Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Microsoft word - moxatag word package insert_rev 01 08_11 clean recreation
HIGHLIGHTS OF PRESCRIBING INFORMATION
anaphylactic reactions require immediate emergency treatment with
These highlights do not include all the information needed to use
epinephrine. Oxygen, intravenous steroids, and airway management,
MOXATAG safely and effectively. See full prescribing information for
including intubation, should also be administered as indicated. (5.1)
MOXATAG.
Clostridium difficile associated diarrhea (ranging from mild diarrhea to
fatal colitis): Evaluate if diarrhea occurs. (5.2)
MOXATAG® (amoxicillin extended-release) Tablets Initial U.S. Approval: 1974 ------------------------------ADVERSE REACTIONS-------------------------------
The most common drug-related adverse reactions (incidence >1.0 %) are
To reduce the development of drug-resistant bacteria and maintain the
vulvovaginal mycotic infection, diarrhea, nausea, vomiting and headache.
effectiveness of MOXATAG and other antibacterial drugs, MOXATAG
should be used only to treat or prevent infections that are proven or strongly
To report SUSPECTED ADVERSE REACTIONS, contact Shionogi Inc.
----------------------------INDICATIONS AND USAGE--------------------------- at 1.800.849.9707 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
MOXATAG is a penicillin-class antibacterial indicated for the treatment of
tonsillitis and/or pharyngitis secondary to Streptococcus pyogenes in adults
------------------------------DRUG INTERACTIONS-------------------------------
and pediatric patients 12 years and older. (1)
Probenecid decreases the renal tubular secretion of amoxicillin.
Concurrent use of amoxicillin and probenecid may result in increased
and prolonged blood levels of amoxicillin. (7.1)
DOSAGE AND ADMINISTRATION-----------------------
Tonsillitis and/or Pharyngitis: 775 mg once daily for 10 days with a meal.
-----------------------USE IN SPECIFIC POPULATIONS------------------------
Pediatrics: The safety and effectiveness of MOXATAG in pediatric
---------------------DOSAGE FORMS AND STRENGTHS----------------------
patients younger than 12 years has not been established. (8.4)
Renal Impairment: MOXATAG has not been studied in patients with
renal impairment; however a reduction of amoxicillin dose is generally
-------------------------------CONTRAINDICATIONS------------------------------
recommended for patients with severe renal impairment. Therefore,
Patients with known serious hypersensitivity to amoxicillin or to other drugs
MOXATAG is not recommended for use in patients with severe renal
in the same class or patients who have demonstrated anaphylactic reactions to
impairment (CrCl < 30 mL/min) or patients on hemodialysis. (8.6)
See 17 for PATIENT COUNSELING INFORMATION
-----------------------WARNINGS AND PRECAUTIONS------------------------ Revised:
Serious and occasionally fatal hypersensitivity (anaphylactic) reactions
have been reported in patients on penicillin therapy. Serious
_______________________________________________________________________________________________________________________________________ FULL PRESCRIBING INFORMATION: CONTENTS* OVERDOSAGE INDICATIONS AND USAGE DESCRIPTION DOSAGE AND ADMINISTRATION CLINICAL PHARMACOLOGY DOSAGE FORMS AND STRENGTHS CONTRAINDICATIONS WARNINGS AND PRECAUTIONS
Anaphylaxis and Hypersensitivity Reactions
NONCLINICAL TOXICOLOGY
Clostridium difficile Associated Diarrhea (CDAD)
Carcinogenesis, Mutagenesis, Impairment of Fertility
CLINICAL STUDIES REFERENCES HOW SUPPLIED/STORAGE AND HANDLING PATIENT COUNSELING INFORMATION ADVERSE REACTIONS
Instructions for Administration of MOXATAG
Adverse Reactions for Other Amoxicillin Products
Clostridium difficile Associated Diarrhea
DRUG INTERACTIONS USE IN SPECIFIC POPULATIONS
*Sections or subsections omitted from the full prescribing information are not
FULL PRESCRIBING INFORMATION 5.5 Development of Drug-Resistant Bacteria
Prescribing amoxicillinin the absence of proven or strongly suspected
INDICATIONS AND USAGE
bacterial infection or treating prophylactically is unlikely to provide benefit to
Tonsillitis and/or Pharyngitis
the patient and increases the risk of the development of drug-resistant bacteria.
MOXATAG is a penicillin-class antibacterial indicated for the treatment
5.6 False-Positive Urinary Glucose Tests
of tonsillitis and/or pharyngitis secondary to Streptococcus pyogenes
High urine concentrations of ampicillin may result in false-positive
(S. pyogenes) inadults and pediatric patients 12 years and older.
reactions when testing for the presence of glucose in urine using Clinitest®,
Benedict's Solution or Fehling's Solution. Since this effect may also occur
To reduce the development of drug-resistant bacteria and maintain the
with amoxicillin, it is recommended that glucose tests based on enzymatic
effectiveness of MOXATAG and other antibacterial drugs, MOXATAG
glucose oxidase reactions (such as Clinistix®) be used.
should be used only to treat or prevent infections that are proven or strongly
suspected to be caused by susceptible bacteria. When culture and
ADVERSE REACTIONS
susceptibility information are available, they should be considered in selecting
or modifying antibacterial therapy. In the absence of such data, local
Because clinical trials are conducted under widely varying conditions,
epidemiology and susceptibility patterns may contribute to the empiric
adverse reaction rates observed in the clinical trials of a drug cannot be
directly compared to rates in the clinical trials of another drug and may not
DOSAGE AND ADMINISTRATION Tonsillitis and/or Pharyngitis 6.1 Clinical Study Experience
The recommended dose of MOXATAG is 775 mg once daily taken
within 1 hour of finishing a meal for 10 days. The full 10-day course of
In a controlled Phase 3 trial, 302 adult and pediatric patients (≥ 12 years)
therapy should be completed for effective treatment of tonsillitis and/or
were treated with MOXATAG 775 mg once-daily for 10 days and 306 adult
pharyngitis secondary to S. pyogenes.
and pediatric patients (≥ 12 years) were treated with penicillin VK 250 mg
In this clinical trial, the majority of treatment-emergent adverse
DOSAGE FORMS AND STRENGTHS
reactions were of a mild and transient nature with similar frequency reported
775 mg blue film-coated, oval-shaped tablets printed with “MB-111” on
in both treatment groups. Discontinuation due to drug-related treatment-
emergent adverse reactions occurred in 1.3 % of the MOXATAG-treated
patients and 3.3 % of the penicillin VK-treated patients.
CONTRAINDICATIONS
The most frequently reported adverse reactions (≥ 1%) which were
MOXATAG is contraindicated in patients with known serious
suspected or probably drug-related are shown in Table 1.
hypersensitivity to amoxicillin or to other drugs in the same class or patients
who have demonstrated anaphylactic reactions to beta-lactams.
Table 1. Drug-Related Treatment-Emergent Adverse Reactions by System
Organ Class Experienced by ≥1% of Patients in Either Treatment Group –
WARNINGS AND PRECAUTIONS 5.1 Anaphylaxis and Hypersensitivity Reactions
Serious and occasionally fatal hypersensitivity (anaphylactic) reactions
have been reported in patients on penicillin therapy. Although anaphylaxis is
more frequent following parenteral therapy, it has occurred in patients on oral
penicillins. These reactions are more likely to occur in individuals with a
history of penicillin hypersensitivity and/or a history of sensitivity to multiple
allergens. There have been reports of individuals with a history of penicillin
hypersensitivity who have experienced severe reactions when treated with
cephalosporins. Before initiating therapy with MOXATAG, careful inquiry
should be made concerning previous hypersensitivity reactions to penicillins,
cephalosporins, or other allergens. If an allergic reaction occurs, MOXATAG
should be discontinued and appropriate therapy instituted.
Serious anaphylactic reactions require immediate emergency treatment with epinephrine. Oxygen, intravenous steroids, and airway management, including intubation, should also be administered as
*Presented in decreasing order of frequency in the MOXATAG column within
indicated. 5.2 Clostridium difficile Associated Diarrhea (CDAD) Clostridium difficile Associated Diarrhea (CDAD) has been reported
with nearly all antibacterial agents, including amoxicillin, and may range in
6.2 Adverse Reactions for Other Amoxicillin Products The following adverse reactions have been reported for other products
severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents
alters the normal flora of the colon leading to overgrowth of C. difficile.
Infections and Infestations: Mucocutaneous candidiasis.
C. difficile produces toxins A and B which contribute to the development of CDAD. Hypertoxin-producing strains of
Gastrointestinal: Nausea, vomiting, diarrhea, and hemorrhagic/
C. difficile cause increased morbidity
and mortality, as these infections can be refractory to antimicrobial therapy
Onset of pseudomembranous colitis symptoms may occur during or after
and may require colectomy. CDAD must be considered in all patients who
present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the
Hypersensitivity Reactions: Anaphylaxis (See Warnings and
Serum sickness like reactions, erythematous maculopapular rashes,
If CDAD is suspected or confirmed, ongoing antibiotic use not directed
erythema multiforme, Stevens-Johnson Syndrome, exfoliative dermatitis,
against C. difficile may need to be discontinued. Appropriate fluid and
toxic epidermal necrolysis, acute generalized exanthematous pustulosis,
electrolyte management, protein supplementation, antibiotic treatment of
hypersensitivity vasculitis and urticaria have been reported. (NOTE: These
C. difficile, and surgical evaluation should be instituted as clinically indicated.
hypersensitivity reactions may be controlled with antihistamines and, if
5.3 Superinfections
necessary, systemic corticosteroids. Whenever such reactions occur,
The possibility of superinfections with mycotic or bacterial pathogens
amoxicillin should be discontinued unless, in the opinion of the physician, the
should be kept in mind during therapy. If superinfections occur, amoxicillin
condition being treated is life-threatening and amenable only to amoxicillin
should be discontinued and appropriate therapy instituted.
5.4 Mononucleosis Rash A high percentage of patients with mononucleosis who receive Liver: A moderate rise in AST (SGOT) and/or ALT (SGPT) has been
noted, but the significance of this finding is unknown. Hepatic dysfunction
ampicillin develop an erythematous skin rash. Thus, ampicillin-class
including cholestatic jaundice, hepatic cholestasis and acute cytolytic hepatitis
antibiotics should not be administered to patients with mononucleosis.
Hemic and Lymphatic Systems: Anemia, including hemolytic anemia,
thrombocytopenia, thrombocytopenic purpura, eosinophilia, leukopenia, and
agranulocytosis have been reported during therapy with penicillins. These
reactions are usually reversible on discontinuation of therapy and are believed
10. OVERDOSAGE Central Nervous System: Reversible hyperactivity, agitation, anxiety,
In case of overdose, discontinue medication, treat symptomatically, and
insomnia, confusion, convulsions, behavioral changes, and/or dizziness have
institute supportive measures as required. If the overdose is very recent and
there is no contraindication, an attempt at emesis or other means of removal of
Renal: Crystalluria has also been reported
drug from the stomach may be performed. A prospective study of 51 pediatric
Miscellaneous: Tooth discoloration (brown, yellow, or gray staining)
patients at a poison-control center suggested that overdosages of less than 250
has been rarely reported. Most reports occurred in pediatric patients.
mg/kg of amoxicillin are not associated with significant clinical symptoms
Discoloration was reduced or eliminated with brushing or dental cleaning in
Interstitial nephritis resulting in oliguric renal failure has been reported
in a small number of patients after overdosage with amoxicillin.
DRUG INTERACTIONS
Crystalluria, in some cases leading to renal failure, has also been
7.1 Probenecid
reported after amoxicillin overdosage in adult and pediatric patients. In case
Probenecid decreases the renal tubular secretion of amoxicillin.
of overdosage, adequate fluid intake and diuresis should be maintained to
Concurrent use of MOXATAG and probenecid may result in increased and
reduce the risk of amoxicillin crystalluria.
prolonged blood levels of amoxicillin. The clinical relevance of this finding
Renal impairment appears to be reversible with cessation of drug
administration. High blood levels may occur more readily in patients with
7.2 Other Antibiotics
impaired renal function because of decreased renal clearance of amoxicillin.
Chloramphenicol, macrolides, sulfonamides, and tetracyclines may
Amoxicillin may be removed from circulation by hemodialysis.
interfere with the bactericidal effects of penicillin. This has been demonstrated
For additional information about overdose treatment, call a poison
in vitro; however, the clinical significance of this interaction is not well
7.3 Oral Contraceptives
As with other antibiotics, amoxicillin may affect the gut flora, leading to
11. DESCRIPTION
lower estrogen reabsorption and potentially resulting in reduced efficacy of
MOXATAG (amoxicillin extended-release) tablets for oral
combined oral estrogen/progesterone contraceptives.
administration are provided as blue film-coated, oval shaped tablets that
contain 775 mg of amoxicillin as the trihydrate and are printed with ”MB-
USE IN SPECIFIC POPULATIONS 8.1 Pregnancy
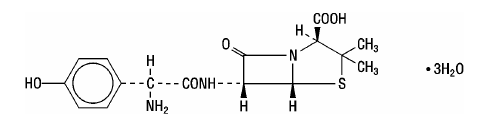
Amoxicillin is a semi-synthetic antibiotic, an analog of ampicillin, with
Teratogenic Effects. Pregnancy Category B. Reproduction studies
bactericidal activity against gram-positive and gram-negative microorganisms.
have been performed in mice and rats at doses up to 2000 mg/kg (12.5 and 25
Chemically, amoxicillin is (2 S,5 R,6 R)-6-[(R)-(-)-2-amino-2-(p-
times the human dose in mg/m2) and have revealed no evidence of impaired
hydroxyphenyl) acetamido]-3,3-dimethyl-7-oxo-4-thia-1-
fertility or harm to the fetus due to amoxicillin. There are, however, no
azabicyclo[3.2.0]heptane-2-carboxylic acid trihydrate. Its chemical name is
adequate and well-controlled studies in pregnant women. Because animal
amoxicillin. It may be represented structurally as:
reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed.
8.2 Labor and Delivery Oral ampicillin-class antibiotics are poorly absorbed during labor.
Studies in guinea pigs showed that intravenous administration of ampicillin slightly decreased the uterine tone and frequency of contractions but moderately increased the height and duration of contractions. However, it is not known whether use of amoxicillin in humans during labor or delivery has
immediate or delayed adverse effects on the fetus, prolongs the duration of
The amoxicillin molecular formula is C16H19N3O5S·3H2O, and the
labor, or increases the likelihood that forceps delivery or other obstetrical
intervention or resuscitation of the newborn will be necessary.
MOXATAG is an extended release tablet formulation consisting of three
components, one immediate-release and two delayed-release, each containing
8.3 Nursing Mothers Penicillins have been shown to be excreted in human milk. Amoxicillin
amoxicillin. The three components are combined in a specific ratio to prolong
use by nursing mothers may lead to sensitization of infants. Caution should be
the release of amoxicillin from MOXATAG compared to immediate-release
exercised when amoxicillin is administered to a nursing woman.
Each tablet contains amoxicillin, crospovidone, FD&C Blue #2 lake,
8.4 Pediatric Use The safety and effectiveness of MOXATAG in pediatric patients 12
hypromellose, hypromellose acetate succinate, iron oxide, magnesium
years of age and older have been established based on results of a clinical trial
stearate, methacrylic acid copolymer, microcrystalline cellulose, polyethylene
that included adults and pediatric patients (12 years and older). [see
glycol 400, polyoxyl 35 castor oil, povidone, shellac, colloidal silicon dioxide,
sodium lauryl sulfate, talc, titanium dioxide, and triethyl citrate.
Studies (14)] Sixty three (21 %) of the study participants were pediatric patients 12 years of age and older. There were no significant differences in
treatment response or adverse reactions from adults.
12. CLINICAL PHARMACOLOGY
The safety and effectiveness of MOXATAG in pediatric patients
12.1 Mechanism of Action
younger than 12 years has not been established.
Amoxicillin is an antibacterial drug. [see Clinical Pharmacology (12.4)]
8.5 Geriatric Use Clinical studies with MOXATAG did not include a sufficient number of 12.2 Pharmacokinetics
patients aged 65 years and over to determine whether they respond differently
MOXATAG is an extended-release formulation of amoxicillin intended to
from younger patients. Other reported clinical experiences with amoxicillin
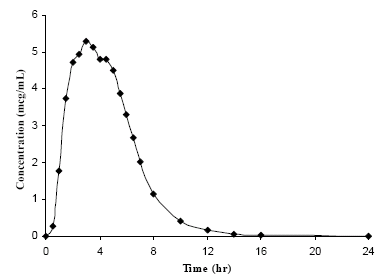
provide once-daily dosing. Following the administration of MOXATAG with
have not yet identified differences in responses between the elderly and
a low-fat meal in healthy subjects, mean amoxicillin AUC0-∞, Cmax, and Tmax
younger patients, but a greater sensitivity of some older individuals cannot be
values were 29.8 μg•h/mL, 6.6 μg/mL and 3.1 hours, respectively. The mean
plasma concentration-time curve is shown below in Figure 1.
This drug is known to be substantially excreted by the kidneys, and the
risk of adverse reactions to this drug may be greater in patients with impaired
Figure 1. Mean Amoxicillin Plasma Concentrations Following a Single
renal function. Because elderly patients are more likely to have decreased
Oral Dose of MOXATAG With a Low-Fat Meal in Healthy Subjects (N=20)
renal function, care should be taken in dose selection, and it may be useful to
8.6 Renal Impairment MOXATAG has not been studied in patients with renal impairment;
however, a reduction of amoxicillin dose is generally recommended for patients with severe renal impairment. Therefore, MOXATAG is not recommended for use in patients with severe renal impairment (CrCl <30 mL/min) or patients on hemodialysis.
Susceptibility Test Methods:
When available, the clinical microbiology laboratory should provide
cumulative results of the in vitro susceptibility test results for antimicrobial drugs used in local hospitals and practice areas to the physician as periodic reports that describe the susceptibility profile of nosocomial and community-acquired pathogens. These reports should aid the physician in selecting the most effective antimicrobial.
Susceptibility testing of penicillins (such as amoxicillin) and other β-
lactams approved by FDA for the treatment of Group A streptococcus (S. pyogenes) is not routinely necessary for clinical purposes. Isolates of Group A streptococcus resistant to amoxicillin have not been recognized and therefore all isolates can be considered susceptible to amoxicillin However, susceptibility tests can be conducted using dilution or diffusion techniques employing penicillin or ampicillin to predict susceptibility to amoxicillin.
Dilution Techniques with food decreases the rate, but not the extent
of amoxicillin absorption. Compared to immediate-release amoxicillin
Quantitative methods are used to determine antimicrobial MICs. These
suspension, the rate of amoxicillin absorption following administration of
MICs provide estimates of the susceptibility of bacteria to antimicrobial
MOXATAG was slower, resulting in a lower C
compounds. The MICs should be determined using a standardized
amoxicillin exposure (AUC) achieved with MOXATAG is similar to that
procedure1,2. Standardized procedures are based on a dilution method (broth
observed after oral administration of a comparable dose of immediate-release
or agar) or equivalent with standardized inoculum concentrations and
standardized concentrations of penicillin or ampicillin. The susceptibility of
Amoxicillin diffuses readily into most body tissues and fluids, with
Group A streptococcus to penicillin or amoxicillin should be interpreted
the exception of brain and spinal fluid, except when meninges are inflamed.
Amoxicillin is approximately 20% protein bound in human serum.
Amoxicillin is primarily cleared by renal excretion. Approximately 60%
Diffusion Technique
of an oral dose of immediate-release amoxicillin is eliminated unchanged in
urine. The half-life of amoxicillin after oral administration of MOXATAG is
Quantitative methods that require measurement of zone diameters also
approximately 1.5 hours, similar to that of immediate-release amoxicillin. No
provide reproducible estimates of the susceptibility of bacteria to
accumulation of amoxicillin was observed after once-daily dosing of 775 mg
antimicrobial compounds. One such standardized procedure3 requires the use
of a standardized inoculum concentration. This procedure uses paper disks
impregnated with 10 units penicillin or 10 mcg ampicillin to test the susceptibility of S. pyogenes to penicillin or amoxicillin. Reports from the
Drug Interactions
laboratory providing results of the standard single-disk susceptibility test
In a study of healthy adult subjects, amoxicillin AUC was similar
should be interpreted according to the criteria in Table 2.
max increased approximately 35% following the administration of
lansoprazole with MOXATAG given with food.
Probenecid decreases the renal tubular secretion of amoxicillin.
Table 2. Susceptibility Test Results Interpretive Criteria for Beta-Hemolytic
Concurrent use of MOXATAG and probenecid may result in increased and
Streptococci including Streptococcus pyogenes
prolonged blood levels of amoxicillin. The clinical relevance of this finding
12.4 Microbiology Amoxicillin is a semi-synthetic antimicrobial belonging to the penicillin
class of antimicrobials with activity against gram-positive bacteria.
The current absence of data on resistant isolates precludes defining any categories other than “Susceptible”. Isolates yielding results suggestive of a
Mechanism of Action
“nonsusceptible” category should be retested, and if the result is confirmed,
Amoxicillin exerts its bactericidal action against susceptible organisms
the isolate should be submitted to a reference laboratory for further testing.
during the stage of multiplication. It acts through the inhibition of
Quality Control
Standardized susceptibility test procedures require the use of laboratory controls to monitor and ensure the accuracy and precision of the supplies and
Mechanism of Resistance
reagents used in the assay, and the techniques of the individuals performing
To date there are no known mechanisms of resistance to penicillin or
the test. Standard penicillin or ampicillin powders should provide the MIC
ranges provided in Table 3. For the disk diffusion technique using the 10 unit
penicillin disk or 10 µg ampicillin disk the criteria in Table 3 should be
S. pyogenes and in clinical infections as described in the
Table 3. Acceptable Quality Control Ranges for Susceptibility Testing
Facultative Gram-Positive Bacteria: in vitro data are available, but their clinical significance is
unknown. At least 90% of the following microorganisms exhibit an
minimum inhibitory concentration (MIC) less than or equal to the
susceptibility breakpoint of amoxicillin (as determined by susceptibility tests
using the class representative agents penicillin or ampicillin). Facultative Gram-Positive Bacteria: Streptococcus spp. (Group B, C, and G; β-hemolytic)
13. NONCLINICAL TOXICOLOGY
effective treatment of tonsillitis and/or pharyngitis secondary to S. pyogenes.13.1 Carcinogenesis, Mutagenesis, Impairment of Fertility
Patients should be instructed not to chew or crush the tablet. No other forms
Long-term studies in animals have not been performed to evaluate
of immediate-release amoxicillin can be substituted for MOXATAG.
carcinogenic potential. Studies to detect mutagenic potential of amoxicillin
17.2 Hypersensitivity Reactions
alone have not been conducted; however, the following information is
Patients should be informed that serious and occasionally fatal
available from tests on a 4:1 mixture of amoxicillin and potassium clavulanate
hypersensitivity (anaphylactic) reactions have been reported while on
(Augmentin). Augmentin was non-mutagenic in the Ames bacterial mutation
penicillin therapy. Patients should be questioned regarding any
assay, and the yeast gene conversion assay. Augmentin was weakly positive in
hypersensitivity reactions to penicillins, cephalosporins or other allergens.
the mouse lymphoma assay, but the trend toward increased mutation
Whenever such reactions occur, the patient should be instructed to contact
frequencies in this assay occurred at doses that were also associated with
their physician immediately. Serious anaphylactic reactions require
decreased cell survival. Augmentin was negative in the mouse micronucleus
immediate emergency treatment with epinephrine. Oxygen, intravenous
test, and in the dominant lethal assay in mice. Potassium clavulanate alone
steroids, and airway management, including intubation, should also be
was tested in the Ames bacterial mutation assay and in the mouse
micronucleus test, and was negative in each of these assays. In a multi-
17.3 Clostridium difficile Associated Diarrhea
generation reproduction study in rats, no impairment of fertility or other
Patients should be informed that diarrhea is a common problem caused by
adverse reproductive effects were seen at doses up to 500 mg/kg
antibiotics which usually ends when the antibiotic is discontinued. Sometimes
(approximately 6 times the human dose in mg/m2).
after starting treatment with antibiotics, patients can develop watery and
bloody stools (with or without stomach cramps and fever) even as late as two
14. CLINICAL STUDIES
or more months after having taken the last dose of the antibiotic. If this
In a randomized, parallel-group, multi-center, double-blind, double-
occurs, patients should contact their physician as soon as possible.
dummy study in adults and pediatrics (age ≥ 12 years) with tonsillitis and/or
pharyngitis secondary to S. pyogenes, MOXATAG 775 mg QD for 10 days
AUGMENTIN is a registered trademark of GlaxoSmithKline.
was non-inferior to penicillin VK 250 mg QID for 10 days.
CLINITEST is a registered trademark of Miles, Inc.
CLINISTIX is a registered trademark of Bayer Corporation.
Using strict evaluability and microbiologic response criteria 4-8 days
MOXATAG is a registered trademark of Shionogi Inc., all rights reserved.
post-therapy, the following bacteriological eradication rates and statistical
outcomes in the per-protocol (PPb) and modified intent-to-treat (mITT)
Manufactured for: Shionogi Inc., Alpharetta, Ga. 30005
populations were obtained (Table 4). The mITT population included all
randomized patients with a positive throat culture for S. pyogenes at baseline.
Manufactured by: Stada Production Ireland, Clonmel, Ireland
The PPb population included mITT patients who had post-therapy cultures,
were compliant with treatment, and didn’t have major protocol violations.
U.S. Patents 6,544,555; 6,669,948; 6,723,341
Table 4. Bacteriological Eradication Rates in Patients with Tonsillitis and/or Pharyngitis
Copyright 2011 Shionogi Inc. All rights reserved.
Rate Difference Population MOXATAG Penicillin VK 95% CI (%)
15. REFERENCES 1.) Clinical and Laboratory Standards Institute (CLSI). Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically; Approved Standard - 7th ed Clinical and Laboratory Standards Institute document M7-A7. Clinical and Laboratory Standards Institute, 940 West Valley Road, Suite 1400, Wayne, PA 19087-1898 USA, 2006. 2.) CLSI. Performance Standards for Antimicrobial Susceptibility Testing; 17th Informational Supplement. CLSI document M100-S17 CLSI, Wayne, PA 19087-1898, 2007. 3.) CLSI. Performance Standards for Antimicrobial Disk Susceptibility Tests; Approved Standard - 9th ed. CLSI document M2-A9 CLSI, Wayne, PA 19087- 1898 2006. 16. HOW SUPPLIED/STORAGE AND HANDLING
MOXATAG tablets for oral administration are provided as blue film-
coated, oval-shaped tablets that contain 775 mg of amoxicillin as the trihydrate. The tablets are printed with “MB-111” on one side in black edible ink. MOXATAG is packaged in bottles as follows:
Bottles of 30 Storage Store at 25º C (77º F); excursions permitted to 15–30º C (59–86º F) [See
USP Controlled Room Temperature.] 17. PATIENT COUNSELING INFORMATION 17.1 Instructions for Administration of MOXATAG Patients should be informed that the recommended dose of MOXATAG
is 775 mg once daily taken with food for 10 days. MOXATAG should be taken within 1 hour of finishing a meal and at approximately the same time every day. The full 10-day course of therapy should be completed for
COMMONLY USED PSYCHOTROPIC DRUGS po = by mouth; prn = as needed; qd = 1x / day ; bid = 2x/day ; tid = 3x/day ; qid = 4x/day; qod = every other day; qhs = at bedtime; qac = before meals; = on WalMart’s $4 Rx plan, however not al dosages may be covered IMPORTANT CLINICAL INFORMATION Commonly used Antidepressants and Antianxiety Medications Start: 100mg bid titrating
Elena Bertola Impregnation of a natural surgically implantable porous structure for the controlled release of antibiotics Introduction The spongy bone tissue is commonly used in medicine for dental implantations as support for the osseous regeneration. One of the possible problems of such implantations after the surgery is the growth of infections in the treated zone. In this paper we
 agranulocytosis have been reported during therapy with penicillins. These
reactions are usually reversible on discontinuation of therapy and are believed
10. OVERDOSAGE
agranulocytosis have been reported during therapy with penicillins. These
reactions are usually reversible on discontinuation of therapy and are believed
10. OVERDOSAGE