Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Mcpmartin
ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
Improvement in Fibromyalgia Symptoms With Acupuncture: Results of a Randomized Controlled Trial
DAVID P. MARTIN, MD, PHD; CHRISTOPHER D. SLETTEN, PHD; BRENT A. WILLIAMS, MS;
OBJECTIVE: To test the hypothesis that acupuncture improves
conditions. More than 90% of patients with fibromyalgia
have tried complementary techniques, including dietary
PATIENTS AND METHODS: We conducted a prospective, partially
and herbal supplements, indicating their openness to
blinded, controlled, randomized clinical trial of patients receivingtrue acupuncture compared with a control group of patients who
complementary medicine and/or inadequate response to
received simulated acupuncture. All patients met American Col-
allopathic therapies.3 The National Institutes of Health has
lege of Rheumatology criteria for fibromyalgia and had tried con-
issued a consensus statement that concludes that acupunc-
servative symptomatic treatments other than acupuncture. Wemeasured symptoms with the Fibromyalgia Impact Questionnaire
ture may be of adjunctive help in the treatment of
(FIQ) and the Multidimensional Pain Inventory at baseline, imme-
fibromyalgia, although a lack of controlled studies weak-
diately after treatment, and at 1 month and 7 months after
treatment. The trial was conducted from May 28, 2002, to August18, 2003.
Of the many trials of acupuncture for fibromyalgia, only
2 were randomized and controlled.5 The first, by Deluze et
RESULTS: Fifty patients participated in the study: 25 in the acu-puncture group and 25 in the control group. Total fibromyalgia
al,6 concluded that acupuncture was effective therapy. The
symptoms, as measured by the FIQ, were significantly improved in
second, more recent study by Assefi et al7 concluded that
the acupuncture group compared with the control group during
acupuncture was not effective for fibromyalgia. Hence,
the study period (P=.01). The largest difference in mean FIQ totalscores was observed at 1 month (42.2 vs 34.8 in the control and
further research is required to define the possible role of
acupuncture groups, respectively; P=.007). Fatigue and anxiety
acupuncture in the treatment of fibromyalgia.
were the most significantly improved symptoms during the follow-
The current study was designed to test the hypothesis
up period. However, activity and physical function levels did notchange. Acupuncture was well tolerated, with minimal adverse
that acupuncture improves symptoms of fibromyalgia
with validated syndrome-specific measurement tools
CONCLUSION: This study paradigm allows for controlled and
and long-term follow-up. Also, we sought to test the
blinded clinical trials of acupuncture. We found that acupuncture
feasibility of conducting prospective, randomized studies
significantly improved symptoms of fibromyalgia. Symptomatic
of acupuncture with a control group exposed to simulated
improvement was not restricted to pain relief and was mostsignificant for fatigue and anxiety.
FIQ = Fibromyalgia Impact Questionnaire; MPI = Multidimensional PainInventory
The protocol was approved by the Mayo Foundation Insti-tutional Review Board, and written consent was obtainedfrom all participants before treatment. Our study popula-
Fibromyalgia is characterized by chronic widespread tion was recruited from patients who were referred to the
musculoskeletal pain and associated symptoms, such
Mayo Fibromyalgia Treatment Program in Rochester,
as fatigue, joint stiffness, and sleep disturbance.1 The disor-
Minn, by their physician, usually after a trial of conserva-
der is thought to represent an alteration in pain threshold or
tive management. This program includes confirmation of
sensory processing at the level of the spinal cord or highercortical levels. No cure is known, and available treatments
From the Department of Anesthesiology (D.P.M., I.H.B.) and Department of
are only partially effective. Fibromyalgia affects 2% of the
Health Sciences Research (B.A.W.), Mayo Clinic College of Medicine, Roches-ter, Minn; and Division of Psychology and Department of Pain Medicine, Mayo
general population: 3.4% women and 0.5% men.2 The
Clinic College of Medicine, Jacksonville, Fla (C.D.S.). Dr Berger is now with the
prevalence of women with the condition increases with age
Medical College of Georgia, Augusta.
and is greater than 7% in women older than 60 years.
This work was supported by Mayo Foundation and the Mayo Anesthesia
Fibromyalgia is also perceived by many to be a disabling
Clinical Research Unit. Dr Martin is supported in part by a Research StarterGrant from the Foundation for Anesthesia Education and Research.
condition. Although it is not a progressive or degenerative
Address reprint requests and correspondence to David P. Martin, MD, PhD,
disease process, it can severely affect quality of life.
Department of Anesthesiology, Mayo Clinic College of Medicine, 200 First St
Acupuncture is a complementary medical technique
SW, Rochester, MN 55905 (e-mail: martin.david@mayo.edu).
used for the treatment of painful disorders, among other
2006 Mayo Foundation for Medical Education and Research Mayo Clin Proc. • June 2006;81(6):749-757 • www.mayoclinicproceedings.com
For personal use. Mass reproduce only with permission from Mayo Clinic Pr
ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
the diagnosis of fibromyalgia by a rheumatologist and 1.5
issues and not all participants had significant others. The
days of education, counseling, and group discussion about
MPI has proven reliability and validity for both chronic
symptom management. At the conclusion of this program,
patients were given an additional informational presenta-
Patients were required to wait at least 4 weeks after
tion about the current study and were invited to participate.
completing the Fibromyalgia Treatment Program before
To determine the sample size, we estimated that acupunc-
beginning study treatments. We conducted FIQ and MPI
ture would yield at least a 2-point reduction in the
measurements at baseline before treatment began, immedi-
Fibromyalgia Impact Questionnaire (FIQ). On the basis of
ately after completion of all treatments, and 1 month and 7
previous studies using the FIQ, 25 patients were required in
months after completion of treatment.
each group. The trial was conducted from May 28, 2002, toAugust 18, 2003.
Patients were excluded if they had prior experience with
After a 4-week period to adopt principles learned in the
acupuncture or a bleeding diathesis. They were required to
Fibromyalgia Treatment Program, patients completed
have sufficient cognitive ability to read the consent form
baseline FIQ and MPI measurements. Patients were ran-
and to complete the survey instruments. Patients had to be
domized immediately before the first treatment session to
within a geographic range that allowed for participation in
either the acupuncture or control group. Randomization
6 treatment sessions during a 2- to 3-week period. No
was done in blocks of 4 to prevent imbalances in treatment
monetary compensation was provided, but parking ex-
allocation. There was no crossover between groups, and
patients were scheduled to avoid any overlap during whichthey could compare experiences. Patients received treat-
ments every 2 to 4 days during 2 to 3 weeks for a total of 6
The FIQ is a standardized and validated tool that is com-
sessions. All treatments were performed at 1 facility by 2
monly used in fibromyalgia research.8 The FIQ is a 20-item
questionnaire used to assess the current health status ofpatients with fibromyalgia. Specifically, it evaluates physi-
cal functioning, work status, depression, anxiety, sleep,
Patients in the acupuncture group were positioned in the
pain, stiffness, fatigue, and well-being, each on a 0- to 10-
sitting position with a screen placed so that they could not
point scale. Individual item scores, not including the scores
observe placement of the treatments yet were allowed eye
that deal with work status, are combined into a total fibro-
contact with the acupuncturist (Figure 1). Acupuncture
myalgia impact score that ranges from 0 to 80. Higher
points were standardized for all patients and not modified
scores indicate a patient is more adversely affected by
for the specific symptoms of the patient. We picked strong
fibromyalgia. The FIQ has proven construct validity, test-
regulatory points that commonly recur in the acupuncture
retest reliability, and content relevance and is a widely
literature. Specifically, we used bilateral points at large
recommended tool to use in fibromyalgia research.8
intestine 4, stomach 36, liver 2, spleen 6, pericardium 6,
We also used the Multidisciplinary Pain Inventory
and heart 7. We also used axial paramedian points along the
(MPI), a more generalized measure of chronic pain and its
bladder meridian at the cervical spine during the first 3
impact.9 The MPI is a 61-item questionnaire developed to
sessions and at the lumbar spine during the last 3 sessions.
evaluate patients with chronic pain. It is composed of 13
Figure 2 illustrates the acupuncture points, totaling 18
scales that measure different pain-related aspects of pa-
needles during the first 3 sessions and 20 needles during the
tients’ lives. Five of these scales were chosen as useful
outcome measures for this study: pain severity, interfer-
At each point, the skin was wiped with alcohol, and an
ence (patients’ perceptions about how pain interferes with
adhesive bandage was placed over the point. The needle
their daily lives), life control (patients’ perceptions about
was inserted through the bandage to the acupuncture point.
control over pain and life events), affective distress (mood,
The sensation of de Qi or “needle grab” was not specifi-
irritability, tension), and general activity level (composite
cally elicited. Electrical stimulation was applied at 2 Hz
activity score based on 4 other MPI scales that were not
between large intestine 4 and stomach 36, bilaterally, and at
used: household chores, outdoor work, activities away
10 Hz over the axial circuits. All stimulator wires were
from home, and social activities). The 5 scales represent
taped to skin to avoid moving the needles. The pulse gen-
areas that the Mayo Fibromyalgia Treatment Program at-
erator (IC-1107+, ITO Co Ltd, Tokyo, Japan) produced
tempts to improve. The 4 other scales not used involved
short, bipolar current spikes at an amplitude typically toler-
support from a spouse or significant other. We excluded
able to most patients. Patients were asked, “Is the stimula-
these scales because our program does not address these
tion uncomfortable?” If it was uncomfortable, the current
Mayo Clin Proc. • June 2006;81(6):749-757 • www.mayoclinicproceedings.com
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
was reduced appropriately. After placement of all needlesand initiation of electrical stimulation, patients were al-lowed to rest quietly in a darkened room while relaxingmusic played in the background for 20 minutes.
CONTROL GROUPPatients in the control group were positioned identically topatients in the acupuncture group so that they could notobserve the treatments. Identical points were used. Eachpoint was wiped with alcohol, the skin was indented with adull surgical instrument, and a small circular adhesive ban-dage was applied that had previously been rigged with anacupuncture needle such that the needle handle stuck out ofthe bandage but did not pierce the skin. Instead, the needlewas bent to form a tripod so that it was supported on theskin surface and appeared as if it were anchored within theskin. Patients in the control group felt the wipe with alco-hol, a mild pricking sensation, and placement of an adhe-sive bandage (Figure 3). All the while they were not able tosee the procedure.
Electrical stimulation was applied to the same points as
the acupuncture group. Even though the lights flashed onthe pulse generator, the resistance of the skin prevented anyperceptible current flow. Just as in the acupuncture group,patients were asked, “Is the stimulation uncomfortable?”After placement of the placebo treatment, patients relaxedfor 20 minutes in a darkened room while quiet musicplayed in the background. Once the treatment was com-pleted, both the acupuncture and control groups looked thesame. In preliminary trials, volunteers could not tell the
FIGURE 1. Experimental setup. Patients were seated with a tray and
difference between the 2 procedures.
blanket placed as a headrest such that their view of the treatmentwas obscured. Both acupuncture and control treatments looked
identical. Some acupuncture needles were attached to an electricalstimulator, whereas others were not. For clarity, not all acupuncture
Conversation was controlled and neutral in both groups.
points are shown in this illustration.
During placement of the treatment, neutral conversationwas used (family, sports, the weather, and so on). Anyreference to specific treatment or symptoms was de-
plete all 6 sessions, they still remained in their respective
flected or referred to the blinded study coordinator. At the
groups for follow-up measurements of pain and quality of
end of the treatments, all materials were removed from
life. Data were analyzed based on the intention-to-treat
the room so patients could not observe the needles or
Figure 4 shows the sequence of events for each patient
in the study. Patients were enrolled after they completed
the Fibromyalgia Treatment Program. Randomization oc-
On completion of the treatment sessions, patients filled
curred at least 4 weeks later, when the baseline assess-
out 3 additional FIQ and MPI surveys. This was done by
ment was made. Then patients received 6 treatments for 2
mail at the end of the treatments and at 1 month and 7
to 3 weeks. Assessments were made immediately after
months after the end of the treatments. All evaluations
completion of the treatments and at 1 month and 7 months
were obtained by the study coordinator, who was blinded
to the group assignment. If patients had concerns about
The primary end point was the FIQ total score, mea-
adverse effects or needed to consult with a physician for
sured as the sum of the 8 FIQ subscales (each on a 0- to 10-
any other reason, they were referred to a clinician not
point scale). The primary analysis involved comparing the
associated with the study. If patients were unable to com-
FIQ total score between the acupuncture and control group
Mayo Clin Proc. • June 2006;81(6):749-757 • www.mayoclinicproceedings.com
For personal use. Mass reproduce only with permission from Mayo Clinic Pr
ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
ing treatment effects at individual time points usinganalysis of covariance complemented this analysis. Sec-ondary analyses involved analyzing the FIQ and MPIsubscales individually using similar techniques as de-scribed herein.
Figure 5 illustrates patient enrollment and allotment tostudy groups. Sixty patients were enrolled in the study oncompletion of the Fibromyalgia Treatment Program. Tenof these patients withdrew from the study during the 4-week period of stabilization before treatments started andbefore randomization. Eight of those patients had difficultyin scheduling the 6 treatment sessions. One patient hadreceived acupuncture in the past but had forgotten thisduring the initial screening process. The final patientelected to withdraw because of apprehension about needlesand a history of vasovagal syncope. Therefore, 50 patients
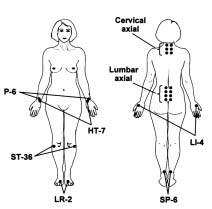
FIGURE 2. Acupuncture points. Needles were placed at the large
completed the baseline assessment and were randomly al-
intestine 4 (LI-4), stomach 36 (ST-36), liver 2 (LR-2), spleen 6 (SP-6), pericardium 6 (P-6), and heart 7 (HT-7). Electrical stimulation
located to the acupuncture and control groups. There were
was provided between LI-4 and ST-36 at 2 Hz. Axial points were
no significant differences between the groups with respect
placed along the bladder meridian and stimulated at 10 Hz. The
to age, sex, or race. All patients were women except for 1
cervical axial circuit was used only during the first 3 sessions, andthe lumbar axial circuit was used only during the last 3 sessions.
(in the control group), even though the study was equallyopen to both men and women. All patients were white
over time using a repeated-measures analysis of variance
except for 1 (in the acupuncture group), reflecting the racial
model. An overall treatment effect was estimated after
composition of the geographic area where the study was
adjusting for time and baseline FIQ total score. Examin-
conducted. The mean ± SD age of the patients was
FIGURE 3. Comparison of acupuncture and control needle configurations. In the acupuncturegroup, the skin is wiped with alcohol, a sterile bandage is applied, and the needle is insertedthrough the bandage to the acupuncture point. In the control group, the skin is wiped withalcohol, the skin is briefly “poked” but not cut, and then a bandage is affixed that contains amodified acupuncture needle that looks identical to the acupuncture treatment. Mayo Clin Proc. • June 2006;81(6):749-757 • www.mayoclinicproceedings.com
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
FIGURE 4. Timeline for each patient. At least 4 weeks elapsed between enrollment and baselineassessment. Patients were then randomized to receive 6 acupuncture or 6 control treatments duringa 2- to 3-week period. Assessments (indicated by asterisks) were made at baseline, treatmentcompletion (0 months), and 1 and 7 months after treatment.
51.7±14.1 years for the control group and 47.9±11.2 years
group did not complete any questionnaires after conclu-
for the acupuncture group (P=.30).
sion of the treatment sessions and was considered lost to
All patients completed at least 5 treatment sessions.
Two patients in the acupuncture group and 1 in the control
The treatments were tolerated well by the patients, and
group were not able to complete the last session because
most reported enjoying the experience. Many of the patients
of scheduling conflicts. They remained in their respective
in both groups reported feeling tired and/or relaxed after the
groups for data collection and analysis, as required by the
treatments. Mild bruising and soreness were more common
intention-to-treat principle. The number of questionnaires
in the acupuncture group. Two patients experienced mild
returned was 100% at baseline and 96% to 98% through
vasovagal symptoms, which were managed conservatively.
the remainder of the study. One patient in the control
One patient (in the control group) experienced a pulmonary
Mayo Clin Proc. • June 2006;81(6):749-757 • www.mayoclinicproceedings.com
For personal use. Mass reproduce only with permission from Mayo Clinic Pr
ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
TABLE 1. Analysis of Variance for the Fibromyalgia Impact Questionnaire (FIQ)*
*Acupuncture-control mean estimate is derived from a repeated-measures analysis of variance
model. This value is the mean expected difference between active and placebo with respect tothe particular FIQ subscale, adjusted for time (days since baseline measurement) and baselinesubscale value. Negative values for this estimate indicate that values for the active arm arelower than the placebo arm. Positive values indicate that values for the active arm are higher. The P values test whether the group effect is significantly different from 0. P<.05 suggests adifference between treatment groups with respect to the particular FIQ subscale. CI = confi-dence interval.
embolism. She had had a history of thromboembolic prob-
superior to the control group (P=.01). Subscale analysis
lems, and her complication was believed to be unrelated to
revealed significant group effects for symptoms of fatigue
and anxiety. The remainder of the subscales also showed
At the conclusion of the treatments, patients were asked
trends toward improvement of symptoms, although they
their opinion regarding group assignment. Approximately
were not statistically significant individually. Repeated-
half of the patients in each group reported that they did not
measures analysis of the MPI data is presented in Table 2.
know their assignment (13 [52%] in the control group and 10
The group effect showed significant improvement in pain
[40%] in the acupuncture group). Of the 12 in the control
(P=.03) up to 1 month after treatment, but the effect was
group who had an opinion, 7 (58%) were correct and 5 (42%)
not statistically significant when the 7-month data were
were incorrect. Of the 15 in the acupuncture group who had
an opinion, only 5 (33%) were correct and 10 (67%) were
Figure 6 shows the difference in FIQ score between the
incorrect. Hence, the ability of the patients to accurately
acupuncture and control groups at each time point, with the
determine the treatment they received did not exceed chance.
greatest difference at 1 month (P=.007). More detailed
Table 1 presents the results of the repeated-measures
comparisons of both the FIQ and MPI measurements at
analysis of variance for the FIQ. This analysis revealed a
each time point are given in Table 3. The total FIQ score in
positive group effect of acupuncture that was statistically
the acupuncture group was improved 7.4 points over the
TABLE 2. Analysis of Variance for the Multidimensional Pain Inventory (MPI)*
*Acupuncture-control mean estimate is derived from a repeated-measures analysis of variance
model. This value is the mean expected difference between active and placebo with respect to theparticular MPI subscale, adjusted for time (days since baseline measurement) and baseline subscalevalue. Negative values for this estimate indicate that values for the active arm are lower than theplacebo arm. Positive values indicate that values for the active arm are higher. The P values testwhether the group effect is significantly different from 0. P<.05 suggests a difference betweentreatment groups with respect to the particular MPI subscale. CI = confidence interval. Mayo Clin Proc. • June 2006;81(6):749-757 • www.mayoclinicproceedings.com
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
FIGURE 6. Effect of acupuncture and control on the Fibromyalgia Impact Questionnaire(FIQ) total score.
control group at 1 month after treatment (P=.007) At this
necessary for quality research in acupuncture because the
time point, pain severity as measured by the MPI was also
control group displayed the expected placebo response that
significantly decreased (P=.03). Other symptoms that
is typical of pain studies.11 An alternative choice for control
showed statistically significant improvement included fa-
treatments in studying acupuncture is to place needles at
tigue, anxiety, and affective distress. All symptom sub-
incorrect or “sham” points. Although it would have been
scales showed some improvement, although not all were
easier to use this as a control, we agree with others who
have argued that needling at sham locations is also likely toprovide neuromodulatory inputs to the sensory nervoussystem. Sham needling may in fact produce physiologic
changes indistinguishable from “true” acupuncture points.
In this controlled, randomized, and blinded assessment of
We believe that the simulated acupuncture configuration
acupuncture, our study patients were unable to determine
described herein provides an inexpensive and effective
in which group they had participated. Such blinding is
method of providing realistic placebo acupuncture treat-
TABLE 3. Results of the Fibromyalgia Impact Questionnaire (FIQ) and Multidimensional Pain Inventory (MPI)*
*Data are presented as mean ± 1 SD from analysis of covariance, adjusted for baseline values. Mayo Clin Proc. • June 2006;81(6):749-757 • www.mayoclinicproceedings.com
For personal use. Mass reproduce only with permission from Mayo Clinic Pr
ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
ments to patients who have not previously experienced
were randomized to receive either acupuncture or control
acupuncture (35 patients in each group). The control acu-
Acupuncture treatments were well tolerated by our pa-
puncture arm consisted of needle insertion at points 20 mm
tients. Most patients found participation in the study to be
away from the experimental points, with decreased inten-
pleasant and rewarding. Bruising and soreness were more
sity of electrical stimulation. Patients received 6 treatment
common in the acupuncture group than in the control
sessions and were assessed immediately after the course of
group, but these were mild and did not affect treatment.
acupuncture with no long-term follow-up. Intention-to-
Acupuncture rarely causes adverse effects that might limit
treat analysis showed that patients in the experimental
cognition or functional rehabilitation. Vasovagal symp-
group improved significantly in all parameters except
toms (in both the acupuncture group and the control group)
morning stiffness, whereas the controls had no change.
were the most troubling adverse effects for a few of our
Pain threshold was improved by 70% in the experimental
patients. Placing patients in the supine position would
group and 4% in the control group. Unfortunately, this
study did not use standardized or validated measures of
We found that acupuncture improved symptoms of
fibromyalgia symptoms or quality of life. Furthermore,
fibromyalgia significantly more than placebo. All symp-
there were no long-term follow-up measurements to deter-
tom subscales were improved with acupuncture, but only
fatigue and anxiety were statistically significant on their
Assefi et al7 studied 25 patients in the acupuncture group
own. Pain trended closely toward statistical significance in
compared with 3 separate control groups, each consisting
the FIQ (P=.07) and MPI (P=.05). However, fibromyalgia
of 25 patients. Their patients were drawn from “all comers”
is a syndrome of symptoms not just pain.
in the community who had fibromyalgia. Our patients were
Our patients were homogenous in diagnosis and severity
drawn from the Mayo Fibromyalgia Treatment Program,
of symptoms. The Fibromyalgia Treatment Program has
and thus they may have been more homogenous and possi-
been shown to reduce the mean FIQ total score from 51.3 to
bly more severely affected. It has been suggested that
44.7.12 The average FIQ total score of our patients at
patients at tertiary care centers have more severe disease.
baseline after the Fibromyalgia Treatment Program was
Our population may represent patients who have recalci-
42.5, which is close to the expected value. The improve-
trant symptoms or are more severely affected than the
ment observed in our study was additive to the benefits
general population. Many had already used most of the
obtained with the Fibromyalgia Treatment Program (ie,
basic treatments for fibromyalgia. Although this may be
educational and behavioral interventions).
the case, most of our patients were from the local commu-
We saw maximum benefit at 1 month (among time
nity, so such a referral bias may be less significant. The
points we considered), and that benefit was less signifi-
study by Assefi et al was performed at several sites by 8
cant at 7 months. Unfortunately, the design of this clinical
different acupuncturists. Our study was done at 1 site by 2
trial does not allow a more precise determination of
acupuncturists. This may have reduced the variability in
acupuncture’s duration. The time course of improvement
after acupuncture should be better characterized in future
The study by Assefi et al looked primarily at pain. Their
quality-of-life measurement, the Medical Outcomes Study
Although patients receiving acupuncture reported im-
36-Item Short-Form Health Survey, is not designed specifi-
proved symptoms, they did not report significantly in-
cally for patients with fibromyalgia. We looked at all
creased levels of activity or physical functioning. How-
symptoms of fibromyalgia with a disease-specific, vali-
ever, we neither set this as a goal for our patients nor
dated measurement tool, the FIQ. In fact, the FIQ was more
encouraged any changes in behavior, even if they men-
sensitive in detecting significant differences between
tioned symptomatic improvement during the study. Also,
the Fibromyalgia Treatment Program had already encour-
Our study showed that acupuncture reduced the FIQ
aged exercise and activity to these patients, so they may
score by 7 points. This benefit was additive to the benefi-
have previously adopted these suggestions. Regardless, the
cial effect produced by the Fibromyalgia Treatment Pro-
lack of functional improvement after reduction of chronic
gram, which also produced a mean benefit of 7 points.12
pain is not an observation unique to this study. Symptom
The magnitude of clinical benefit produced by acupuncture
reduction may be necessary, but not sufficient, for func-
is similar to that reported with pharmacological interven-
tions such as tricyclic antidepressants13 (7 points), fluox-
Two other randomized controlled studies of acupunc-
etine14 (8 points), and tramadol and acetaminophen15 (6
ture for fibromyalgia have been published.6,7 Deluze et al6
points). Therefore, the effect of acupuncture is both clini-
prospectively studied 70 patients with fibromyalgia who
cally and statistically significant. Mayo Clin Proc. • June 2006;81(6):749-757 • www.mayoclinicproceedings.com
For personal use. Mass reproduce only with permission from Mayo Clinic Proceedings.
ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
Our study has certain limitations. Perhaps most signifi-
We thank Gregory A. Wilson for study coordination and patient
cant is the relatively small size of the study population. recruitment; Heidi L. Schmitz, Carolyn J. Nereson, Victoria L.
Additionally, some will argue that the acupuncture therapy
Rud, Donna J. Fritsch, and Evelyn K. Perry for help with patient
provided was not optimal with respect to point selection,
scheduling and appointment flow; and Yuko F. Voss, BA, Megan
elicitation of de Qi, and electrical stimulation. To preserve
M. O’Byrne, MA, and Cyndy O. Townsend, PhD, for help withdata analysis.
blinding, the design of the study did not allow customizedpoint selection or specific elicitation of the de Qi sensation,sometimes referred to as “needle grab.” Some schools of
acupuncture require this sensation as an indication of
1. Buskila D. Fibromyalgia, chronic fatigue syndrome, and myofascial pain
syndrome. Curr Opin Rheumatol. 2001;13:117-127.
proper needle position. However, studies suggest that the
2. Wolfe F, Ross K, Anderson J, Russell IJ. Aspects of fibromyalgia in the
sensation of de Qi occurs equally frequently at true and
general population: sex, pain threshold, and fibromyalgia symptoms. J.
sham acupuncture points.16 Nevertheless, these deficien-
3. Wahner-Roedler DL, Elkin PL, Vincent A, et al. Use of complementary
cies would tend to minimize the treatment effect observed.
and alternative medical therapies by patients referred to a fibromyalgia treat-
Hence, our results may represent a minimum effectiveness
ment program at a tertiary care center. Mayo Clin Proc. 2005;80:55-60. 4. NIH Consensus Development Panel on Acupuncture. Acupuncture.
Our patients were mostly women, which does not accu-
5. Berman BM, Ezzo J, Hadhazy V, Swyers JP. Is acupuncture effective in
the treatment of fibromyalgia? J Fam Pract. 1999;48:213-218.
rately reflect the male-female ratio of the incidence of
6. Deluze C, Bosia L, Zirbs A, Chantraine A, Vischer TL. Electroacu-
fibromyalgia. This may represent scheduling difficulties on
puncture in fibromyalgia: results of a controlled trial. BMJ. 1992;305:1249-1252.
behalf of potential patients or other factors that limited
7. Assefi N, Sherman K, Jacobsen C, Goldberg J, Smith W, Buchwald D. A
randomized clinical trial of acupuncture compared with sham acupuncture in
enrollment by men. Our population was also predomi-
fibromyalgia. Ann Intern Med. 2005;143:10-19.
nantly white, which reflects the community population in
8. Burckhardt CS, Clark SR, Bennett RM. The fibromyalgia impact ques-
tionnaire: development and validation. J Rheumatol. 1991;18:728-733.
Olmsted County, Minnesota, where this study was con-
9. Turk DC. Customizing treatment for chronic pain patients: who, what,
ducted. Future research should extend these observations to
and why. Clin J Pain. 1990;6:255-270.
men and to other ethnic and racial groups. 10. Turk DC, Okifuji A, Sinclair JD, Starz TW. Differential responses by
psychosocial subgroups of fibromyalgia syndrome patients to an interdiscipli-nary treatment. Arthritis Care Res. 1998;11:397-404. 11. Turner J, Deyo R, Loeser J, VonKorff M, Fordyce W. The importance of
placebo effects in pain treatment and research. JAMA. 1994;271:1609-1614. 12. Pfeiffer A, Thompson J, Nelson A, et al. Effects of a 1.5-day multi-
This study represents a prospective, blinded, randomized
disciplinary outpatient treatment program for fibromyalgia: a pilot study. Am J
trial of acupuncture for patients with fibromyalgia. Acu-
Phys Med Rehabil. 2003;82:186-191. 13. Heymann RE, Helfenstein M, Feldman D. A double-blind, randomized,
puncture was well tolerated with minimal adverse effects.
controlled study of amitriptyline, nortriptyline and placebo in patients with
Symptoms of fibromyalgia improved in the acupuncture
fibromyalgia: an analysis of outcome measures. Clin Exp Rheumatol. 2001;19:697-702.
group to a greater extent than in the control group. Specific
14. Goldenberg D, Mayskiy M, Mossey C, Ruthazer R, Schmid C. A ran-
symptoms that showed the most significant improvements
domized, double-blind crossover trial of fluoxetine and amitriptyline in thetreatment of fibromyalgia. Arthritis Rheum. 1996;39:1852-1859.
included fatigue and anxiety. The improvement was both
15. Bennett RM, Kamin M, Karim R, Rosenthal N. Tramadol and acetamin-
clinically and statistically significant. Therefore, acupunc-
ophen combination tablets in the treatment of fibromyalgia pain: a double-
ture may have a role in the symptomatic treatment of
blind, randomized, placebo-controlled study. Am J Med. 2003;114:537-545. 16. Vincent CA, Richardson PH, Black JJ, Pither CE. The significance of
needle placement site in acupuncture. J Psychosom Res. 1989;33:489-496. Mayo Clin Proc. • June 2006;81(6):749-757 • www.mayoclinicproceedings.com
For personal use. Mass reproduce only with permission from Mayo Clinic Pr
Rebecca Weng BOptom Brien Holden Vision Institute r.weng@brienholdenvision.org Acute Bacterial Conjunctivitis ABSTRACT Acute bacterial conjunctivitis is encountered frequently in optometric practice. The condition often resolves on its own without any treatment. Although it is a self-limiting condition, current initial treatment for bacterial conjunctivitis is the application
nineteen years on the job Part 2 of a 2-part article by Lindy Dunagan-Groger [Volume 12 Number 2 (June 2002) features part 1 of this article] n the year that Michael turned 18 I transitioned into a new set of I am an organized documentation- issues — those of parenting and being person; I have kept all those papers and a young adult. This included officially obtaining disabili
 ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
was reduced appropriately. After placement of all needlesand initiation of electrical stimulation, patients were al-lowed to rest quietly in a darkened room while relaxingmusic played in the background for 20 minutes.
ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
was reduced appropriately. After placement of all needlesand initiation of electrical stimulation, patients were al-lowed to rest quietly in a darkened room while relaxingmusic played in the background for 20 minutes.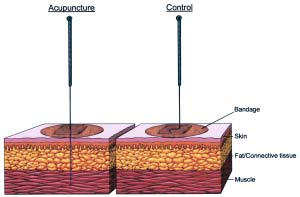
 ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
ing treatment effects at individual time points usinganalysis of covariance complemented this analysis. Sec-ondary analyses involved analyzing the FIQ and MPIsubscales individually using similar techniques as de-scribed herein.
ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
ing treatment effects at individual time points usinganalysis of covariance complemented this analysis. Sec-ondary analyses involved analyzing the FIQ and MPIsubscales individually using similar techniques as de-scribed herein.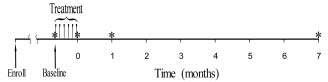 ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
FIGURE 4. Timeline for each patient. At least 4 weeks elapsed between enrollment and baselineassessment. Patients were then randomized to receive 6 acupuncture or 6 control treatments duringa 2- to 3-week period. Assessments (indicated by asterisks) were made at baseline, treatmentcompletion (0 months), and 1 and 7 months after treatment.
ACUPUNCTURE IMPROVES FIBROMYALGIA SYMPTOMS
FIGURE 4. Timeline for each patient. At least 4 weeks elapsed between enrollment and baselineassessment. Patients were then randomized to receive 6 acupuncture or 6 control treatments duringa 2- to 3-week period. Assessments (indicated by asterisks) were made at baseline, treatmentcompletion (0 months), and 1 and 7 months after treatment.