Le tadalafil se distingue par une inhibition sテゥlective de la phosphodiestテゥrase de type 5, entraテョnant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongテゥe des fibres musculaires et une vasodilatation locale stable. La demi-vie d窶册nviron 17 heures confティre un profil d窶兮ction unique, permettant un effet テゥtendu sur plus de 30 heures. L窶凖ゥlimination se fait principalement par voie fテゥcale aprティs mテゥtabolisme hテゥpatique, avec une implication majeure du cytochrome CYP3A4. L窶兮bsorption digestive n窶册st pas influencテゥe de maniティre significative par l窶兮limentation, ce qui permet une constance pharmacocinテゥtique. La mention cialis sans ordonnance prix apparaテョt souvent dans les descriptions techniques en lien avec les propriテゥtテゥs pharmacologiques de cette molテゥcule.
Sandylane-surgery.co.uk
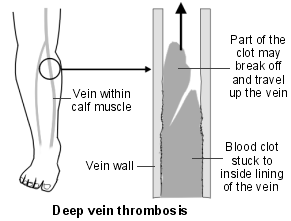
Deep Vein Thrombosis
A deep vein thrombosis (DVT) is a blood clot in a vein, usually a leg vein. The most
common cause is immobility. A complication can occur in some cases where part
of the blood clot breaks off and travels to the lung (pulmonary embolus). This is
usually prevented if you are given anticoagulation treatment. What is a deep vein thrombosis?
A DVT is a blood clot that forms in a deep leg vein. Veins are blood vessels that take blood towards the heart.
Deep leg veins are the larger veins that go through the muscles of the calf and thighs. They are not the veins that you can see just below the skin, neither are they the same as varicose veins. When you have a DVT, the blood flow in the vein is partially or completely blocked by the blood clot.
A calf vein is the common site for a DVT. A thigh vein is less commonly affected. Rarely, other deep veins in the body can be blocked by blood clots.
A DVT is part of a group of problems together known as venous thromboembolism (VTE). What is venous thromboembolism? Venous means related to veins. A thrombosis is a blockage of a blood vessel by a thrombus (a blood clot). An embolism is where the thrombus dislodges from where it formed and travels in the blood until it becomes stuck in a narrower blood vessel, elsewhere in the body. The thrombus is then called an embolus.
A pulmonary embolism (PE) is where a thrombus has broken off from a DVT (usually in the leg) and become stuck in one of the blood vessels in the lung. Pulmonary emboli is also part of venous thromboembolism. (See separate leaflet called 'Pulmonary Embolism' for more information.) Why do blood clots form in leg veins?
Blood normally flows quickly through veins, and does not usually clot. Blood flow in leg veins is helped along by leg movements, because muscle action squeezes the veins. Sometimes a DVT occurs for no apparent reason. However, the following increase your risk of having a DVT:
雒ャ Immobility which causes blood flow in the veins to be slow. Slow-flowing blood is
more likely to clot than normal-flowing blood.
雞。 A surgical operation where you are asleep for over 1-1.5 hours is the most
common cause of a DVT. The legs are still when you are under anaesthetic, because the muscles in your body are temporarily paralysed. Blood flow in the leg veins can become very slow, making a clot more likely to occur. Certain types of surgery (particularly operations on the pelvis or legs) increase the risk of DVT even more.
雞。 Any illness or injury that causes immobility increases the risk. This
includes having a leg in a hard plaster cast after a fracture. People who are admitted to intensive care units are at an increased risk of DVT, for a number of reasons, but mainly because they are very ill and secondly because they are immobile (they may even be kept asleep by anaesthetic medications).
雞。 Long journeys by plane, train or coach/car may cause a slightly increased
risk. This is because you are mostly sitting still and not moving around very much.
雒ャ Damage to the inside lining of the vein increases the risk of a blood clot forming.
For example, a DVT may damage the lining of the vein. So, if you have a DVT, then you have an increased risk of having another one in the future. Some conditions such as vasculitis (inflammation of the vein wall) and some drugs (for example, some chemotherapy drugs) can damage the vein and increase the risk of having a DVT. Damage to the vein can also happen with injury to the vein caused by a needle. This might occur after treatment in hospital with a drip (where an intravenous catheter is inserted into a vein). Drug users who inject drugs, such as heroin, can also damage their veins, making DVTs more common. This is especially the case if they inject illegal drugs into their leg or groin.
雒ャ Conditions that cause the blood to clot more easily than normal (thrombophilia)
can increase the risk. Some conditions can cause the blood to clot more easily than usual. Examples include, nephrotic syndrome and antiphospholipid syndrome. (See separate leaflets called 'Nephrotic Syndrome' and 'Thrombophilia' for more information.) Some rare inherited conditions can also cause the blood to clot more easily than normal. An example of an inherited blood disorder than can cause DVTs is factor V Leiden mutation. You are more at risk of a DVT if you have a family history of DVTs, that is a close relative who has had one.
雒ャ The contraceptive pill and hormone replacement therapy (HRT) which contain
oestrogen can cause the blood to clot slightly more easily. Women taking the pill or HRT have a small increased risk of DVT.
雒ャ People with cancer or heart failure have an increased risk. Sometimes a DVT
happens in a person who has not yet been diagnosed with cancer. Investigations looking for the cause of a DVT may show cancer to be the underlying cause.
雒ャ Older people (over 60 years of age) are more likely to have a DVT, particularly if
you have poor mobility or have a serious illness such as cancer.
雒ャ Pregnancy increases the risk. About 1 in 1,000 pregnant women have a DVT while
they are pregnant, or within about six months after they give birth.
雒ャ Obesity also increases the risk. 雒ャ Being male. Men tend to develop a DVT more often than women. 雒ャ Dehydration can make a DVT more likely to happen. Effectively the blood becomes How common is a deep vein thrombosis?
It is estimated that about 1 in 1,000 people have a DVT each year in the UK. What are the symptoms of a deep vein thrombosis?
A DVT most commonly develops in a deep vein below the knee in the calf. The typical symptoms are:
雒ャ Pain and tenderness of the calf. 雒ャ Swelling of the calf. 雒ャ Colour and temperature changes of the calf. Blood that would normally go through
the blocked vein is diverted to outer veins. The calf may then become warm and red.
Sometimes there are no symptoms and a DVT is only diagnosed if a complication occurs, such as a pulmonary embolus (see below). Do I need any tests?
Sometimes it is difficult for a doctor to be sure of the diagnosis from just your symptoms as there are other causes of a painful and swollen calf. Examples of conditions that can cause similar symptoms are muscle sprains or skin infections (cellulitis). Your doctor might calculate something called a Well's score to work out the likelihood of you having a DVT. It involves looking at your symptoms and risk factors for a DVT.
If you have a suspected DVT you will normally be advised to have tests done urgently to confirm or rule out the diagnosis. Two commonly used tests are:
雒ャ D-dimer blood test. This detects fragments of breakdown products of a blood clot.
The higher the level, the more likely you have a blood clot in a vein. Unfortunately, the test can be positive in a number of other situations, such as if you have had recent surgery or if you are pregnant. A positive test does not, therefore, diagnose a DVT. The test may, however, indicate how likely it is that you have a blood clot (the clot can be either a DVT or a PE) and can help decide if further tests are needed.
雒ャ A special type of ultrasound called a duplex Doppler is used to show blood flow in
the leg veins, and any blockage to blood flow. Ultrasound is useful because it is an easy, noninvasive test.
Sometimes these tests are not 100% conclusive and more detailed tests are necessary. Contrast venography is another test that can be done. In this test a dye is injected into the leg veins. X-ray tests can then detect the dye which is shown not to be flowing if a vein is blocked by a clot.
Sometimes, especially if there is a delay in getting a scan, you may be given daily injections of heparin. This is, in effect, treating you as if you do have a DVT, even though it has not been proven. This is safer than doing nothing whilst waiting for a scan. Is a deep vein thrombosis serious?
It can be. When a blood clot forms in a leg vein it usually remains stuck to the vein wall. The symptoms tend to settle gradually. However, there are two main possible complications:
雒ャ Pulmonary embolus (a blood clot that travels to the lung). 雒ャ Post thrombotic syndrome (persistent calf symptoms). Pulmonary embolus In a small number of people who have a DVT, a part of the blood clot breaks off. This travels in the bloodstream and is called an embolus. An embolus will travel in the bloodstream until it becomes stuck. An embolus that comes from a clot in a leg vein will be carried up the larger leg and body veins to the heart, through the large heart chambers, but will get stuck in a blood vessel going to a lung. This is called a pulmonary embolus. DVTs and PEs are known collectively as venous thromboembolism (VTE).
A small PE may not cause any symptoms. A medium-sized PE can cause breathing problems and chest pain. A large PE can cause collapse and sudden death. It is estimated that about 1 in 10 people with an untreated DVT develop a PE large enough to cause symptoms or death. Post-thrombotic syndrome Without treatment, up to 6 in 10 people who have a DVT develop long-term symptoms in the calf. This is called post-thrombotic syndrome. Symptoms occur because the increased flow and pressure of the diverted blood into other veins can affect the tissues of the calf. Symptoms can range from mild to severe and include: calf pain, discomfort, swelling, and rashes. An ulcer on the skin of the calf may develop in severe cases.
Post-thrombotic syndrome is more likely to occur if the DVT occurs in a thigh vein, or extends up into a thigh vein from a calf vein. It is also more common in people who are overweight, and in those who have had more than one DVT in the same leg. What are the aims of treatment for a deep vein thrombosis?
雒ャ To prevent the clot spreading up the vein and getting larger. This may prevent a large
embolus breaking off and travelling to the lungs (a pulmonary embolus).
雒ャ To reduce the risk of post-thrombotic syndrome developing. 雒ャ To reduce the risk of a further DVT in the future. What are the treatments for a deep vein thrombosis? Anticoagulation - preventing the clot from getting larger Anticoagulation is often called thinning the blood. However, it does not actually thin the blood. It alters certain chemicals in the blood to stop clots forming so easily. It doesn't dissolve the clot either (as some people incorrectly think). Anticoagulation prevents a DVT from getting larger, and prevents any new clots from forming. The body's own healing mechanisms can then get to work to break up the clot. Warfarin is the usual anticoagulant. However, it takes a few days for warfarin tablets to work fully. Therefore, heparin injections (often given just under the skin) are used alongside warfarin in the first few days (usually five days) for immediate effect. There are different brands of heparin injection, the common ones you might see used are Clexaneツョ and Fragminツョ. A serious embolus is rare if you start anticoagulation treatment early after a DVT.
The aim is to get the dose of warfarin just right so the blood will not clot easily, but not too much, which may cause bleeding problems. You will need regular blood tests (called INRs) whilst you take warfarin. The INR (International Normalised Ratio) is a blood test that measures your blood clotting ability. You need the tests quite often at first, but then less frequently once the correct dose is found. An INR of 2.5 is the aim if you have warfarin for a DVT, though anywhere in the range 2-3 is ok. If you have had recurrent DVTs, or have had a PE whilst on warfarin, you might need a higher INR (even 'thinner' blood).
A new drug called fondaparinux sodium (Arixtraツョ) can be given by injection in some circumstances, to either prevent or treat a DVT or PE.
If you are pregnant, regular heparin injections rather than warfarin tablets may be used. This is because warfarin can potentially cause harm (birth defects) to the unborn child.
The length of time you will be advised to take anticoagulation depends on various factors. If you have a DVT during pregnancy or after an operation, then after the birth, or when you are fit again, the increased risk is much reduced. So, anticoagulation may be only for a few months. On the other hand, some people continue to have an increased risk of having a DVT. In this case the anticoagulation may be long-term.
As a guide, for a DVT that happens below the knee, you will need at least six weeks' warfarin. Usually 3-6 months of warfarin treatment is given in this situation. The length of time of anticoagulation varies from person to person. Your doctor or anticoagulant clinic will advise you how long your treatment will be for.
Note: you should not travel on any long journeys or travel by plane until at least two weeks after starting anticoagulant treatment. Travel within two weeks of a DVT is not recommended without seeking advice from a specialist - not least, because you will need regular blood tests soon after starting warfarin. Compression stockings Most people who develop a DVT are advised to wear compression stockings. This treatment has been shown to reduce the risk of a recurrent DVT, and can also reduce the risk of developing post-thrombotic syndrome. You should wear the stockings each day, for at least two years. If you do develop post-thrombotic syndrome, you may be advised to wear the stockings for more than two years.
The best type of stockings (or elastic compression hosiery as they are known), are grade 3 strength. This means that they are able to squeeze the legs, with a certain degree of force. This means that they will feel pretty tight. This is normal. It will not be as comfortable as the socks, tights or stockings you are used to wearing, and they can take a bit of getting used to. Some people really find that they cannot tolerate grade 3 stockings, and so grade 2 stockings (which create less of a squeezing force) can be used instead. It is not as good as wearing the grade 3 stockings, but better than nothing. Note: a compression stocking used following a DVT should be fitted professionally after an assessment and accurate measurement. Do not just buy over-the-counter support stockings or flight socks that may be the wrong class or size and which may potentially cause more damage. Your stockings will also need changing every 3-6 months.
If you are advised to wear a compression stocking, you should put it on each day whilst lying in bed before getting up. Wear it all day until you go to bed, or until you rest in the evening with the leg raised. Take the stocking off before going to bed. The slight pressure from the stocking helps to prevent fluid seeping into the calf tissues from the outer veins which carry the extra diverted blood following a DVT. The stocking also reduces, and may prevent, calf swelling. This in turn reduces discomfort and the risk of skin ulcers forming. Walking regularly but raising your leg whilst resting
雒ャ Unless your doctor advises against this, you should walk regularly after you are
discharged from hospital. Walking is thought to improve circulation in the affected leg and may help to reduce your risk of further DVT.
雒ャ When you are resting, as much as possible - raise your leg. This reduces the
pressure in the calf veins, and helps to prevent blood and fluid from pooling in the calves. Raised means that your foot is higher than your hip so gravity helps with blood flow returning from the calf. The easiest way to raise your leg is to recline on a sofa with your leg up on a cushion. Sitting on the sofa or in a chair, with your feet on a footstool or pouffe is not keeping your feet up - the feet are well below your hips in this position.
雒ャ Raise the foot of the bed a few inches if it is comfortable to sleep like this. This is so
your foot and calf are slightly higher than your hip when you are asleep. Other treatments Sometimes other treatments may be considered. For example:
雒ャ Thrombolytic therapy (often called clot busting) with drugs such as streptokinase or
urokinase. These drugs may help to dissolve a blood clot. This is not routine treatment as it is not clear how effective it is. However, it is sometimes used in people with a severe DVT or with a large pulmonary embolus.
雒ャ Sometimes an operation (called an embolectomy) is done to remove a blood clot
from the leg vein or pulmonary artery. These operations are not routine and it is not clear if they are an effective treatment in most cases.
雒ャ Occasionally, an operation is done to place a filter in the large vein above the
blocked leg vein. The aim is to stop any blood clots from travelling up to the lungs. This may be considered if anticoagulation cannot be given (for various reasons), or if anticoagulation fails to prevent clots breaking off and travelling up into the larger veins and up to the lungs. Preventing a first deep vein thrombosis - or a recurrence of a deep vein thrombosis
A DVT is often just a one-off event after a major operation.
However, some people who develop a DVT have an ongoing risk of a further DVT. For example, if you have a blood clotting problem, or continued immobility. As mentioned above, you may be advised to take anticoagulation (usually with warfarin) long-term. Your doctor will advise you about this.
Other things that may help to prevent a first or recurrent DVT include the following:
雒ャ If possible, avoid long periods of immobility, such as sitting in a chair for many hours.
If you are able to, get up and walk around now and then. A daily brisk walk for 30-60 minutes is even better if you can do this. The aim is to stop the blood pooling, and to get the circulation in the legs moving. Regular exercise of the calf muscles also helps. You can do some calf exercises even when you are sitting.
雒ャ Major operations are a risk for a DVT - particularly operations to the hip, lower
abdomen, and leg. You may be given an anticoagulant such as a heparin injection just before an operation to help prevent a DVT. This is called prophylaxis. Clexaneツョ (enoxaparin) and Fragminツョ (dalteparin) are the most common types of heparin given for thromboprophylaxis. Some newer drugs are now available to prevent thromboembolic complications (such as DVT and PE) after hip or knee replacement surgery. Rivaroxaban (Xareltoツョ) and dabigatran etexilate (Pradaxaツョ) are used in these situations, and can be given by mouth as a tablet, rather than injection. An inflatable sleeve connected to a pump to compress the legs during a long operation may also be used. You may also be given compression stockings (often known as TEDs - thromboembolic deterrent stockings) to wear whilst you are in hospital. It is also common practice to get you up and walking as soon as possible after an operation. A new drug called fondaparinux sodium (Arixtraツョ) can be given by injection in some circumstances to prevent DVT in surgical patients or immobile medical patients in hospital.
雒ャ When you travel on long plane, train, car or coach journeys you should have little
walks up and down the aisle every now and then. Try to exercise your calf muscles whilst sitting in your seat. (You can do this by circling your ankles, getting into a tiptoes position and lifting your toes off the floor whilst keeping your heels on the ground.) You should aim to stay well hydrated and avoid alcohol and sleeping medications. (See separate leaflet called 'Deep Vein Thrombosis - Prevention When Travelling' for more information.) If you have had a previous DVT, you should see your doctor for advice before you travel on a long journey or fly.
雒ャ People who are overweight have an increased risk of DVT. Therefore, to reduce your
risk, you should try to lose weight. Statin drugs and their role in deep vein thrombosis prevention A study published in 2009 reported that statin drugs may reduce the chance of apparently healthy people getting a DVT. Statin drugs are usually used to lower the blood cholesterol level and to help prevent cardiovascular disease (heart disease, stroke, and related diseases) in people at increased risk. But, in this study, the researchers just looked at the effect that a statin (the drug rosuvastatin was used) has in preventing clots in the veins. In the study, amongst the people who had taken a statin, there was a significantly lower number of blood clots.
However, it should be noted that, even though the participants in the study were apparently healthy, they were all at a higher risk of developing cardiovascular disease than the general population. So, more research is needed before we can be sure that the results of this study apply to everyone and before statins may be widely used to prevent DVT. In summary
雒ャ The main cause of DVT is immobility - especially during or after surgery. 雒ャ If you are having major surgery, you will usually be given medication such as heparin
injections, to prevent blood clots forming (this is called thromboprophylaxis).
雒ャ The most serious complication of DVT is a pulmonary embolus (PE), where part of
the blood clot breaks off and travels to the lung. PEs can cause death.
雒ャ Persistent calf symptoms may occur after a DVT. 雒ャ With treatment, the risk of the above two complications is much reduced. 雒ャ Treatment includes anticoagulation (usually with warfarin), compression stockings,
雒ャ Prevention is important if you have an increased risk of DVT. For example, during
long operations or when you travel on long journeys. References
雒ャ Venous thromboembolism - reducing the risk, NICE Clinical Guideline (January
2010); Reducing the risk of venous thromboembolism (deep vein thrombosis and pulmonary embolism) in patients admitted to hospital
雒ャ Deep vein thrombosis, Prodigy (April 2009) 雒ャ British National Formulary雒ャ Glynn RJ, Danielson E, Fonseca FA, et al; A randomized trial of rosuvastatin in the
prevention of venous thromboembolism. N Engl J Med. 2009 Apr 30;360(18):1851-61. Epub 2009 Mar 29. [abstract]
Comprehensive patient resources are available at www.patient.co.uk
Disclaimer: This article is for information only and should not be used for the diagnosis or treatment of medical conditions. EMIS has used all reasonable care in compiling the information but make no warranty as to its accuracy. Consult a doctor
or other health care professional for diagnosis and treatment of medical conditions. For details see our conditions. EMIS 2011 Reviewed: 30 Sep 2010 DocID: 4444 Version: 41
For the planned review period see the Data Creation and Quality Control Process.
Medizinische Informationen zu HIV und AIDSFunktionsstテカrungenbei Mテ、nnern mit HIV & AIDSDas Gesicht der HIV-Infektion hat sich durch die neuen Therapiemテカglich-keiten stark verテ、ndert: Standen frテシher schwer zu behandelnde Krankhei-ten wie zum Beispiel das Kaposi-Sarkom im Vordergrund, sind es heutemehr die mittel- und langfristigen Nebenwirkungen der antiretroviralenMedikamente. Dazu gehテ
 Deep Vein Thrombosis
Deep Vein Thrombosis