Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Xeed™
A QUALITY PRODUCT WITH FULL THERAPEUTIC DOSE/DAY LEADING TO RELATIVELY SPEEDIER CURE FROM TB, LESSER CHANCES OF GETTING DRUG RESISTANT TB AND REDUCED RISK OF TREATMENT FAILURE XEED™ is a fixed dose combination (FDC) of four drugs Rifampicin, Ethambutol,
Pyrazinamide and Isoniazid with proven bioavailability of Rifampicin for the treatment of tuberculosis. It offers the convenience of a fixed dose combination, at the same time
ensuring optimal bioavailability of all the active drugs.
It ensures release of Rifampicin & Isoniazid at different sites to avoid interaction leading
to 42% enhanced bioavailability of Rifampicin as compared to conventional FDCs.
It is estimated that between 19% to 43% of the world population is infected with
tuberculosis. As per recent forecasts, between 2000 and 2020, nearly one billion people
will be newly infected, 200 million people will develop active tuberculosis, and 35
million will die from the disease - if control is not further strengthened. The HIV
epidemic has also increased the risk of tuberculosis
WHO & IUATLD recommend the use of FDCs to ensure the delivery of correct dosage
and avoidance of monotherapy, thereby, preventing the development of Multi Drug
However, it has been observed that the co-administration of Rifampicin with Isoniazid in
the form of FDC or in loose combination, leads to a significant loss of bioavailability of
XEED™ is a compression-coated tablet, wherein Isoniazid is present in the core and is
coated with special polymers for site-specific release and avoid the known adverse
interaction with Rifampicin. The outer layer of the tablet contains Rifampicin,
Ethambutol and Pyrazinamide. The tablets are further coated with selected polymers to
prevent the degradation of the active drugs due to exposure to light and m
Outer Coating to protect from light and moisture Rifampicin, Ethambutol, Pyrazinamide Outer Layer Specialized Polymer Coating for Site Specific Release Isoniazid core 3.1 Mechanism of action
The problem of bioavailability of Rifampicin has been solved by spatial control of release
of both the drugs in such a way that the release takes place at different locations in GIT.
The site-specific release of Rifampicin and Isoniazid prevents the drugs from coming in
contact with each other in solution stage in the acidic pH of gastric region, thereby,
preventing the degradation. XEED™’s innovative technology releases Rifampicin,
Ethambutol and Pyrazinamide in the stomach while the special polymer coating on the
Isoniazid core prevents its release in the stomach, thereby avoiding any interaction
between Isoniazid and Rifampicin. Rifampicin releases in acidic pH of stomach and gets
absorbed immediately which ensures absolute bioavailability of Rifampicin. The
Isoniazid core moves on to the proximal part of the intestine and the release of the drug
takes place in the duodenum where pH rises above 5.0. The release of two drugs at
different sites results in no loss of bioavailability of either of the drug.
4.1 Study I
The bioavailability of Rifampicin in XEED™ was compared to the reference
conventional preparation in a six volunteer pilot study. The Cmax and AUC
(bioavailability) of Rifampicin from the XEED™ were found to be significantly higher
from the formulation containing conventional Rifampicin.
4.2 Study II
In an another single blinded, randomized, two-way, cross-over bioequivalence study
carried out in 12 healthy volunteers, it was found that the Cmax and AUC (bioavailability)
of Rifampicin from the XEED ™ formulation was found to be higher when compared to
Cmax of Rifampicin from the reference conventional formulation. No difference in Cmax &
AUC (bioavailability) of Isoniazid was observed between the XEED ™ formulation and
Isoniazid of the reference conventional formulation.
4.3 Study III
Bioequivalence results from above pilot studies were strongly convincing and hence a
third BA/BE study was planned in 24 healthy volunteers. They were evaluated in a 3-way
crossover design for bioavailability of Rifampicin in the XEED ™ formulation against
conventional Rifampicin. It was reported that the XEED ™ had 42% higher relative
bioavailability of Rifampicin (with respect to AUC) than Rifampicin 450 mg (Rimactane)
C o nv . F D C T im e ( H rs )
Figure 1 : a relative bioavailability equal to 141.97% was observed for Rifampicin in case
of XEED™ when compared with reference conventional formulations (in loose
C o nv . F D C T im e ( hrs )
Figure 1 : There was no loss in bioavailability of Isoniazid as Cmax and AUCs are same
in both the cases, and as designed only Tmax has been delayed
4.4 Study IV
In order to evaluate the clinical significance of higher bioavailability of Rifampicin in the
XEED™, a randomized, open-labeled, comparative, prospective, multi-centric Phase IV
study involving 420 TB patients (Male - 78.3%, Female - 21.7%) with clinical
symptomatology of cough, fever, anorexia, haemoptysis, lethargy and weight loss was
planned. The aim was to evaluate the safety and efficacy of the XEED™ against
conventional FDC, in the treatment of primary pulmonary tuberculosis. All the patients
An early symptomatic relief in fever, cough (both productive and non-
productive), night sweats and haemoptysis was observed in patients with the
There was 91% improvement observed in the XEED™ group as compared to
70% in conventional FDC group, at the end of initiation phase (2 months) of
Also, at the end of continuation phase 99% of subjects taking the XEED™
showed improvement as compared to 84% taking conventional FDC.
At the end of IP At the end of CP Improved Deteriorate / Improved Deteriorate / Table 1 : Overall improvement in fever, cough, night sweats, haemoptysis in patients with XEED™ as compared to conventional FDC
There was a quicker radiological improvement seen in patients taking the
XEED™. Subjects in the XEED™ group showed early significant improvement in
all the defined markers of radiographs as compared to conventional group at day 45
Clinical study volunteers at one of the center of Phase IV study were also simultaneously
evaluated for Rifampicin and Isoniazid levels in the XEED™ and conventional FDC.
This was a parallel, non-cross over bioavailability study in 24 patients at the beginning of
their clinical therapy at first therapeutic dose. These patients were admitted for a day after
first dose of anti tubercular FDC and their blood levels were monitored for 12 hours
thereafter. Equal numbers of subjects were given XEED™ and conventional FDC. It was
observed that bioavailability of Rifampicin in XEED™ group was 20% higher as
compared to Rifampicin in conventional FDC. Further, no difference in Isoniazid Cmax
and bioavailability was observed. There was a significant delay in Tmax of Isoniazid in
Product patents are filed in all major countries across the globe and patent is already
Australia, Nigeria, North Korea, Poland, South Africa, Sudan, Tanzania, Turkey
CTD compilation under process for regulated markets
XEED™ 4 XEED™ 3E XEED™ 2
Step Therapy Criteria Step Therapy Group Drug Names Step Therapy Criteria If the patient has tried a Step 1 drug, then authorization for a Step 2 drug may be given. Step 1 Drug(s): Actos, Actoplus Met, Duetact, Januvia, Janumet, Kombiglyze, Onglyza. Step Therapy Group Drug Names Step Therapy Criteria If the patient has tried two Step 1 drugs, then authorization for
Tardive Dyskinesia is a side effect of antipsychotic medications. If an antipsychotic medication or Amoxapine is prescribed, this policy must be followed in combination with the "Psychotropic Medications Administration Policy”. Persons who receive the service of medication administration and/or monitoring of medications from Home and Community Options, Inc. shall be free from chemical restr



 C o nv . F D C
C o nv . F D C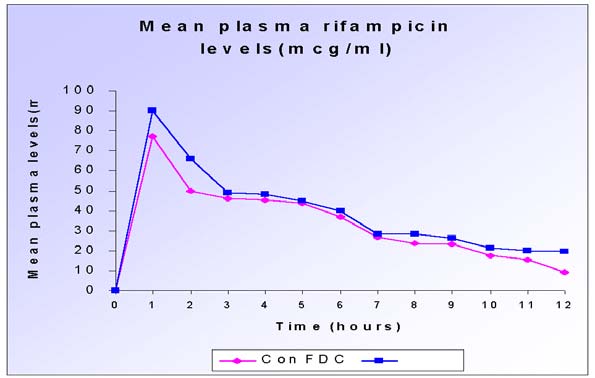 Clinical study volunteers at one of the center of Phase IV study were also simultaneously
evaluated for Rifampicin and Isoniazid levels in the XEED™ and conventional FDC.
This was a parallel, non-cross over bioavailability study in 24 patients at the beginning of
their clinical therapy at first therapeutic dose. These patients were admitted for a day after
first dose of anti tubercular FDC and their blood levels were monitored for 12 hours
thereafter. Equal numbers of subjects were given XEED™ and conventional FDC. It was
observed that bioavailability of Rifampicin in XEED™ group was 20% higher as
compared to Rifampicin in conventional FDC. Further, no difference in Isoniazid Cmax
and bioavailability was observed. There was a significant delay in Tmax of Isoniazid in
Product patents are filed in all major countries across the globe and patent is already
Clinical study volunteers at one of the center of Phase IV study were also simultaneously
evaluated for Rifampicin and Isoniazid levels in the XEED™ and conventional FDC.
This was a parallel, non-cross over bioavailability study in 24 patients at the beginning of
their clinical therapy at first therapeutic dose. These patients were admitted for a day after
first dose of anti tubercular FDC and their blood levels were monitored for 12 hours
thereafter. Equal numbers of subjects were given XEED™ and conventional FDC. It was
observed that bioavailability of Rifampicin in XEED™ group was 20% higher as
compared to Rifampicin in conventional FDC. Further, no difference in Isoniazid Cmax
and bioavailability was observed. There was a significant delay in Tmax of Isoniazid in
Product patents are filed in all major countries across the globe and patent is already

 Australia, Nigeria, North Korea, Poland, South Africa, Sudan, Tanzania, Turkey
CTD compilation under process for regulated markets
XEED™ 4
Australia, Nigeria, North Korea, Poland, South Africa, Sudan, Tanzania, Turkey
CTD compilation under process for regulated markets
XEED™ 4  XEED™ 2
XEED™ 2