___ No___
If not, please skip to the signature line. Please indicate the amount of time you can do these activities by using the spaces provided.
Thank you for taking time to complete this form. Please return to the receptionist, or mail in to: Pain Management Partners, LLC Dr. J. Morris, 2401 River Rd. Suite 101, Eugene, OR 97404.
.Signature__________________________________________
H:\Data\Our Documents\Jim\painques.doc/jm
Arizona Glaucoma Specialists (www.azglaucomaspecialists.com) Tucson (520) 544-4393 Fax (520) 544-0098 Phoenix (480) 538-7075 Fax (480) 538-7952 Name:____________________________________ Date:___/___/____ Age/DOB:___________________________ Referred by:________________________________ Primary Care Physician:________________________________ Please fill out FRONT AND BACK of this page b
ARTICULO COMPLETO TRADUCIDO AL IDIOMA ESPAÑOL SETIEMBRE DE 2006 DISPERSION NOSOCOMIAL DE ENTEROCOCUS FAECIUM RESISTENTE A LA VANCOMICINA (ERV) Y AL LINEZOLID EN UN CENTRO MEDICO DE ALTA COMPLEJIDAD Thomas E. Dobbs, Mukesh Patel, Ken B. Waites, Stephen A. Moser, Alan M. Stamm, and Craig J. Hoesley Journal Of Clinical Microbiology, Set. 2006, p. 3368-3370. R
 Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
PLEASE MARK THE AREAS ON YOUR BODY WHERE YOU FEEL THE DESCRIBED
SENSATIONS: Use the following symbols. Marks areas of radiation. Include all affected areas.
Show main pain areas, use arrows to show spread.
PLEASE USE ANY OTHER MARKINGS FOR OTHER TYPES OF PAIN.
How often does your pain interfere: work
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
What makes your pain worse?
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
PLEASE MARK THE AREAS ON YOUR BODY WHERE YOU FEEL THE DESCRIBED
SENSATIONS: Use the following symbols. Marks areas of radiation. Include all affected areas.
Show main pain areas, use arrows to show spread.
PLEASE USE ANY OTHER MARKINGS FOR OTHER TYPES OF PAIN.
How often does your pain interfere: work
Pain Management Partners LLC- James R. Morris, MD
2401 River Rd. Suite 101 Eugene, OR 97404 (541) 344-8469 Fax 687-8631
What makes your pain worse?