Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Unknown
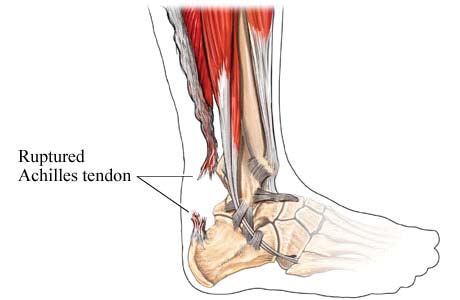
sussexfoot&anklecentre Achilles Tendon Rupture
While it is possible to treat ruptures of the Achilles tendon non-operatively
(plaster), this is often associated with a substantially higher re-rupture rate
(average 18%) than operative treatment (risk of re-rupture after surgical repair
of the tendon <3%) and can also result in a weaker calf muscle/tendon unit.
Surgery is performed in order to regain maximum strength of the Achilles and
push-off strength of the foot. The strength of the muscle depends on
establishing the exact correct tension between the muscle and the tendon, and
this is restored most accurately by surgically repairing the torn tendon ends.
This surgery involves a general anaesthetic. An incision is made over the
ruptured tendon at the back of the calf at or just above the level of the
ankle. The surgical technique needs to be meticulous and great care taken
with the skin in order to minimise the risk of wound healing problems.
Modern surgical techniques mean that the risk of serious wound problems
Type of Procedure:
after this type of surgery is very small (~1%). Length of Procedure: Main Risks Of Surgery Swelling/Scar - Initially the foot and ankle will be swollen and needs Anaesthesia:
elevating. The swelling will disperse over the following weeks and monthsbut will remain evident for up to 6-9 months. The scar can cause irritationto begin with but usually settles to a great extent over the first 4-6 weeks. Rupture or tearing of the Achilles tendonWound healing problems – The risk of serious wound healing is a common condition and typically
problems is approxiamately 1%. It is important to keep the foot elevatedover the first 10 days to reduce the swelling and risk of wound healing
occurs in an individual who undertakes
problems. In rare circumstances when the wound is problematic, further
sporting activity to which they areInfection – The risk of deep infection occurring is approximately 1%.
For example, the invitation to play tennis after a prolonged period of little or
You will be given intravenous antibiotics to help prevent this. It is important to
no exercise. However, tears can also occur in those who play sport regularly
keep the foot elevated over the first 10 days to reduce the swelling and risk
but it is usually the more explosive take-off/high impact landing action sports
of infection. If there is an infection, it may resolve with a course of antibiotics
that are responsible (although tears can occasionally occur after simply
but may require a period of hospitalisation or rarely, further surgery.
stumbling when walking). Essentially, there is a vigorous contraction of the
calf muscle and the Achilles tendon tears. The patient often describes the
Nerve damage – The sural nerve is close to the incision. This supplies
sense that someone or something has hit the back of their leg producing
sensation to the outside of the foot. This may rarely (1%) be damagedduring the surgery and this may leave a patch of numbness on the outside
sudden pain. Although it is possible to walk, it is painful and the leg is weak.
of the foot. This numbness may be permanent but would not affect function. Re-rupture of the Achilles Tendon – Following surgical repair of the tendon the risk of further rupture is less than 3% (compared to an average of 18% in reports of non surgical treatment of this injury). It is very important that patients follow the post operative instructions provided to minimise the risk of such problems. www.sussexfoot.com Post Operative Course Achilles Tendon Repair Deep Vein Thrombosis (DVT) – This is a clot of blood in the
deep veins of the leg. The risk of a clot occurring is reported as less than
• Below knee cast (backslab plaster) applied at end of surgery
1% after foot and ankle surgery which is generally substantially lower thanafter hip or knee surgery. Suspicion of DVT is raised if the leg becomes
• Expect some numbness in foot for 12-24 hours
very swollen and painful. There are tests that can be performed to
• Pain medication and elevation of foot
confirm/exclude the presence of a DVT. If confirmed, you will probablyrequire treatment with a blood thinning agent (heparin preparation and / or
warfarin). The main concern with regards a DVT is that rarely (<1:1000
chance with foot and ankle surgery) a piece of clot can break away in theleg and travel to the lungs which is much more serious and can be life-threatening. This is called a pulmonary embolus and signs of this include
• Elevation of leg as much as possible for first 2 weeks
Whilst in hospital following surgery it is likely that you will be treated with ablood thinning agent (LMWH - low molecular weight heparin injections) to
• Mobilisation non-weight bearing with physiotherapist (crutches/frame)
minimise the risk of DVT / PE but this does not afford total protection. You
• Discharge home day 2 or 3 usually possible
will be given a venous compression stocking to wear on the uninjured legand exercises to keep the toes and knee moving are advised, as well as
• No weight bearing on operated leg for first 4 weeks
• May shower/bath if able to keep leg dry
If you are concerned that the leg has become more swollen and painful(some swelling always occurs after surgery), or if you experience chestpain/shortness of breath, then you should contact the hospital, general
practitioner, or accident and emergency department immediately.
• Outpatient review of wounds (and removal stitches if necessary)
Sick Leave
• Cast replaced with boot including heel wedges
In general 4 weeks off work is required for sedentary employment, 12
• No weight bearing on operated leg/boot untile 4 weeks post surgery
weeks for standing or walking work and 16 weeks for manual / labour
• Patient to remain in boot at all times (except for supervised physio)
intensive work. We will provide a sick certificate for the first 2 weeks;further certificates can be obtained from your GP.
• Supervised physiotherapy may begin. Only include:
• Swelling control - ice, elevation, effleurage and massage as appropriate
ONLY IF left leg surgery only and automatic vehicle should you expect to
• No stretches/active exercises until 4 weeks post surgery
return to driving is usually possible after outpatient review at 2 weeks postsurgery - otherwise unable to drive until 3 months post surgery.
• May return to driving at this stage ONLY IF left leg surgery only and
These notes are intended as a guide and some of the details may
automatic vehicle - otherwise unable to drive until 3 months post surgery
vary according to your individual surgery or because of specialinstructions from your surgeon. 1 Outpatient review and removal of (2) heel wedges as appropriate 3 Allowed to partially weight bear on operated leg with crutches/frame 4 Supervised physiotherapy to continue (+ unsupervised exercise may
begin) as instructed by physiotherapist including:
a Swelling control - ice, elevation, effleurage and massage b Scar mobilisation c Assisted/active PF, DF Inversion/eversion exercises to begin gently www.sussexfoot.com
• Outpatient review and further wedges removed
• Usually allowed to begin full weight bearing in boot at this stage
• Boot removed for bathing / showering at this stage
• To remain in boot until 8 weeks following surgery
a Swelling control – ice, elevation, effleurage and massage b Scar mobilisation c Assisted / active PF, DF Inversion / eversion exercises d Gait progression work i Aim for walking without walking aids (if plantegrade achieved) II Aim to achieve walking with parallel bars out of boot prior 8 weeks (2 months) 1 Physiotherapy to continue: a Scar mobilisation b Assisted / active PF, DF Inversion / eversion exercises c Boot removed (by physio once functional dorsiflexion achieved) d Begin double stance heel raises and continue strengthening e Single gel heel insert in shoe - worn until 12 weeks after surgery f May begin proprioceptive work after week 8 12 weeks (3 months) onwards 1. Outpatient review 2. Physiotherapy to continue: a Begin single stance heel rise exercises b Begin jogging on trampoline and treadmill via walk-run programme c Eventually progress 20 minute outdoor run before adding cutting d Progress later to figure of eight drills as appropriate sussexfoot&anklecentre
The Sussex Foot & Ankle Centre was founded in 2005 by two orthopaedic surgeons, David Redfern
David J Redfern Haywards Heath
and Stephen Bendall, with the aim of providing a high quality specialist service for the diagnosis
and treatment of all foot and ankle problems. Both orthopaedic surgeons are specialists in problems
affecting the foot and ankle and have many years of experience. They operate the service with
outpatient clinics at the Brighton and Haywards Heath Nuffield Hospitals. Stephen P Bendall Tel 01444 456999
The sussex foot and ankle center strives to provide the best advice and treatment for all foot and
ankle problems. This includes sports injuries and trauma, bunions, metatarsalgia, and arthritis. Brighton
Both surgeons have particular interests in minimally invasive surgery and are at the forefront of
developing such techniques in this country. Private Secretary 01273 627060 Direct Fax 01273 627061
Both surgeons are also academically very active and have appointments within the national
Email admin@sussexfoot.com
(BOFAS) and international (EFAS) professional foot and ankle surgery societies. Tel 01273 627060 www.sussexfoot.com
Yesterday we talked about the loop product and the associated Gerstenhaber andBV structures on the loops space of the manifold. I’m going to put the equivariantpart of the story on hold for a little bit and come back to it. Since the first papers of Chas-Sullivan, others have taken these ideas and madethem more rigorous. To my knowledge, Cohen-Jones was the first one. This usesthe language of
Toxicology Brief managing common poisonings in companion animals P E T F O O D R E C A L LAminopterinand melamineidentified in some of thetested samples of the re-called pet foods manufac-tured by Menu Foods(www.menufoods.com). How thesesubstances entered the pet food chainhasn't been determined. Investigatorsalso don't know whether these sub- M etformin is an antihyper- glycemic p
 sussexfoot&anklecentre
sussexfoot&anklecentre