Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Piediabeticoceped.com
E p i d e m i o l o g y / H e a l t h S e r v i c e s R e s e a r c h O R I G I N A L Many Americans Have Pre-Diabetes and Should Be Considered for Metformin ARY K. RHEE, MD K.M. VENKAT NARAYAN, MD
diabetes and then more rapidly to diabetes. IRSTEN HERRICK, MSC PAUL KOLM, PHD AVID C. ZIEMER, MD ENNIFER G. TWOMBLY, MD, PHD
studies, ϳ25–40% of individuals with pre-
IOLA VACCARINO, MD, PHD AWRENCE S. PHILLIPS, MD
diabetes go on to develop diabetes over 3– 8
ILLIAM S. WEINTRAUB, MD
years (4 – 6), and there is evidence of com-plications in 50% of patients at the time ofdiagnosis of diabetes (7). OBJECTIVE — To determine the proportion of the American population who would merit
metformin treatment, according to recent American Diabetes Association (ADA) consensus panel
recommendations to prevent or delay the development of diabetes.
lifestyle change and/or medication (4 – 6),the American Diabetes Association (ADA)
RESEARCH DESIGN AND METHODS — Risk factors were evaluated in 1,581 Screen-
ing for Impaired Glucose Tolerance (SIGT), 2,014 Third National Health and Nutrition Exam-ination Survey (NHANES III), and 1,111 National Health and Nutrition Examination Survey
2005–2006 (NHANES 2005–2006) subjects, who were non-Hispanic white and black, without
known diabetes. Criteria for consideration of metformin included the presence of both impaired
fasting glucose (IFG) and impaired glucose tolerance (IGT), with Ն1 additional diabetes risk
factor: age Ͻ60 years, BMI Ն35 kg/m2, family history of diabetes, elevated triglycerides, reduced
HDL cholesterol, hypertension, or A1C Ͼ6.0%.
years, BMI Ն35 kg/m2, family history ofdiabetes in first-degree relative, elevated
RESULTS — Isolated IFG, isolated IGT, and IFG and IGT were found in 18.0, 7.2, and 8.2%
of SIGT; 22.3, 6.4, and 9.4% of NHANES III; and 21.8, 5.0, and 9.0% of NHANES 2005–2006
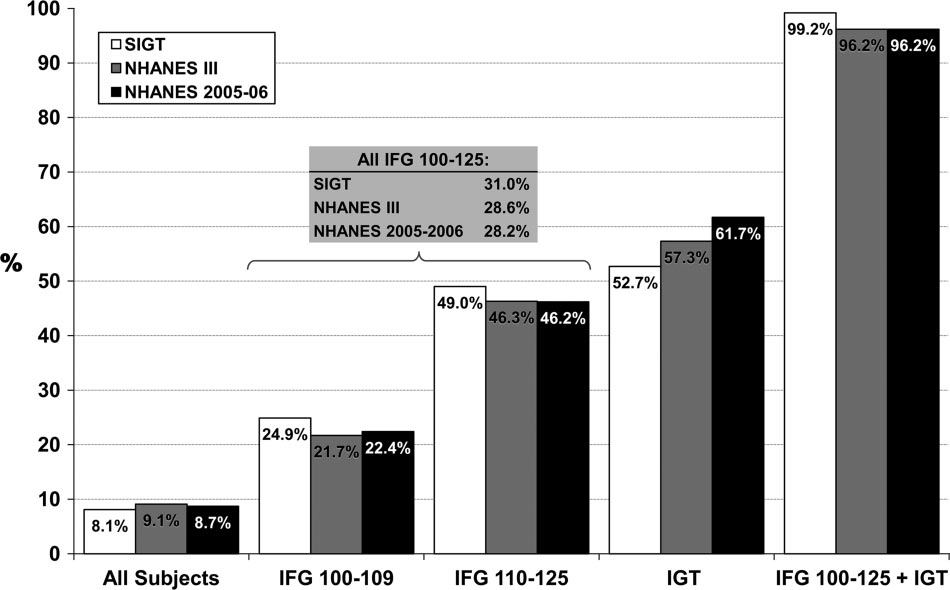
subjects, respectively. In SIGT, NHANES III, and NHANES 2005–2006, criteria for metformin
consideration were met in 99, 96, and 96% of those with IFG and IGT; 31, 29, and 28% of allthose with IFG; and 53, 57, and 62% of all those with IGT (8.1, 9.1, and 8.7% of all subjects),
CONCLUSIONS — More than 96% of individuals with both IFG and IGT are likely to meet
ADA consensus criteria for consideration of metformin. Because Ͼ28% of all those with IFG met
the criteria, providers should perform oral glucose tolerance tests to find concomitant IGT in all
patients with IFG. To the extent that our findings are representative of the U.S. population, ϳ1
in 12 adults has a combination of pre-diabetes and risk factors that may justify consideration of
metformin treatment for diabetes prevention.
teers without known diabetes who werescreened for diabetes/pre-diabetes by the
Diabetes Care 33:49–54, 2010
75-g oral glucose tolerance test (OGTT). Diabetesisapublichealthepidemic havepre-diabetes:impairedfastingglu- RESEARCHDESIGNAND
cose (IFG) and/or impaired glucose toler-
METHODS — I n c r o s s - s e c t i o n a l
rently, an estimated 38 million Americans
w h i c h t i m e g l u c o s e m e t a b o l i s m
● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ● ●
From the 1Department of Medicine, Division of Endocrinology, Metabolism, and Lipids, Emory University
to change in lifestyle. Criteria for con-
School of Medicine, Atlanta, Georgia; the 2Nutrition and Health Sciences Program, Graduate Division of
Biological and Biomedical Sciences, Emory University, Atlanta, Georgia; the 3Department of Medicine,
Division of Cardiology, Emory Program in Cardiovascular Outcomes Research and Epidemiology, At-lanta, Georgia; the 4Christiana Care Health System, Newark, Delaware; the 5Hubert Department of Global
additional diabetes risk factor: age Ͻ60
Health, Rollins School of Public Health, Emory University, Atlanta, Georgia; the 6Department of Medi-
cine, Emory University School of Medicine, Atlanta, Georgia; and the 7Atlanta VA Medical Center,
Corresponding author: Mary K. Rhee, mrhee@emory.edu. Received 3 March 2009 and accepted 21 September 2009. Published ahead of print at http://care.
diabetesjournals.org on 6 October 2009. DOI: 10.2337/dc09-0341.
2010 by the American Diabetes Association. Readers may use this article as long as the work is properly
cited, the use is educational and not for profit, and the work is not altered. See http://creativecommons.
participate in the Screening for Impaired
org/licenses/by-nc-nd/3.0/ for details. The costs of publication of this article were defrayed in part by the payment of page charges. This article must therefore be herebymarked “advertisement” in accordance with 18 U.S.C. Section 1734 solely to indicate this fact.
DIABETES CARE, VOLUME 33, NUMBER 1, JANUARY 2010
Metformin indicated in many pre-diabetic patients
by the Emory Institutional Review Board.
The invitation to participate was extended
after ingestion of the glucose load. For our
well as to members of the community.
Criteria for eligibility were age Ն18 years,
and had a survey weight value Ͼ0 (n ϭ
prior diagnosis of diabetes, not pregnant
or breast-feeding, not taking glucocorti-
Ն126 mg/dl or 2-h postchallenge glucose and A1C were categorized using the cut-
Ն200 mg/dl. Isolated IFG was further offs recommended by the ADA: age Ͻ60
first visits (selected largely on the basis of
(8). Other risk factors for diabetes that
need to balance participant sex and race),
begun before 11:00 A.M. after an overnight
line, 1 h, and 2 h. Blood samples were also
Hospital and Grady Memorial Hospital.
part in the Third National Health and Nu-
within 30 min. All samples were stored at
Ϫ80°C until assayed. Chemical analyses number of subjects in NHANES III and
were performed in the central clinical lab-
the diabetes status of one or more first-
left blank (NHANES III, n ϭ 1,163;
Statistics of the Centers for Disease Con-
NHANES 2005–2006, n ϭ 116), relatives
trol and Prevention that include both in-
nationally representative sample to assess
the health and nutritional status of adults
for the analysis of the SIGT study group.
In addition, subjects with missing values
11:00 A.M. after an overnight fast of at least
load, and had a survey weight value Ͼ0.
Among this subset (n ϭ 2,833), we in-
by self-report and included family history
of diabetes in a first-degree relative, race,
history of hypertension, history of diabe-
study population) (n ϭ 2,057).
seen in the morning session were asked to
sured using digital scales with subjects in
overnight for at least 9 h, reported no use
jects had been seated quietly for 5 min.
of oral medications or insulin for diabetes,
philia, and did not receive cancer chemo-
therapy in the previous 3 weeks. All blood
DIABETES CARE, VOLUME 33, NUMBER 1, JANUARY 2010
Rhee and Associates Table 1—Characteristics of study subjects
of elevated triglycerides and A1C levels(Table 2). Even with the differences in theprevalence of risk factors, almost all sub-
2005–2006) and those with IGT (isolated
IFG (isolated or with IGT), one-quarter to
NHANES III, and 28% in NHANES2005–2006) met the recommended crite-
to account for the complex survey design,
had diabetes, similar to the proportions in
ternational, Research Triangle Park, NC). RESULTS — Among 1,581 volunteers
NHANES 2005–2006) did so (Fig. 1).
populations met the criteria for consider-
NHANES III population (n ϭ 2,014), the
CONCLUSIONS — In consideration
(n ϭ 1,111), the average age was 46 years
diabetes, as specified by the ADA consen-
presence of each risk factor was generally
high risk of developing diabetes, defined
Table 2—Prevalence of risk factors for diabetes in study subjects
Data are %. Glucose tolerance categories: IFG (ϮIGT), IFG with or without IGT; IGT (ϮIFG), IGT with or without IFG; IFG ϩ IGT, both IFG and IGT. *ReducedHDL cholesterol defined as Յ40 mg/dl in men and Յ50 mg/dl in women. †Hypertension defined by any of the following: history of hypertension, systolic bloodpressure Ն130 mmHg, or diastolic blood pressure Ն85 mmHg. ‡Metformin indicated per the ADA consensus statement (8) criteria of the presence of both IFG andIGT and one of the following diabetes risk factors: age Ͻ60 years, BMI Ն35 kg/m2, family history of diabetes, elevated triglycerides, reduced HDL cholesterol, andA1C Ͼ6.0%. Risk factors for diabetes that were not specifically defined by the ADA were categorized according to the AHA/NHLBI diagnostic criteria for metabolicsyndrome (12): presence of hypertension by history, systolic blood pressure Ͼ130 mmHg or diastolic blood pressure Ͼ85 mmHg, triglyceride level Ն150 mg/dl,and HDL cholesterol Ͻ40 mg/dl in men and Ͻ50 mg/dl in women.
DIABETES CARE, VOLUME 33, NUMBER 1, JANUARY 2010
Metformin indicated in many pre-diabetic patients
Figure 1—Prevalence of metformin indication, stratified by glucose tolerance category. Metformin is indicated per the ADA consensus statementcriteria of the presence of both IFG and IGT and one of the following diabetes risk factors: age Ͻ60 years, BMI Ն35 kg/m2, family history of diabetes,elevated triglycerides, reduced HDL cholesterol, and A1C Ͼ6.0% (8). Risk factors for diabetes that were not specifically defined by the ADA werecategorized according to the AHA/NHLBI diagnostic criteria for metabolic syndrome (12): presence of hypertension by history, systolic bloodpressure Ͼ130 mmHg or diastolic blood pressure Ͼ85 mmHg, triglyceride level Ն150 mg/dl, and HDL cholesterol Ͻ40 mg/dl in men and Ͻ50 mg/dlin women. Glucose tolerance categories are as follows: IFG 100 –109, FPG levels 100 –109 mg/dl and 2-h postchallenge plasma glucose Ͻ140 mg/dl;IFG 110 –125, FPG 110 –125 mg/dl and 2-h postchallenge plasma glucose Ͻ140 mg/dl; all IFG, isolated IFG (FPG 100 –125 mg/dl and 2-hpostchallenge plasma glucose Ͻ140 mg/dl); IGT, isolated IGT; and IFG 100 –125 ϩ IGT, all IFG and IGT.
(both IFG and IGT as well as an additional
and preventive treatment of the disease.
risk factor) (8). To determine the propor-
Diabetes is currently the leading cause of
identify preventive treatment. In addition
tion of individuals who would be targeted
blindness, end-stage renal disease requir-
to lifestyle modification, pharmacological
treatment with acarbose (5), rosiglitazone
tions in the U.S. and increases the risk for
cardiovascular disease and stroke by two-
the onset of diabetes in individuals with
pre-diabetes. The relative risk reduction
billion in both direct and indirect health
IFG, nearly one-third of subjects met the
treated with acarbose (5), 52– 62% over
prevalence of diabetes has been on the rise
2– 4 years with orlistat (19), 62% over 3
years with rosiglitazone (6), and 26 –31%
cating that the epidemic is likely to con-
over 2.5–2.8 years with metformin (4).
statement, more than one-half of all of the
subjects with IGT qualified, and almost all
of those with both IFG and IGT qualified.
benefit of preventive treatment must out-
Overall, 8 –9% met the recommended cri-
risk for the development of diabetes, such
weigh any associated side effects or addi-
teria. Assuming that our data are general-
that 25–39% of patients with IFG or IGT
tional risks, particularly because none of
go on to develop diabetes over a period of
dication of diabetes prevention. Gastroin-
cardiovascular disease (16,17) and micro-
associated with acarbose (5) and orlistat
(19), leading to poor patient compliance,
with diabetes (18). Given these risks, pro-
DIABETES CARE, VOLUME 33, NUMBER 1, JANUARY 2010
Rhee and Associates References
(21), and heart failure (22) are associated
from university and health care settings,
1. Centers for Disease Control and Preven-
with rosiglitazone. Therefore, metformin,
they may also follow healthier lifestyles,
tion. National Diabetes Fact Sheet: General
which has been used for many years and is
which could offset such a bias. Moreover,
Information and National Estimates on Dia-betes in the United States, 2007. Atlanta,
tively safe, has become the leading candi-
ment of pre-diabetes (23). Similar to the
Geiss LS. Full accounting of diabetes and
call for primary prevention of diabetes in
treatment, beginning with lifestyle modi-
formin in addition to lifestyle changes. To
the extent that our findings are represen-
tative of the U.S. population, close to 1 in
vides a looser set of criteria regarding the
initiation of pharmacological treatment.
incidence of type 2 diabetes with lifestyle
tion or delay. Notably, eligibility for met-
5. Chiasson JL, Josse RG, Gomis R, Hanefeld
those with IFG, IGT, and/or the metabolic
for prevention of type 2 diabetes mellitus:
vascular disease, nonalcoholic fatty liver
IGT had at least one risk factor. Therefore,
disease, a history of gestational diabetes,
6. Gerstein HC, Yusuf S, Bosch J, Pogue J,
has been established, the presence of ad-
into account the target populations as de-
ditional risk factors could almost be as-
logical treatment to prevent or delay de-
rosiglitazone Medication) trial. Effect of
nearly one-third of all subjects with IFG
rosiglitazone on the frequency of diabetes
met the criteria for metformin treatment,
patients with IFG to test for the presence
stantial costs: at current generic rates for
7. UK Prospective Diabetes Study (UKPDS).
consideration of metformin treatment.
billion per year. However, several studies
suggest that diabetes prevention or delay
Heine RJ, Henry RR, Pratley R, Zinman B. Acknowledgments — This work was sup-
ported in part by grants DK-070715 and RR-
effective and/or cost-saving (24); further
glucose tolerance: implications for care.
evaluation using a variety of cost analysis
066204 (to L.S.P., W.S.W., P.K., and V.V.),
VA HSR&D SHP 08-144 and IIR 07-138 (to
finitive conclusion regarding the cost of
the first evaluation of the proportion of
No potential conflicts of interest relevant to
10. Centers for Disease Control and Preven-
Parts of this study were presented in ab-
prevention or delay of development of di-
stract form at the 68th Scientific Sessions of
Statistics (NCHS). National Health and
the American Diabetes Association, San Fran-
Nutrition Examination Survey Data. Third
cisco, California, 6 –10 June 2008. National Health and Nutrition ExaminationSurvey, 1988 –1994, NHANES III. Hyatts-
recruited on a volunteer basis, there may
combe, Rincy Varughese, Eileen Osinski, Jade
Irving, Amy Barrera, Lennisha Pinckney, Jane
risk factors for diabetes. Therefore, the
Caudle, and Circe Tsui. We also appreciate the
support of the Emory General Clinical Re-
of individuals at higher risk. However, be-
11. Centers for Disease Control and Preven-
DIABETES CARE, VOLUME 33, NUMBER 1, JANUARY 2010
Metformin indicated in many pre-diabetic patients
type 2 diabetes in the Baltimore Longitu-
20. Grey A. Skeletal consequences of thiazo-
Statistics (NCHS). National Health and
lidinedione therapy. Osteoporos Int 2008;
Nutrition Examination Survey Data. Con-tinuous National Health and Nutrition Ex-
16. Norhammar A, Tenerz A, Nilsson G, Ham-
21. Hollenberg NK. Considerations for man-
amination Survey, NHANES 2005–2006.
sten A, Efendíc S, Ryde´n L, Malmberg K.
Glucose metabolism in patients with acute
myocardial infarction and no previous diag-
nosis of diabetes mellitus: a prospective
tive heart failure and cardiovascular death
nhanes/nhanes2005–2006/nhanes05_06.
diabetes given thiazolidinediones: a meta-
12. Grundy SM, Cleeman JI, Daniels SR, Do-
analysis of randomised clinical trials. Lan-
betes Association diagnostic criteria: col-
23. American College of Endocrinology Task
Spertus JA, Costa F. Diagnosis and manage-
laborative analysis of diagnostic criteria in
Force on Pre-Diabetes. American College ofEndocrinology Consensus Statement on the
18. Barr EL, Wong TY, Tapp RJ, Harper CA,
Diagnosis and Management of Pre-Diabetes
Lung, and Blood Institute Scientific State-
in the Continuum of Hyperglycemia—When
eral neuropathy associated with retinopa-
Do the Risks of Diabetes Begin? Washing-
13. Pinhas-Hamiel O, Zeitler P. The global
spread of type 2 diabetes mellitus in chil-
impaired glucose metabolism? The 1999 –
dren and adolescents. J Pediatr 2005;146:
14. Warram JH, Sigal RJ, Martin BC, Krolewski
19. Torgerson JS, Hauptman J, Boldrin MN,
AS, Soeldner JS. Natural history of impaired
Sjo¨stro¨m L. XENical in the prevention of
glucose tolerance: follow-up at Joslin Clinic.
study: a randomized study of orlistat as an
15. Meigs JB, Muller DC, Nathan DM, Blake
adjunct to lifestyle changes for the pre-
preventing type 2 diabetes in adults with
DR, Andres R. The natural history of pro-
gression from normal glucose tolerance to
DIABETES CARE, VOLUME 33, NUMBER 1, JANUARY 2010
ATTENTION DEFICIT After completing this educational activity, HYPERACTIVITY DISORDER { Discuss the occurrence and distribution of ADHD from childhood through adulthood. { Outline the current understanding of the causes of { Discuss the impact of ADHD symptoms on function. { Discuss teaching-related practices that have been found to be useful with students with ADH
Jødedom Rabbiner prof. dr. Walter Homolka Grunnleggende forståelse Den eldste av de tre monoteistiske religionene har en historie som strekker seg flere tusen år tilbake. Det har aldri eksistert én jødedom, like lite som dagens jødiske religion kan karakteriseres som én jødedom. Den jødiske religionen kjennetegnes snarere av at den gjennom alle tider har avspeilet et mer eller mind
 Metformin indicated in many pre-diabetic patients
Metformin indicated in many pre-diabetic patients