Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Doi:10.1016/j.jpain.2005.01.353
Botulinum Toxin A Injection of the Obturator Internus Muscle
Abstract: Chronic perineal pain is often a difficult condition to manage. Current treatments include pudendal nerve injections and pudendal nerve release surgery. The obturator internus muscle has a close relationship to the pudendal nerve and might be a potential target for therapeutic intervention. Perspective: A case is presented of refractory perineal pain that was successfully treated by injecting the obturator internus muscle with botulinum toxin A.
2005 by the American Pain Society Key words: Chronic pain, perineal pain, obturator internus, botulinum toxin.
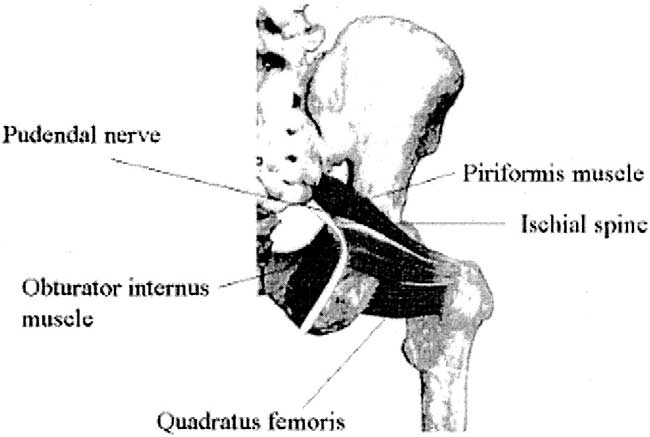
Thecauseofchronicperinealpainisoftendifficult Thepudendalnerveenterstheglutealre-
to identify and the syndrome difficult to
gion through the lower part of the greater sciatic fo-
Musculoskeletal dysfunction might contribute to
ramen below the piriformis muscle. It hooks around
the signs and symptoms of chronic pelvic Al-
the sacrospinous ligament near its attachment to the
though the obturator internus muscle has been identi-
ischial spine; the pudendal nerve reenters the pelvis
through the lesser sciatic foramen and through the
written about this muscle as a possible target for thera-
pudendal (Alcock’s) canal that is formed by the obtu-
peutic intervention. The fascia of the obturator internus
rator fascia on the lateral wall of the ischioanal fossa
muscle contributes to the formation of the pudendal
Within the pudendal canal, the pudendal nerve
canal and when thickened might become a possible en-
divides into 2 terminal branches, the perineal nerve
trapment Injections into the muscle, adjacent to
and the dorsal nerve of the penis or clitoris.
the canal, might have beneficial effects because of ac-
The pudendal canal is a fascial tunnel on the medial
tions on both the muscle and the nerve in terms of de-
aspect of the obturator internus muscle. The obturator
creasing compression and modulation of neurotransmit-
internus muscle originates within the pelvis on the obtu-
Botulinum toxin has been used successfully in the
rator membrane, a membrane that closes all but the su-
perior border of the obturator foramen, and on those
ported indicating that injection of the obturator inter-
portions of the pubis and ischium that surround the ob-
nus muscle with botulinum toxin might be a therapeutic
turator foramen. It is a lateral rotator of the thigh. Al-
option for patients with chronic perineal pain. This case
though broad in origin, the muscle tapers to a narrow
report received institutional review board approval, and
tendon that passes through the lesser sciatic foramen
the subject of the case report gave signed consent for
and rides over the ischial body (over a bursa) just superior
to the ischial tuberosity to attach on the medial aspect ofthe greater trochanter of the femur. Anatomy of the Pudendal Nerve and Obturator Internus Muscle Case Report
Arising from the sacral plexus (S2, 3, 4), the pudendal
A 64-year-old woman complained of right-sided pelvic
nerve is a sensory and motor nerve to the peri-
pain affecting the upper leg, vagina, and rectum. Thepain was rated at a level of 4 to 8 out of 10 on a visualanalogue scale and had been present for 4 years. The
Received June 28, 2004; Revised January 3, 2005; Accepted January 3,2005.
pain was aggravated by sitting. Previous diagnoses made
From the Center for Pain Management, Baylor University Medical Center,
included lumbosacral radiculopathy, post-laminectomy
syndrome, pudendal nerve entrapment, sacroiliac joint
Address reprint requests to Noor M. Gajraj, MD, Baylor Center for PainManagement, 5575 Warren Parkway, POB1, Suite 220, Frisco, TX 75034.
dysfunction, and piriformis syndrome. The patient had
received numerous medications and injection therapies
in the past including pudendal nerve injections with local
2005 by the American Pain Societydoi:10.1016/j.jpain.2005.01.353
anesthetic and steroid, sacroiliac joint injections, and
The Journal of Pain, Vol 6, No 5 (May), 2005: pp 333-337
the second injection 100 units of botulinum A in 3 mL0.25% bupivacaine was injected on a separate occasion. Discussion
Pudendal nerve entrapment is a recognized cause of
chronic perineal typically presentingas pain in the penis, scrotum, labia, perineum, or anorec-tal region. Pudendal nerve pathology might also causeurinary incontinence, anal incontinence, and dysorgas-mia. Pudendal nerve entrapment is a clinical diagnosismade in patients with the typical history of perineal painaggravated by sitting, relieved by standing, and absentwhen recumbent or sitting on a toilet seat. No widelyaccepted confirmatory test is available, although a neu-
Figure 1. Anatomy of the obturator internus muscle and pu-
rophysiologic examination might confirm nerve dam-
The pudendal nerve is predisposed to entrapment at
the level of the ischial spine and within the pudendalAt the ischial spine, the nerve can be com-
piriformis muscle injections. Other previous therapies in-
pressed between the sacrotuberous and sacrospinous
cluded physical therapy and water aerobics. The patient
ligaments. At the pudendal canal, the pudendal nerve
also had a pudendal nerve release procedure in France 2
can be compressed by the falciform process of the sa-
years previously, but with only partial relief. Medications
crotuberous ligament. The fascia on the obturator in-
being taken at the time of the office visit included meth-
ternus contributes to the formation of the pudendal
adone 20 mg twice a day, zonegran 200 mg twice a day,
canal. If thickened, the obturator fascia also might act
Zoloft 50 mg once daily, valium 5 mg at night, and
zanaflex 12 mg at night. Physical examination showed a
nerve entrapment include local anesthetic and steroid
distressed woman, uncomfortable while sitting, but
there were no focal neurologic signs. A vaginal examina-
tion was not performed at that time but had been per-
toxin have been reported in patients with cervical dys-
formed by a previous physician and showed tenderness
tonia and spastic disorders.More patients re-
at the right anterior and right posterior lateral regions.
ported improvement in pain than dystonia, raising the
The patient underwent a right obturator internus mus-
possibility that pain relief might not be solely the re-
cle injection with bupivacaine 0.25%, which gave 90%
relief for 12 hours. The average preprocedural and post-
toxin has been used successfully in pain management
procedural visual analogue scale scores were 7 of 10 and
1 of 10, respectively. After a subsequent botulinun toxin
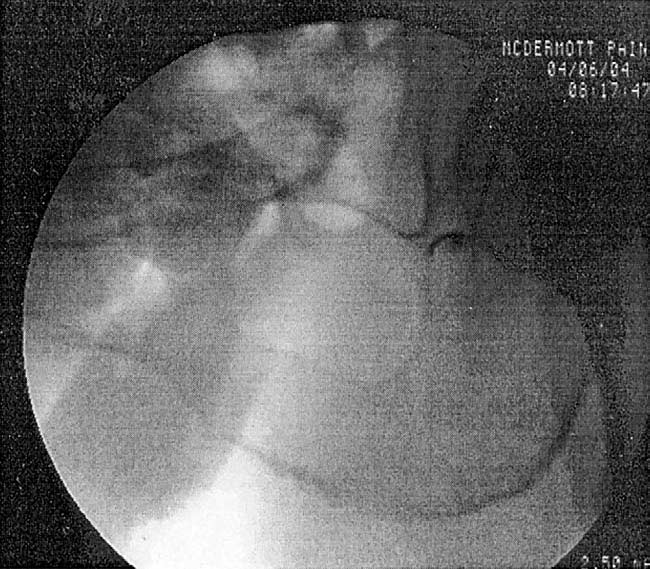
A injection, the patient again reported 90% relief fromher pain for more than 3 months. Pain assessments weremade before the procedure and then at 1-hour intervalsafter the procedure by using a 0 to 10 numeric ratingscale. There were no adverse effects such as motor weak-ness or disturbance of bowel or bladder function. Fluoroscopically Guided Obturator Internus Muscle Injection Technique
The patient was placed in the prone position. Standard
monitors were applied consisting of electrocardiogram,pulse oximetry, and an automated blood pressure de-vice. Sedation was achieved by using increments of intra-venous midazolam and fentanyl. Fluoroscopy was usedto visualize the obturator foramen. The skin and subcu-taneous tissues were anesthetized by using 1% lido-caine. With an aseptic technique and transgluteal ap-proach, a 22-gauge spinal needle was advanced to thelateral border of the obturator foramen, inferior to theischial spine Correct needle placement was con-firmed by injecting 1 mL of iohexol. For the diagnostic
Figure 2. Fluoroscopic view of right obturator internus muscle
injection 5 mL of 0.25% bupivacaine was injected. For
and bruising at the injection site, a flu-like syn-
mouth, dysphagia, and formation of neutralizing an-
num toxin not only inhibits acetylcholine release but
also the release of pain neurotransmitters such as glu-
tamate, substance P, calcitonin gene-related peptide,
it can be very useful in refractory Botulinum
toxin is usually reconstituted by mixing the contents of
ter release might prevent local sensitization of noci-
a vial with normal saline, although it is also common
ceptors and thus reduce the perception of pain. Botu-
practice to use local anesthetic as a In the
linum toxin might also alter impulse transmission
case reported, the pain relief obtained by the botuli-
within the dorsal horn pathways responsible for hy-
num toxin injection might have resulted in part from
the bupivacaine, although this effect would be ex-
action include changes in the sensitivity and response
pected to last only hours rather than months. Injection
patterns of muscle nociceptors, diminished activity in
of botulinum toxin into the obturator internus muscle
the gamma-motor neurons with consequent changes
in muscle spindle afferents, alterations in cholinergic
In conclusion, obtutator internus muscle injections
control of vascular and autonomic functions, and di-
might be a therapeutic option for patients with
rect noncholinergic effects on pain The du-
chronic perineal pain whose other treatments have
ration of action of botulinum toxin correlates with
failed. The precise mechanism of action and the rela-
neural sprouting and reinnervation of the muscle,
tive actions on the muscle and pudendal nerve remain
which restores function in 1 to 4 mAdverse
to be elucidated. Evidence for efficacy from a single
events from botulinum toxin therapy are not generally
serious and might include localized pain, tenderness,
randomized controlled studies are required. References
10. Borodic GE, Acquadro MA, Johnson EA: The use of bot-ulinum toxin for the treatment of chronic facial pain. J Pain3:21-27, 2002
1. Clinical Management Guidelines for Obstetrician-Gyne-cologists: Number 51, March 2004: Chronic Pelvic Pain. Ob-
11. Calvillo O, Skaribas IM, Rockett C: Computed tomogra-
phy-guided pudendal nerve block. A new diagnostic ap-proach to long-term anoperineal pain: A report of two
2. Amarenco G, Lanoe Y, Ghnassia RT, Goudal H, Perrigot M:
cases. Reg Anesth Pain Med 25:420-423, 2000
Alcock’s canal syndrome and perineal neuralgia. Rev Neurol(Paris) 144:523-526, 1988
12. Chalkiadaki A, Rohr UP, Hefter H: Early pain reduction inthe treatment of spasticity after a single injection of botuli-
3. Andersen OK, Gracely RH: Facilitation of the human no-
num A toxin. Dtsch Med Wochenschr 126:1361-1364, 2001
ciceptive reflex by stimulation of A beta-fibres in a second-ary hyperalgesic area sustained by nociceptive input from
13. Cheshire WP, Abashian SW, Mann JD: Botulinum toxin
the primary hyperalgesic area. Acta Physiol Scand 155:87-97,
in the treatment of myofascial pain syndrome. Pain 59:65-
4. Aoki KR: Evidence for antinociceptive activity of botuli-
14. Difazio D, Jabbari B: A focused review of the use of
num toxin type A in pain management. Headache 43:S9-S15,
botulinum toxins for low back pain. Clin J Pain 18:S155-S162,
5. Arezzo JC: Possible mechanisms for the effects of botuli-
15. Foster L, Clapp L, Erickson M, Jabarri B: Botulinum toxin
num toxin on pain. Clin J Pain 18:S125-S132, 2002
A and chronic low back pain: A randomized, double-blindstudy. Neurology 56:1290-1293, 2001
6. Ashton AC, Dolly JO: Characterization of the inhibitoryaction of botulinum neurotoxin type A on the release of
16. Freund B, Schwartz M, Symington JM: Botulinum toxin:
several transmitters from rat cerebrocortical synaptosomes.
New treatment for temporomandibular disorders. Br J Oral
7. Baker PK: Musculoskeletal origins of chronic pelvic pain:
17. Gobel H, Heinze A, Heinze-Kuhn K, Austermann K: Bot-
Diagnosis and treatment. Obstet Gynecol Clin North Am 20:
ulinum toxin A in the treatment of headache syndromes and
pericranial pain syndromes. Pain 91:195-199, 2001
8. Bigalke H, Heller I, Bizzini B: Tetanus toxin and botulinum
18. Guis-Sabatier S, Pieri-Balandraud N, Garnier-Soumet P,
A toxin inhibit release and uptake of various transmitters, as
Coste J, Roux H, Mattei JP: Pubic pain in athletes: A case due
studied with particulate preparations from rat brain and
to an abscess in the obturator muscle. Rev Rhum Engl Ed
19. Gunter J, Brewer A, Tawfik O: Botulinum toxin a for
9. Borodic G, Acquadro M, Johnson E: Botulinum toxin ther-
vulvodynia: A case report. J Pain 5:238-240, 2004
apy for pain and inflammatory disorders: mechanisms andtherapeutic effects. Expert Opin Investig Drugs 10:1531-
20. Guyer BM: Mechanism of botulinum toxin in the relief
of chronic pain. Curr Rev Pain 3:427-431, 1999
21. Herskowitz A, Herskowitz B: Treatment of neck and
40. O’Brien PC: The use and misuse of N-of-one studies. Int
shoulder pain with botulinum neurotoxins. Pain Practice
41. Padberg M, de Bruijn SF, de Haan RJ, Tavey DLJ: Treat-
22. Hodgson M: N-of-one clinical trials: The practice of en-
ment of chronic tension-type headache with botulinum tox-
vironmental and occupational medicine. J Occup Med 35:
in: A double-blind, placebo-controlled clinical trial. Cepha-
23. Holds JB, Alderson K, Fogg SG, Anderson RL: Motor
42. Pisani R, Stubinski R, Datti RA: Entrapment neuropathy
nerve sprouting in human orbicularis muscle after botuli-
of the internal pudendal nerve: Report of two cases. Scand
num A injection. Invest Ophthalmol Vis Sci 31:964-967, 1990
24. Hough DM, Wittenberg KH, Pawlina W, Maus TP, King
43. Porta M: A comparative trial of botulinum toxin type A
BF, Vrtiska TJ, Farrell MA, Antolak SJ: Chronic perineal pain
and methylprednisolone for the treatment of myofascial
caused by pudendal nerve entrapment: Anatomy and CT-
pain syndrome and pain from chronic muscle spasm. Pain
guided perineural injection technique. Am J Roentgenol
44. Raj PP: Botulinum neurotoxin in chronic pain manage-
25. Ishikawa H, Mitsui Y, Yoshitomi T, Mashimo K, Aoki S,
Mukuno K, Shimizu K: Presynaptic effects of botulinumtoxin type A on the neuronally evoked response of albino
45. Raj PP: Treatment algorithm overview: BoNT therapy for
and pigmented rabbit iris sphincter and dilator muscles. Jpn
46. Ramsden CE, McDaniel MC, Harmon RL, Renney KM:
26. Jabbari B, Ney J: Treatment of low back pain with bot-
Pudendal nerve entrapment as source of intractable peri-
ulinum neurotoxins. Pain Practice 4:S47-S53, 2004
neal pain. Am J Phys Med Rehabil 82:479-484, 2003
47. Robert R, Prat-Pradal D, Labat JJ, Bensignor M, Raoul S,
27. Jankovic J, Brin MF: Therapeutic uses of botulinum
Rebai R, Leborgne L: Anatomic basis of chronic perineal
pain: Role of the pudendal nerve. Surg Radiol Anat 20:93-98,
28. Jarvis SK, Abbott JA, Lenart MB, Steensma A, Vancaillie
TG: Pilot study of botulinum toxin type A in the treatment of
48. Rohde RS, Ziran BH: Obturator internus tendinitis as a
chronic pelvic pain associated with spasm of the levator ani
source of chronic hip pain. Orthopedics 26:425-426, 2003
muscles. Aust N Z J Obstet Gynaecol 44:46-50, 2004
49. Royal MA: Botulinum toxins in pain management. Phys
29. Johnson EA: Clostridial toxins as therapeutic agents:
Benefits of nature’s most toxic proteins. Ann Rev Microbiol53:551-575, 1999
50. Royal MA: The use of botulinum toxins in the manage-ment of pain and headache. Pain Practice 1:215-235, 2001
30. Kelm S, Gerats G, Chalkiadaki A, Hefter H: Reduction ofpain and muscle spasms by botulinum toxin A. Nervenarzt
51. Schraffordt SE, Tjandra JJ, Eizenberg N, Dwyer PL: Anat-
omy of the pudendal nerve and its terminal branches: Acadaver study. ANZ J Surg 74:23-26, 2004
31. Lang AM: Botulinum toxin type B in piriformis syn-drome. Am J Phys Med Rehabil 83:198-202, 2004
52. Schulte-Mattler WJ, Krack P: Treatment of chronic ten-sion-type headache with botulinum toxin A: A randomized,
32. Leigh RE: Obturator internus spasm as a cause of pelvic
double-blind, placebo-controlled multicenter study. Pain
and sciatic distress. Lancet 72:286-287, 1952
33. Lew MF: Review of the FDA-approved uses of botulinum
53. Shafik A: Pudendal canal syndrome: A cause of chronic
toxins, including data suggesting efficacy in pain reduction.
54. Shafik A, el-Sherif M, Youssef A, Olfat ES: Surgical anat-
34. Loening-Baucke V, Read NW, Yamada T, Barker AT:
omy of the pudendal nerve and its clinical implications. Clin
Evaluation of the motor and sensory components of the
pudendal nerve. Clin Neurophysiol 93:35-41,1994
55. Shafik A, El-Sibai O: Botulin toxin in the treatment of
35. Mauillon J, Thoumas D, Leroi AM, Freger P, Michot F,
nonrelaxing puborectalis syndrome. Dig Surg 15:347-351,
Denis P: Results of pudendal nerve neurolysis-transposition
in twelve patients suffering from pudendal neuralgia. DisColon Rectum 42:186-192, 1999
56. Silberstein S: Botulinum neurotoxins: Origins and basicmechanisms of action. Pain Practice 4:S19-S26, 2004
36. McDonald JS, Spigos DG: Computed tomography-guided pudendal block for treatment of pelvic pain due to
57. Slocumb JC: Neurological factors in chronic pelvic pain:
pudendal neuropathy. Obstet Gynecol 95:306-309, 2000
Trigger points and the abdominal pelvic pain syndrome. Am J Obstet Gynecol 149:536-543, 1984
37. Naumann M, Jankovic J: Safety of botulinum toxin typeA: A systematic review and meta-analysis. Curr Med Res
58. Smith HS, Audette J, Royal MA: Botulinum toxin in pain
management of soft tissue syndromes. Clin J Pain 18:S147-S154, 2002
38. Naumann M, Yakovleff A, Durif F: A randomized, dou-ble-masked, crossover comparison of the efficacy and safety
59. Sundaraj SR, Ponciano P, Johnstone C , Noore F, Castro
of botulinum toxin type A produced from the original bulk
M: Treatment of chronic refractory intractable headache
toxin source and current bulk toxin source for the treatment
with botulinum toxin type A: A retrospective study. Pain
of cervical dystonia. J Neurol 249:57-63, 2002
39. Neill ME, Swash M: Chronic perianal pain: An unsolved
60. Swezey RL: Obturator internus bursitis: A common fac-
tor in low back pain. Orthopedics 16:783-785, 1993
61. Tarsy D, First ER: Painful cervical dystonia: Clinical fea-
65. Tsui JK, Eisen A, Stoessl AJ, Calne S, Calne DB: Double-
tures and response to treatment with botulinum toxin. Mov
blind study of botulinum toxin in spasmodic torticollis. Lan-
62. Tepper SJ: Treatment of headache pain with botulinum
66. Turner ML, Marinoff SC: Pudendal neuralgia. Am J Ob-
neurotoxins. Pain Practice 4:S38-S46, 2004
63. Tetzschner T, Sorensen M, Lose G, Christiansen J: Puden-
67. Welch MJ, Purkiss JR, Foster KA: Sensitivity of embryonic
dal nerve function during pregnancy and after delivery. Int
rat dorsal root ganglia neurons to Clostridium botulinum
Urogynecol J Pelvic Floor Dysfunct 8:66-68, 1997
64. Thoumas D, Leroi AM, Mauillon J, Muller JM, BenozioM, Dennis P, Freger P: Pudendal neuralgia: CT-guided pu-
68. Wheeler AH, Goolkasian P, Gretz SS: Botulinum toxin A
dendal nerve block technique. Abdom Imaging 24:309-312,
for the treatment of chronic neck pain. Pain 94:255-260,
HITESH GUPTA MPH (UNC-USA), M.Phil (BITS-Pilani), Ph.D (BITS-Pilani) Project Director of HIV/AIDS programme for Long Distance Truck Drivers for last three years at Project Implementation Unit (PIU) working at Jaipur as part of the Kavach project, under the Umbrella of Avaahan. The Primary Objective of the project is to arrest the growth of HIV/AIDS among long distance truckers by cr
Case Report: An 82 year old male with diffuse infiltrating glioblastoma multiforma remains in remission eleven months after initial surgical debulking and treatment with a patented herbal formula. LaRochelle, Paul Jay, MDCM, FRCS[c], FAAOS Abstract An eighty-two year old severely diabetic male presented to the emergency room with aphasia and right sided weakness on January
 the second injection 100 units of botulinum A in 3 mL0.25% bupivacaine was injected on a separate occasion.
the second injection 100 units of botulinum A in 3 mL0.25% bupivacaine was injected on a separate occasion.