Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
1klei.oa
Absence of an Effect of Liposuction on Insulin Action
and Risk Factors for Coronary Heart Disease
Samuel Klein, M.D., Luigi Fontana, M.D., Ph.D., V. Leroy Young, M.D., Andrew R. Coggan, Ph.D., Charles Kilo, M.D.,
Bruce W. Patterson, Ph.D., and B. Selma Mohammed, M.D., Ph.D. b a c k g r o u n d
Liposuction has been proposed as a potential treatment for the metabolic complica- From the Center for Human Nutrition,
Washington University School of Medicine,
tions of obesity. We evaluated the effect of large-volume abdominal liposuction on St. Louis (S.K., L.F., V.L.Y., A.R.C., C.K.,
metabolic risk factors for coronary heart disease in women with abdominal obesity.
B.W.P., B.S.M.); and the Division of FoodScience, Human Nutrition and Health, Isti-tuto Superiore di Sanità Rome, Rome (L.F.).
We evaluated the insulin sensitivity of liver, skeletal muscle, and adipose tissue (with Washington University School of Medi-a euglycemic–hyperinsulinemic clamp procedure and isotope-tracer infusions) as well cine, 660 South Euclid Ave., Campus Box
as levels of inflammatory mediators and other risk factors for coronary heart disease in15 obese women before and 10 to 12 weeks after abdominal liposuction. Eight of the N Engl J Med 2004;350:2549-57. women had normal glucose tolerance (mean [±SD] body-mass index, 35.1±2.4), and Copyright 2004 Massachusetts Medical Society. seven had type 2 diabetes (body-mass index, 39.9±5.6).
Liposuction decreased the volume of subcutaneous abdominal adipose tissue by 44 per-cent in the subjects with normal glucose tolerance and 28 percent in those with diabetes;those with normal oral glucose tolerance lost 9.1±3.7 kg of fat (18±3 percent decreasein total fat, P=0.002), and those with type 2 diabetes lost 10.5±3.3 kg of fat (19±2 per-cent decrease in total fat, P<0.001). Liposuction did not significantly alter the insulinsensitivity of muscle, liver, or adipose tissue (assessed by the stimulation of glucosedisposal, the suppression of glucose production, and the suppression of lipolysis,respectively); did not significantly alter plasma concentrations of C-reactive protein,interleukin-6, tumor necrosis factor a, and adiponectin; and did not significantly affectother risk factors for coronary heart disease (blood pressure and plasma glucose, insulin,and lipid concentrations) in either group. c o n c l u s i o n s
Abdominal liposuction does not significantly improve obesity-associated metabolic ab-normalities. Decreasing adipose tissue mass alone will not achieve the metabolic ben-efits of weight loss.
Downloaded from www.nejm.org by EARL J. MASON MD PHD on August 13, 2005 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
(waist circumference, blood pressure, plasma lipid
increased waist circumference, increased concentrations, and serum markers of inflamma-
a abdominal subcutaneous fat, and in- tion) in women with abdominal obesity. Obese
creased visceral fat, is associated with insulin resis- women with normal glucose tolerance and thosetance and other metabolic risk factors for coronary with type 2 diabetes were studied to assess the po-heart disease.1 Although both the abdominal sub- tential beneficial effects of liposuction in personscutaneous fat mass and the visceral fat mass are as- with moderate or severe insulin resistance. sociated with insulin resistance,2 it is not knownwhether one or both of these fat depots are actually
involved in the pathogenesis of insulin resistance or whether they are simply associated with the meta- subjects bolic complications of obesity.
We studied eight women with abdominal obesity
Diet-induced weight loss improves the metabol- (waist circumference, more than 100 cm) who had
ic complications of abdominal obesity. However, normal oral glucose tolerance but moderate insulinsuccessful long-term weight management is diffi- resistance (mean [±SD] age, 42±3 years) and sevencult to achieve, and the majority of obese persons women with abdominal obesity who had type 2 dia-who lose weight by implementing lifestyle changes betes and more severe insulin resistance (age, 52±3regain their lost weight over time.3 Frustration with years). The women with type 2 diabetes were beingthe efficacy of current obesity therapies has led to treated with a combination of two or three oral hypo-increased interest in alternative approaches. Recent- glycemic medications (glipizide, glyburide, glime-ly, it has been suggested that liposuction, which piride, rosiglitazone, pioglitazone, or metformin). can remove large amounts of body fat, is a poten- They were consecutive eligible patients who weretial treatment for the metabolic complications of scheduled to undergo large-volume liposuction per-obesity.4-7
formed by one of the authors and were enrolled
Liposuction, also known as lipoplasty or suction- between November 2001 and March 2003. No evi-
assisted lipectomy, is the most common aesthetic dence of other serious illnesses or organ dysfunc- surgical procedure performed in the United States; tion was found after the subjects had completed a nearly 400,000 procedures are performed annual- comprehensive medical evaluation, which includ- ly.8 Recent advances in liposuction techniques now ed a history and physical examination, electrocardi- make it possible to remove considerable amounts ography, standard blood and urine tests, and a two- of subcutaneous adipose tissue.9 Therefore, abdom- hour oral glucose-tolerance test. All the subjects had inal liposuction provides a unique opportunity to had a stable weight (with fluctuations of not more evaluate the importance of subcutaneous abdomi- than 2 percent of the body weight) for at least two nal fat in the pathogenesis of insulin resistance and months and had been sedentary (exercising for less in the risk of coronary heart disease in persons with than one hour per week) for at least six months be- abdominal obesity. However, the metabolic effects fore entering the study. Each subject provided writ- of liposuction are unclear because the results of ten informed consent before participating, and the studies have varied.5-7,10,11 The interpretation of study was approved by the human studies commit- data from such studies is confounded by lifestyle tee of Washington University School of Medicine, and weight changes that occurred among the sub- St. Louis. jects after liposuction was performed, by variations in the volume of adipose tissue removed and the site study design of its removal, by differences in the methods used Assessments of Body Composition to assess insulin sensitivity, and by differences in the Each subject’s body composition was assessed with- subjects’ baseline weight and insulin sensitivity.
in nine days before liposuction. Total body fat and
The purpose of the present study was to deter- fat-free mass were determined by dual-energy x-ray
mine the effect of large-volume abdominal liposuc- absorptiometry (Hologic QDR 1000/w). Abdomi-tion on insulin sensitivity in liver, skeletal muscle, nal and thigh fat masses were quantified by meansand adipose tissue (evaluated with the use of a two- of magnetic resonance imaging (Siemens). Eightstage euglycemic–hyperinsulinemic clamp proce- 10-mm-thick slice images were obtained both atdure, in conjunction with stable isotope-tracer infu- the L4–L5 interspace and at the superior border ofsions) and on risk factors for coronary heart disease the medial condyle of the tibia and were analyzed
Downloaded from www.nejm.org by EARL J. MASON MD PHD on August 13, 2005 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
l i p o s u c t i o n a n d m e t a b o l i c a b n o r m a l i t i e s
for subcutaneous and intracompartmental (abdo- for evaluating the effect of insulin on glucose pro-men or muscle) fat content.
duction and lipolysis (stage 1) and on glucose dis-posal (stage 2). The rates of tracer infusions were
Euglycemic–Hyperinsulinemic Clamp Protocol
decreased during each stage of the clamp protocol
The subjects were admitted to the General Clinical to account for the expected changes in endogenousResearch Center (Washington University School of substrate metabolism. Blood samples were obtainedMedicine) and consumed a standard meal (55 per- before the beginning of the tracer infusion to deter-cent carbohydrate, 30 percent fat, and 15 percent mine baseline plasma concentrations of C-reactiveprotein) containing 16 kcal per kilogram of fat-free protein, cytokines, lipids, substrates, and hormonesmass at 7 p.m. At 8 p.m., they consumed a 240-kcal and to determine background substrate tracer-to-liquid snack (Ensure, Ross Laboratories). The last tracee ratios. Blood was collected every 10 minutesdose of hypoglycemic medication was taken on the during the last 30 minutes of the basal period andday of admission. At 5 a.m. the next morning, after during the last 30 minutes of each stage of the eu-the subjects had fasted overnight, catheters were in- glycemic–hyperinsulinemic clamp procedure toserted into a radial artery for blood sampling and determine plasma substrate and insulin concentra-into an antecubital vein for the infusion of insulin, tions and substrate tracer-to-tracee ratios (i.e., thedextrose, and tracers. At 7 a.m., a primed (priming ratios of labeled to unlabeled substrate in plasma). dose, 4.1 mg per kilogram [22.5 µmol per kilo- Plasma was separated by centrifugation within 30gram]), constant infusion of [6,6-2H ]glucose minutes after collection and stored at ¡70°C until
(0.46 mg per minute per kilogram [0.25 µmol per final analyses were performed. minute per kilogram]) was started, followed at9 a.m. by a primed (priming dose, 116 µg per kilo- Liposuctiongram [1.2 µmol per kilogram]), constant infusion Approximately one week after completing the eu-of [1,1,2,3,3-2H ]glycerol (7.8 µg per minute per glycemic–hyperinsulinemic clamp procedure, each
kilogram [0.08 µmol per minute per kilogram]) and subject underwent large-volume tumescent liposuc-a constant infusion of [2,2-2H ]palmitate (9.0 µg tion, defined as the removal of more than 4 liters of
per minute per kilogram [0.035 µmol per minute aspirate.12 This procedure involves subcutaneousper kilogram]).
injection of a large volume of Ringer’s lactate con-
After infusion of the tracer for 3.5 hours (the taining dilute epinephrine (1:1,000,000) to induce
basal period), a two-stage euglycemic–hyperinsu- vasoconstriction and thus to minimize bleeding. Alllinemic clamp protocol was initiated and continued liposuction procedures were performed by one offor 6 hours. Euglycemia (a glucose level of approxi- the authors, who primarily removed superficialmately 100 mg per deciliter [5.6 mmol per liter]) and deep subcutaneous abdominal fat. In addition,was maintained by variable-rate infusion of 20 per- smaller amounts of fat were removed from the arms,cent dextrose containing approximately 2.5 percent flanks, hips, or thighs in five subjects without dia-[6,6-2H ]glucose. During stage 1 of the clamp betes and in four subjects with diabetes. A total of
protocol (from hour 3.5 to hour 6.5 of the tracer- 16±1 liters (12±1 liters from the upper body andinfusion study), insulin was infused at a rate of 4±2 liters from the lower body) of Ringer’s lactate20 mU per square meter of body-surface area per plus epinephrine-infiltrated adipose tissue was as-minute after initiation by a two-step priming dose pirated from the subjects with normal oral glucoseof insulin for 10 minutes (80 mU per square meter tolerance and a total of 17±2 liters (16±2 liters fromper minute for 5 minutes, followed by 40 mU per the upper body and 1±1 liters from the lower body)square meter per minute for 5 minutes). During was aspirated from the subjects with type 2 diabetes. stage 2 of the clamp protocol (hour 6.5 to hour 9.5of the tracer-infusion study), insulin was infused at Evaluation after Liposuctiona rate of 50 mU per square meter per minute after Subjects were instructed to resume their normalinitiation by a two-step priming dose of insulin for lifestyle after the initial recovery period and to weigh10 minutes (200 mU per square meter per minute themselves weekly at home. Each subject was con-for 5 minutes, followed by 100 mU per square meter tacted by one of the investigators at least once everyper minute for 5 minutes).
week by phone to review her medical condition and
These insulin infusion rates result in plasma in- to reinforce the importance of maintaining her
sulin concentrations that provide an optimal range usual food intake and physical activity and to main-
Downloaded from www.nejm.org by EARL J. MASON MD PHD on August 13, 2005 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
tain a stable body weight. No serious complications without diabetes were analyzed separately. A two-occurred in any subject, and all were able to return way analysis of variance (time by clamp stage) withto their usual lifestyle within 10 days after liposuc- repeated measures was used to compare the effectstion. For each of the seven subjects with type 2 dia- of liposuction on basal and insulin-mediated sub-betes, hypoglycemic medications were regulated strate metabolism. Changes in body compositionby the subject’s physician. In six of them, the medi- and risk factors for coronary heart disease werecations were not changed after the clamp procedure; assessed by means of Student’s t-test for pairedin one, rosiglitazone (4 mg per day) was stopped, samples. All reported P values are two-sided, and aand glipizide and metformin were continued.
P value of 0.05 or less was considered to indicate
All the studies performed before liposuction statistical significance.
were repeated 10 to 12 weeks after liposuction. The10-to-12-week delay was intended to eliminate the
confounding effects of postsurgical inflammationon our study end points. b o d y c o m p o s i t i o n
Liposuction decreased body weight and body-mass
a n a l y s e s o f b l o o d s a m p l e s
index (the weight in kilograms divided by the square
Plasma glucose concentrations were determined of the height in meters) because of a marked de-with use of a glucose analyzer (Yellow Springs In- crease in body fat (Table 1). Ten to 12 weeks afterstruments), and plasma fatty acid concentrations surgery, the mass of body fat had decreased bywere quantified by means of gas chromatography.13 9.1±3.7 kg from baseline (18±3 percent of the totalPlasma insulin and leptin concentrations were mea- fat mass, P=0.002) in the subjects with normal oralsured by radioimmunoassay (Linco Research). glucose tolerance and by 10.5±3.3 kg (19±2 per-Plasma lipid concentrations were determined enzy- cent of the total fat mass, P<0.001) in the subjectsmatically (Roche/Hitachi 747 Analyzer, Roche Di- with type 2 diabetes. The decrease in measured fatagnostics). Enzyme-linked immunosorbent assay mass was consistent with the amount of fat aspi-kits were used to measure plasma C-reactive pro- rated during liposuction; approximately 60 percenttein (American Laboratory Products), adiponectin of the liposuction aspirate was composed of fat. (B-Bridge International), interleukin-6, and tumor The decrease in body fat was greater than the totalnecrosis factor a (Quantakine High Sensitive, R&D decrease in body weight, however, because of ab-Systems). Plasma glucose, glycerol, and palmitate dominal-tissue edema, which often persists fortracer-to-tracee ratios were determined with the use months after liposuction.16 The measured truncalof gas chromatography–mass spectrometry.13,14
fat-free mass, which included tissue fluid, increasedfrom 24.5±2.7 kg to 27.4±3.0 kg (P<0.001) in the
c a l c u l a t i o n s
two groups overall. Liposuction decreased the vol-
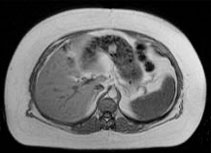
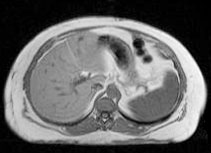
A physiologic and isotopic steady state was achieved ume of subcutaneous abdominal adipose tissue by during the last 30 minutes of the basal period and 44 percent in the subjects with normal glucose toler- the insulin-infusion period, so the rates of appear- ance and 28 percent in those with diabetes, where- ance and disappearance of substrate were calculat- as the volumes of visceral adipose tissue and thigh ed as the tracer infusion rate divided by the tracer- adipose tissue did not change significantly (Fig. 1 to-tracee ratio.15 The rate of appearance of total and Table 1). free fatty acid was calculated by dividing the rate of appearance of palmitate by the percent contribu- circulating inflammatory mediators tion of palmitate to total plasma free fatty acids. a n d o t h e r r i s k f a c t o r s f o r c o r o n a r y h e a r t d i s e a s e s t a t i s t i c a l a n a l y s i s
Liposuction caused a decrease in waist circumfer-
The number of subjects to be enrolled was deter- ence in both groups, but it did not significantly altermined as the estimated number needed for the study other risk factors for coronary heart disease (Tableto detect a statistically significant effect of liposuc- 2). Liposuction also decreased plasma leptin con-tion on glucose kinetics with a power of at least 0.8, centrations in both groups, but it did not signifi-if the subjects had lost a similar amount of body fat cantly alter the concentrations of other circulatingby dieting. Data on subjects with diabetes and those cytokines or of C-reactive protein (Table 3).
Downloaded from www.nejm.org by EARL J. MASON MD PHD on August 13, 2005 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
l i p o s u c t i o n a n d m e t a b o l i c a b n o r m a l i t i e s
Table 1. Effects of Liposuction on Body Composition in Obese Women with Normal Glucose Tolerance or Type 2 Diabetes.* Variable Normal Glucose Tolerance (N=8) Type 2 Diabetes (N=7)
1895±778 –1519 (–1977 to –1061) <0.001
* Plus–minus values are means ±SD. Body-composition studies were performed within 9 days before liposuction and were repeated 10 to 12
weeks after liposuction. CI denotes confidence interval, minus signs decreases, and plus signs increases. s u b s t r a t e k i n e t i c s a n d i n s u l i n s e n s i t i v i t y
risk factors for coronary heart disease in women
In the subjects with normal glucose tolerance, plas- with abdominal obesity who had either moderatema insulin concentrations after liposuction were insulin resistance and normal glucose tolerance orsimilar to those before liposuction for both stages more severe insulin resistance and type 2 diabetes. 1 and 2 of the clamp procedure (stage 1 and 2 values Weight stability was carefully maintained beforebefore liposuction, 44±7 and 90±12 µU per millili- and after liposuction to eliminate the confoundingter [264±42 and 540±72 pmol per liter], respective- effects of changes in energy balance on the studyly; stage 1 and 2 values after liposuction, 42±5 and end points. Our data show that the aspiration of89±6 µU per milliliter [252±30 and 534±48 pmol large amounts of subcutaneous abdominal adiposeper liter], respectively); the same was true of the tissue resulted in a considerable decrease in bodysubjects with type 2 diabetes (stage 1 and 2 values weight, waist circumference, and plasma leptin con-before liposuction, 40±2 and 86±7 µU per milliliter centrations but did not have a significant effect on[240±12 and 516±42 pmol per liter], respectively;stage 1 and 2 values after liposuction, 41±3 and86±6 µU per milliliter [246±18 and 516±36 pmolper liter], respectively). Insulin infusion duringstage 1 caused the expected decreases in the rates ofappearance of glucose, glycerol, and free fatty acids,
Liposuction
and insulin infusion during stage 2 caused the ex-pected increase in the rate of disappearance of glu-cose both in subjects with normal glucose toleranceand in those with type 2 diabetes (Fig. 2 and 3). Rates of appearance of glucose, glycerol, and freefatty acid and the rate of disappearance of glucose
during basal conditions and during each stage of
Liposuction
the clamp procedure were not significantly differ-ent before and after liposuction in either group(Fig. 2 and 3). Figure 1. Photographs and Abdominal Magnetic Resonance Images Obtained before and after Liposuction.
The photographs of one study subject and images of another show the large
In the present study, we evaluated the effects of
amount of subcutaneous abdominal fat removed by liposuction.
large-volume liposuction on insulin sensitivity and
Downloaded from www.nejm.org by EARL J. MASON MD PHD on August 13, 2005 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
Table 2. Effects of Liposuction on Risk Factors for Coronary Heart Disease in Obese Women with Normal Glucose Tolerance or Type 2 Diabetes.* Variable Normal Glucose Tolerance (N=8) Type 2 Diabetes (N=7)
Liposuction Liposuction Change (95% CI) Value
* Plus–minus values are means ±SD. To convert the values for glucose to millimoles per liter, multiply by 0.0555. To convert the values for insu-
lin to picomoles per liter, multiply by 6. To convert the values for cholesterol to millimoles per liter, multiply by 0.0259. To convert the values for triglycerides to millimoles per liter, multiply by 0.0113. The measurements were made within 9 days before liposuction and again 10 to 12 weeks after liposuction. CI denotes confidence interval, minus signs decreases, and plus signs increases. Table 3. Effects of Liposuction on Mediators of Inflammation in Obese Women with Normal Glucose Tolerance or Type 2 Diabetes.* Variable Normal Glucose Tolerance (N=8) Type 2 Diabetes (N=7)
Value Liposuction Liposuction Change (95% CI) Value
Tumor necrosis factor a (pg/ml) 3.5±5.8
* Plus–minus values are means ±SD. The measurements were made within 9 days before liposuction and again 10 to 12 weeks after liposuc-
tion. CI denotes confidence interval, minus signs decreases, and plus signs increases.
† Values were obtained from six subjects in each group.
insulin sensitivity in skeletal muscle (assessed as subjects is equivalent to the weight loss achieved bythe stimulation of glucose uptake), in the liver (as- optimal behavioral and pharmacologic treatments.3sessed as the suppression of glucose production), A total weight loss of approximately 12 percent ofor adipose tissue (assessed as the suppression of body weight would be required to achieve the fatlipolysis). In addition, liposuction had no signifi- loss resulting from liposuction in our study sub-cant effects on other risk factors for coronary heart jects, because about 75 percent of the decrease indisease, including blood pressure; fasting plasma body-mass that occurs by dieting is due to loss ofglucose, insulin, and lipid concentrations; and con- body fat.17 This amount of weight loss usually re-centrations of plasma markers of inflammation sults in marked improvement in the metabolic ab-and insulin resistance (C-reactive protein, tumor normalities associated with obesity and improvesnecrosis factor a, interleukin-6, and adiponectin).
insulin sensitivity,18 blood pressure,19 and concen-
The amount of fat removed by liposuction in our trations of serum lipids20 and circulating markers
Downloaded from www.nejm.org by EARL J. MASON MD PHD on August 13, 2005 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
l i p o s u c t i o n a n d m e t a b o l i c a b n o r m a l i t i e s
(µmol/min) Disappearance of Glucose Appearance of Glucose (µmol/min) (µmol/min) Appearance of Free Fatty Acids Appearance of Glycerol (µmol/min) Figure 2. Mean Rates of Appearance and Disappearance of Glucose and Rates of Appearance of Glycerol and Free Fatty Acids in the Basal State and during the Euglycemic–Hyperinsulinemic Clamp Procedure in Obese Women with Normal Glucose Tolerance before and after Liposuction.
Stage 1 of the euglycemic–hyperinsulinemic clamp procedure involved the infusion of insulin at a rate of 20 mU per square meter of body-surface area per minute, and stage 2 involved the infusion of insulin at a rate of 50 mU per square meter per minute. The T bars represent the SD.
of inflammation.21 Therefore, it is striking that the cutaneous abdominal fat and reduces the totalamount of fat loss achieved by liposuction in our number of body fat cells, without altering visceraldiabetic and nondiabetic subjects did not improve fat mass,31 the size of the remaining fat cells,10 in-any of these metabolic variables.
tramyocellular fat, or intrahepatic fat.
The absence of an apparent therapeutic effect of
The results of the present study also show that
liposuction provides insight into the mechanism by removing a large amount of abdominal subcutane-which conventional therapy for obesity — namely, ous fat by liposuction does not significantly affectdiet, pharmacotherapy, and bariatric surgery — im- the levels of circulating mediators of inflammationproves insulin sensitivity. Our results suggest that that are probably involved in the development ofinduction of a negative energy balance, not simply insulin resistance and coronary heart disease.32 Ad-a decrease in the mass of adipose tissue, is critical ipose tissue is now recognized as an importantfor achieving the metabolic benefits of weight loss. endocrine organ that produces several bioactive pro-Even small amounts of weight loss induced by a teins, including interleukin-6, tumor necrosis fac-negative energy balance affects many variables per- tor a, and adiponectin. Interleukin-6 and tumortaining to body-fat composition and lipid metab- necrosis factor a can cause insulin resistance andolism — variables that probably contribute to the atherosclerosis by impairing insulin signaling, stim-metabolic abnormalities associated with obesi- ulating lipolysis and fatty acid release, increasingty.22-25 Weight loss decreases visceral fat mass,26 hepatic synthesis of C-reactive protein, and increas-intramyocellular fat,27 intrahepatic fat,28 fat-cell ing systemic inflammation,32-34 whereas the pro-size,29 and the rate of release of fatty acids from adi- duction of adiponectin by adipose tissue can im-pose tissue.30 In contrast, liposuction removes sub- prove insulin sensitivity and inhibit vascular
Downloaded from www.nejm.org by EARL J. MASON MD PHD on August 13, 2005 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
The new england journal of medicine
(µmol/min) Disappearance of Glucose Appearance of Glucose (µmol/min) (µmol/min) Appearance of Free Fatty Acids Appearance of Glycerol (µmol/min) Figure 3. Mean Rates of Appearance and Disappearance of Glucose and Rates of Appearance of Glycerol and Free Fatty Acids in the Basal State and during the Euglycemic–Hyperinsulinemic Clamp Procedure in Obese Women with Diabetes before and after Liposuction.
Stage 1 of the euglycemic–hyperinsulinemic clamp procedure involved the infusion of insulin at a rate of 20 mU per square meter of body-surface area per minute, and stage 2 involved the infusion of insulin at a rate of 50 mU per square meter per minute. The T bars represent the SD.
inflammation.35,36 Fat loss achieved by convention- improve insulin sensitivity in the liver, skeletal mus-al obesity treatments decreases the plasma concen- cle, or adipose tissue; serum concentrations oftrations of C-reactive protein, interleukin-6, and markers of inflammation; or other risk factors fortumor necrosis factor a37,38 and increases the con- coronary heart disease. These findings offer impor-centration of adiponectin39; in contrast, liposuction tant insights into the mechanisms responsible forin our subjects did not significantly change the the metabolic benefits observed with moderate diet-plasma concentrations of any of these markers. induced weight loss, which decreases hepatic andHowever, fat removal by liposuction did decrease muscle fat content, fat-cell size, visceral fat mass,the plasma leptin concentration, which is a marker and circulating concentrations of proinflammatoryof adipose-tissue mass.40 These results suggest that cytokines. The effects of a negative energy balancea negative energy balance influences adipocyte and on specific endogenous triglyceride depots and in-monocyte activation and the gene expression of flammation, which are not altered by liposuction,selected cytokines, but that long-term leptin pro- may be necessary to achieve many of the clinicalduction is influenced primarily by total fat mass.
The results of the present study suggest that ab-
Supported by grants (HD 01459, DK 37948, RR-00954 [to the Bio-
medical Mass Spectrometry Resource], RR-00036 [to the General
dominal liposuction should not, by itself, be con- Clinical Research Center], and DK 56341 [to the Clinical Nutritionsidered a clinical therapy for obesity. Aspiration of Research Unit]) from the National Institutes of Health. large amounts of subcutaneous abdominal fat in
We are indebted to the nursing staff of the General Clinical Re-
search Center for their help in performing the studies, to Freida
women with abdominal obesity may have cosmetic Custodio and Junyoung Kwon for their technical assistance, and tobenefits, but the procedure does not significantly the subjects for their participation in the study.
Downloaded from www.nejm.org by EARL J. MASON MD PHD on August 13, 2005 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
l i p o s u c t i o n a n d m e t a b o l i c a b n o r m a l i t i e s
r e f e r e n c e s
SC, Kelley DE. Intramuscular lipid content
et al. Relation of body fat distribution to
metabolic complications of obesity. J Clin
15. Steele R. Influences of glucose loading
weight loss. Metabolism 2000;49:467-72.
and of injected insulin on hepatic glucose
28. Tiikkainen M, Bergholm R, Vehkavaara
output. Ann N Y Acad Sci 1959;82:420-30.
S, et al. Effects of identical weight loss on
16. Mladick RA. Lipoplasty of the calves and
body composition and features of insulin re-
generalized and regional adiposity to insu-
ankles. Plast Reconstr Surg 1990;86:84-93.
sistance in obese women with high and low
lin sensitivity in men. J Clin Invest 1995;96:
17. Ballor DL, Poehlman ET. Exercise-train-
liver fat content. Diabetes 2003;52:701-7. 29. Knittle JL, Ginsberg-Fellner F. Effect of
weight reduction on in vitro adipose tissue
technical review on obesity. Gastroenterol-
analytical finding. Int J Obes Relat Metab
lipolysis and cellularity in obese adolescents
and adults. Diabetes 1972;21:754-61. 18. Uusitupa M, Lindi V, Louheranta A, Sa- 30. Klein S, Luu K, Gasic S, Green A. Effect
lopuro T, Lindstrom J, Tuomilehto J. Long-
of weight loss on whole body and cellular
term improvement in insulin sensitivity by
lipid metabolism in severely obese humans.
changing lifestyles of people with impaired
glucose tolerance: 4-year results from the
31. Matarasso A, Kim RW, Kral JG. The im-
Martinez-Abundis E. The effects of surgical-
Finnish Diabetes Prevention Study. Diabetes
pact of liposuction on body fat. Plast Recon-
ly removing subcutaneous fat on the meta-
bolic profile and insulin sensitivity in obese
19. Stevens VJ, Obarzanek E, Cook NR, et al. 32. Ahima RS, Flier JS. Adipose tissue as an
women after large-volume liposuction treat-
blood pressure: results of the Trials of Hy-
pertension Prevention, phase II. Ann Intern
33. Kern PA, Ranganathan S, Li C, Wood L,
Spear SL, Yanovski JA. Improvements in car-
diovascular risk profile with large-volume
20. Dattilo AM, Kris-Etherton PM. Effects of
crosis factor and interleukin-6 expression in
liposuction: a pilot study. Plast Reconstr
weight reduction on blood lipids and lipo-
human obesity and insulin resistance. Am J
proteins: a meta-analysis. Am J Clin Nutr
PF. Effect of large-volume liposuction on sex
21. Ziccardi P, Nappo F, Giugliano G, et al. 34. Yudkin JS, Kumari M, Humphries SE,
lism in females. Aesthetic Plast Surg 1995;
centrations and improvement of endothelial
stress and coronary heart disease: is inter-
functions in obese women after weight loss
leukin-6 the link? Atherosclerosis 2000;148:
over one year. Circulation 2002;105:804-9.
Plastic Surgery. Cosmetic Surgery National
22. Boden G, Shulman GI. Free fatty acids 35. Ouchi N, Kihara S, Arita Y, et al. Adi-
Data Bank 2002 statistics. (Accessed April
in obesity and type 2 diabetes: defining their
ponectin, an adipocyte-derived plasma pro-
20, 2004, at http://www.surgery.org/press/
role in the development of insulin resistance
tein, inhibits endothelial NF-kB signaling
and beta-cell dysfunction. Eur J Clin Invest
Large-volume liposuction: a review of 631
23. Krssak M, Falk Petersen K, Dresner A, et 36. Okamoto Y, Kihara S, Ouchi N, et al. Ad-
consecutive cases over 12 years. Plast Re-
al. Intramyocellular lipid concentrations are
iponectin reduces atherosclerosis in apolipo-
correlated with insulin sensitivity in humans:
protein E-deficient mice. Circulation 2002;
10. Lambert EV, Hudson DA, Bloch CE,
a 1H NMR spectroscopy study. Diabetologia
Koeslag JH. Metabolic response to localized
1999;42:113-6. [Errata, Diabetologia 1999;
37. Esposito K, Pontillo A, Di Palo C, et al.
surgical fat removal in nonobese women.
Effect of weight loss and lifestyle changes
Aesthetic Plast Surg 1991;15:105-10. 24. Seppala-Lindroos A, Vehkavaara S, Hak-
on vascular inflammatory markers in obese
11. Berntorp E, Berntorp K, Brorson H,
kinen AM, et al. Fat accumulation in the liver
Frick K. Liposuction in Dercum’s disease:
is associated with defects in insulin sup-
38. Dandona P, Weinstock R, Thusu K,
with cardiovascular disease and insulin sen-
free fatty acids independent of obesity in
sitivity. J Intern Med 1998;243:197-201.
normal men. J Clin Endocrinol Metab 2002;
mor necrosis factor-alpha in sera of obese
12. Trott SA, Beran SJ, Rohrich RJ, Kenkel
patients: fall with weight loss. J Clin Endo-
JM, Adams WP Jr, Klein KW. Safety consid-
25. Weyer C, Foley JE, Bogardus C, Tataran-
erations and fluid resuscitation in liposuc-
39. Yang WS, Lee WJ, Funahashi T, et al.
tion: an analysis of 53 consecutive patients.
abdominal adipocyte size, but not obesity it-
Weight reduction increases plasma levels of
Plast Reconstr Surg 1998;102:2220-9.
self, predicts type II diabetes independent of
an adipose-derived anti-inflammatory pro-
13. Horowitz JF, Coppack SW, Paramore D,
insulin resistance. Diabetologia 2000;43:
tein, adiponectin. J Clin Endocrinol Metab
Cryer PE, Zhao G, Klein S. Effect of short-
term fasting on lipid kinetics in lean and
26. Purnell JQ, Kahn SE, Albers JJ, Nevin 40. Considine RV, Sinha MK, Heiman ML,
weight loss with reduction of intra-abdomi-
14. Horowitz JF, Coppack SW, Klein S.
nal fat on lipid metabolism in older men.
Whole body and adipose tissue glucose me-
J Clin Endocrinol Metab 2000;85:977-82.
humans. N Engl J Med 1996;334:292-5.
tabolism in response to short-term fasting
27. Goodpaster BH, Theriault R, Watkins Copyright 2004 Massachusetts Medical Society.
Downloaded from www.nejm.org by EARL J. MASON MD PHD on August 13, 2005 .
Copyright 2004 Massachusetts Medical Society. All rights reserved.
Psychoneuroendocrinology (2004) 29, 1341–1344Effects of PhD examination stress onallopregnanolone and cortisol plasma levels andperipheral benzodiazepine receptor densityHal A. Droogleever Fortuyna, Frank van Broekhovena,*, Paul N. Spanb,Torbjo¨mc, Frans G. Zitmana,1, Robbert J. VerkesaaUnit for Clinical Psychopharmacology and Neuropsychiatry, 331 Department of Psychiatry,University Medical
L’ús social del valencià. Antecedents ¿El valencià va avant, el valencià va arrere? Quin és l’ús social del valencià a començaments del segle XXI? Per a intentar respondre a eixa pregunta sense paréixer que estiguem ballant la yenka, segons l’estat d’ànim de cada moment, em permetran que em remeta a l’anàlisi d’una època que a mi m’ha ajudat molt a comprendre la situac


 l i p o s u c t i o n a n d m e t a b o l i c a b n o r m a l i t i e s
Table 1. Effects of Liposuction on Body Composition in Obese Women with Normal Glucose Tolerance or Type 2 Diabetes.*
l i p o s u c t i o n a n d m e t a b o l i c a b n o r m a l i t i e s
Table 1. Effects of Liposuction on Body Composition in Obese Women with Normal Glucose Tolerance or Type 2 Diabetes.*

 The new england journal of medicine
(µmol/min)
The new england journal of medicine
(µmol/min)