Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Microsoft word - joc130058supp1_edited.doc
Supplementary Online Content
Gerber JS, Prasad PA, Fiks AG, et al. Effect of an outpatient antimicrobial stewardship intervention on broad-spectrum antibiotic prescribing by primary care pediatricians: a randomized trial. JAMA. doi:10.1001/jama.2013.6287
eAppendix. Content Summaries of Clinician Education for Sinusitis, Pharyngitis, and Pneumonia eFigure 1. Example Clinician Feedback Report eFigure 2. Study Timeline eTable 1.ICD-9 Codes and Laboratory Test Results Used for ARTI Case Definitions eTable 2.ICD-9 Codes Used for Defining Non-ARTI Diagnoses Excluded From Analyses eTable 3. Antibiotic Prescribing by Condition With Supplementary (Post Hoc) Pre-Post Analyses Confirming the Results of the Primary Analyses
This supplementary material has been provided by the authors to give readers additional information about their work.
2013 American Medical Association. All rights reserved.
Downloaded From: http://pubs.jamanetwork.com/ on 03/09/2014 eAppendix. Content Summaries of Clinician Education for Sinusitis, Pharyngitis, and Antimicrobial Treatment of PHARYNGITIS in Children
Most cases of pharyngitis are viral in origin.
Antimicrobial therapy should NOT be given to a child with pharyngitis in the absence of positive
rapid test or positive culture for Group A Streptococcus (GAS).
For the treatment of the non-allergic patient with documented GAS pharyngitis:
Penicillin (PO or IM) is recommended Amoxicillin is an acceptable alternative
A clinical isolate of GAS resistant to penicillin has NEVER been documented.
Azithromycin and cephalosporins (e.g. cephalexin/keflex, cefdinir/omnicef), though active
against GAS, are not recommended for routine treatment of GAS pharyngitis because:
These drugs have NOT been shown to be superior for the treatment of GAS pharyngitis, or for the prevention of suppurative or non-suppurative sequelae (e.g. acute rheumatic fever) of GAS pharyngitis.
Data does not support increased patient compliance of these oral medications over oral penicillin or amoxicillin.
Exposure to such broad-spectrum agents promotes resistance to these and other antibiotics.
Sources:
Red Book: Report of the Committee on Infectious Diseases. 2009. American Academy of
2013 American Medical Association. All rights reserved.
Downloaded From: http://pubs.jamanetwork.com/ on 03/09/2014 Antimicrobial Treatment of PNEUMONIA in Children
After respiratory viruses, Streptococcus pneumoniae remains the predominant organism causing
uncomplicated, community-acquired pneumonia in children, particularly in those between ages 3 months and 6 years of age.
Initial antimicrobial treatment of uncomplicated, community-acquired pneumonia in children
should be with a narrow-spectrum agent with good activity against Streptococcus pneumoniae.
Because of its effectiveness, safety, tolerability, low cost, and narrow spectrum:
amoxicillin (80-90 mg/kg/day) is recommended
(zithromax), cefdinir (omnicef), and cefixime (suprax) have inferior activity,
relative to amoxicillin, against Streptococcus pneumoniae.
The addition of clavulanate to amoxicillin (amoxicillin-clavulanate/augmentin) does NOT
enhance its activity against Streptococcus pneumoniae.
Sources:
Red Book: Report of the Committee on Infectious Diseases. 2009. American Academy of
Antimicrobial Treatment of SINUSITIS in Children
Based on the available data, initial antimicrobial treatment of acute, uncomplicated sinusitis
should be with a narrow-spectrum agent targeting Streptococcus pneumoniae.
Because of its effectiveness, safety, tolerability, low cost, and narrow spectrum:
amoxicillin (80-90 mg/kg/day) is recommended
(zithromax) and cefdinir (omnicef) have inferior activity, relative to amoxicillin,
against Streptococcus pneumoniae.
The addition of clavulanate to amoxicillin (amoxicillin-clavulanate/augmentin) does NOT
enhance its activity against Streptococcus pneumoniae.
Sources:
Red Book: Report of the Committee on Infectious Diseases. 2009. American Academy of
IDSA Clinical Practice Guidelines. Practice Guidelines for the Diagnosis and Management of
Group A Streptococcal Sinusitis. 2002. Available at: http://www.idsociety.org/
2013 American Medical Association. All rights reserved.
Downloaded From: http://pubs.jamanetwork.com/ on 03/09/2014 eFigure 1. Example Clinician Feedback Report
Abbreviations: Rx, Prescription; Q, Quarter.
2013 American Medical Association. All rights reserved.
Downloaded From: http://pubs.jamanetwork.com/ on 03/09/2014 eFigure 2. Study Timeline
Feedback reports occurred at 4-month intervals
2013 American Medical Association. All rights reserved.
Downloaded From: http://pubs.jamanetwork.com/ on 03/09/2014 eTable 1.ICD-9 Codes and Laboratory Test Results Used for ARTI Case Definitions Viral ARTIs ICD-9 Codes Bacterial ARTIs ICD-9 Codes
461.8, 461.9, 473.9, 473.2, 473.1, 473.0, 487.1
(034.0 or 462 or 463) AND (rapid strep or culture positive)
Abbreviations: ICD-9, International Classification of Disease, 9th edition; ARTI, Acute Respiratory Tract Infections; URI, Upper Respiratory Tract Infection
2013 American Medical Association. All rights reserved.
Downloaded From: http://pubs.jamanetwork.com/ on 03/09/2014 eTable 2. ICD-9 Codes Used for Defining Non-ARTI Diagnoses Excluded From Analyses Non-ARTIs ICD-9 Codes
380.10, 380.11, 380.12, 380.13, 380.14, 380.15, 380.16
680, 680.0, 680.1, 680.2, 680.3, 680.4, 680.5, 680.6, 680.7, 680.8, 680.9, 681, 681.0, 681.00, 681.01, 681.02, 681.1, 681.10, 681.11, 681.9, 682, 682.0, 682.1, 682.2, 682.3, 682.4, 682.5, 682.6, 682.7, 682.8, 682.9
879.8, 879.9, 959.9, E906.5, E906.0, E906.3, 891.0, 890.0, 884.0, 883.0, 882.0, 881.00
Streptococcal) Streptococcal infection (without
034.1, 041, 041.00, 041.01, 041.1, 041.09, 390, 040.82, 566,
079.9, 079.88, 079.98, 614.9, 616.1, 616.10
730.20, 730.21, 730.22, 730.23, 730.24, 730.25, 730.26, 730.27, 730.28, 730.29, 711.06, 711.05, 711.03, 711.00
008.5, 008.43, 008.00, 004.9, 004.3, 003.9, 003.1, 003.0
Abbreviations: ICD-9, International Classification of Disease, 9th edition; ARTI, Acute Respiratory Tract Infections
2013 American Medical Association. All rights reserved.
Downloaded From: http://pubs.jamanetwork.com/ on 03/09/2014 eTable 3. Antibiotic Prescribing by Condition With Supplementary (Post Hoc) Pre-Post Analyses Confirming the Results of the Primary Analyses Rate (%): Difference Post – Pre % In period In period ABX/sick visit 0.5 (-0.1, 1.1); p=0.13 Strep/sick visit 0.2 (-0.2, 0.6); p=0.42 PNA/sick visit -0.1 (-0.3, 0.1); p=0.25 Sinu/sick visit 0.2 (-0.2, 0.6); p=0.52 Broad/All ABX INT -7.3 (-11.9, -2.7); p<0.001 Broad/Strep 0.8 (-2.3, 4.0); p=0.82 Broad/PNA -3.2 (-10.8, 4.4); p=0.05 Broad/SINU -15.9 (-26.1, -5.8); p=0.002
Tx: treatment (I=intervention; C=control; Diff = difference between treatment and control groups All rates are standardized estimates (see text and references for details on standardization) based on a logistic regression model with main effects for period (pre vs. post), a main effect for intervention, and the interaction. Covariates used for standardization are the same as those listed in the text. P-values are based on the Wald test for the interaction term. P-values and confidence intervals allow for the cluster-randomized design. P-values can differ from the primary models (displayed in the figures and reported in the text), which account for the trajectories of prescribing prior to the intervention and then compare these trajectories to those after the intervention. Counts represent the number of prescriptions/number of visits during the entire period, pre-intervention or intervention.
2013 American Medical Association. All rights reserved.
Downloaded From: http://pubs.jamanetwork.com/ on 03/09/2014
TRIGEMINAL NEURALGIA ASSOCIATION TEXAS SUPPORT GROUPS NEWSLETTER JULY 2006 SAN ANTONIO SUPPORT GROUP MEETING – DATE CHANGE The San Antonio Support Group will meet next on August 1 not August 8 as originally planned. Jonathan White, M.D. with UT Southwestern in Dallas will be the guest speaker. For more details, please check the meeting flyer. FORT WORTH
Basic om Whisky Det finns mer än skottar som producerar Whisk(e)y Whisky är ett alltför enkelt ord som för många bara betyder en drink med kiltvarning. Varför krångla till det, ta något billigt och kasta i några isbitar som dom gör på film. För andra är tvärtom, man är mycket noga med sin whisky och dess traditioner och ursprung. Malt, peat, blended, vatted, pot s
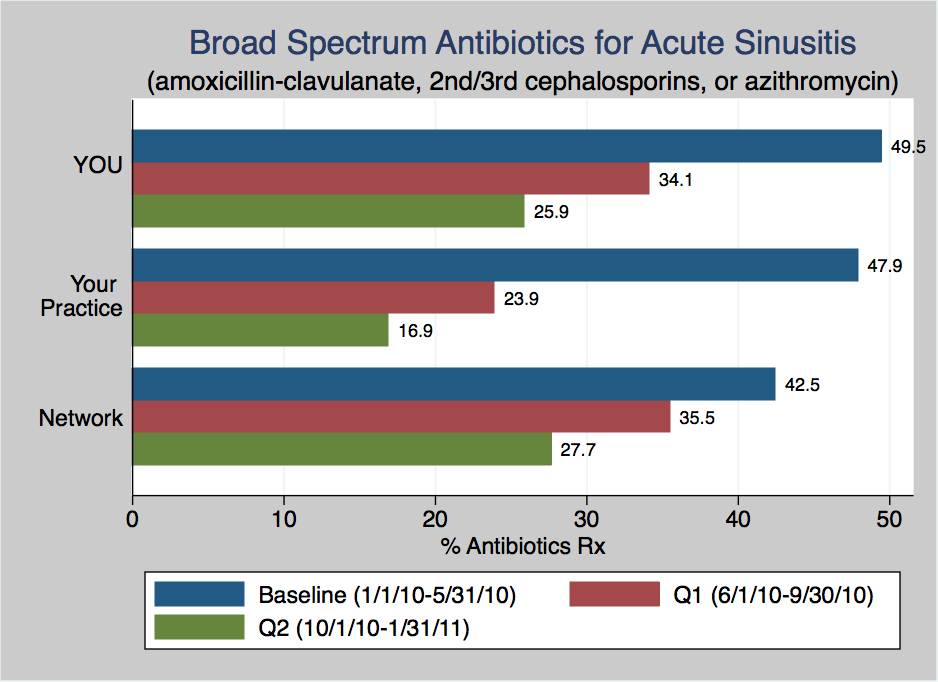 eFigure 1. Example Clinician Feedback Report
eFigure 1. Example Clinician Feedback Report 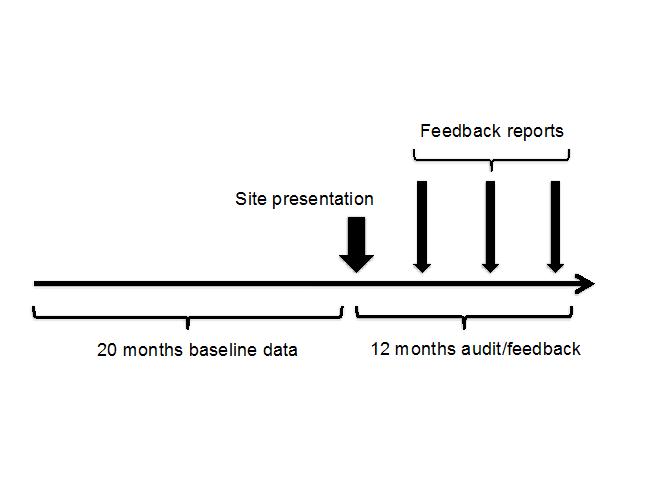 eFigure 2. Study Timeline
eFigure 2. Study Timeline