Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Original article: applied kinesiology for treatment of women with mastalgia
The Breast (2001) 10, 15–19# 2001 Harcourt Publishers Ltddoi:10.1054/brst.2000.0176, available online at http://www.idealibrary.com on
Applied kinesiology for treatment of women with mastalgia
W. M. Gregory,1 S. P. Mills,2 H. H. Hamed1 and I. S. Fentiman11Hedley Atkins Breast Unit, Guy’s Hospital, London, UK; 2Association of Systematic Kinesiology, Surbiton,Surrey, UK
S U M M A R Y. To determine whether an applied kinesiology technique was of benefit to women with breast pain,an open pilot study was conducted in which 88 newly presenting women with self-rated moderate or severe mastalgiawere treated by applied kinesiology. This involved a hands-on technique consisting of rubbing a series of ‘lymphaticreflex points’ while touching painful areas of the breasts. The women were predominantly pre-menopausal, andpatients with both cyclical and non-cyclical pain were included in the study. Patients’ self-rated pain scores, bothbefore and immediately after applied kinesiology were compared, together with a further score 2 months later. Immediately after treatment there was considerable reduction in breast pain in 60% of patients with completeresolution in 18%. At the visit after 2 months, there was a reduction in severity, duration and frequency of pain of50% or more in about 60% of cases (P50.0001). This preliminary study suggests that applied kinesiology may be aneffective treatment for mastalgia, without side-effects and merits testing against standard drug therapies. # 2001Harcourt Publishers Ltd
similarities with both chiropractic and acupuncture. Asimple physical technique has been developed, which is
Mastalgia, either cyclical or non-cyclical is a common
suitable for application to women with breast pain.
problem, which is usually-limiting and often responds to
This involves the kinesiologist touching the painful area
reassurance that there is no underlying serious pathology.
of the breast with one hand while massaging a series of
Nevertheless there is a small proportion of women who
points on the outside of the upper leg (from the knee to
have pain of such severity that it interferes with their
the hip) with the other hand.These points were first
personal, sexual and worklife. For this reason some are
described by Chapman in the 1930s, and he claimed to
given endocrine treatments such as bromocriptine,
have correlated these reflex points with specific organs.
danazol and tamoxifen, all of which have been shown in
Chapman’s reflex points are found mostly on the torso
double-blind placebo-controlled studies to be effective.
and legs. Those used to relieve breast pain run along a
A wide variety of side-effects has been reported and
line in the centre of the outside of the thigh,
sometimes these can be of such severity that treatment
approximately where the seam would lie on pair of
has to be stopped. After cessation of treatment there is
trousers. These points may be very tender and the
usually relapse of pain, often within 3 months.Dietary
kinesiologist usually massages them only briefly at first,
factors may also contribute to breast pain and reduction
returning to rub more firmly until the tenderness
of fat intake has been shown to reduce mastas has
diminishes. The massaging is done with a rotary-type
the use of evening primrose oil (gamma linolenic
action of the fingertips, beginning at the knee and
This latter treatment appears to be effective mostly in
working up the leg to the hip. Once pain in this area of
the breast has reduced the kinesiologist moves on to
Applied kinesiology is a multifaceted complimentary
touch any other painful areas of the breast. This process
medical approach, which has developed recently and has
usually takes 20–30 min to complete. Subsequently thepatient can use this technique herself. To test thiskinesiological approach in women with mastalgia, a trial
Address correspondence to: I. S. Fentiman, Hedley Atkins Breast Unit,Guy’s Hospital, London SE1 GRT, UK.
was initiated at Guy’s Hospital Breast unit.
participating was 37 years (range 17–64). Of thepatients, 68 were pre-menopausal, two were perimeno-
All cases had self-rated moderate or severe mastalgia
pausal, six had undergone hysterectomies, and 10 were
with no discrete masses on clinical examination. They
were aged 20–70 years with either cyclical or non-
The patients were seen by just two kinesiologists
cyclical breast pain, and with no evidence of malignancy
(SPM or WMG). The pain evaluation forms were
on mammograms for those aged over 40 years. None
handed out by the kinesiologist and the women
were receiving any other treatment for mastalgia apart
evaluated their pain before and after the treatment.
from mild analgesics, nor had any been treated with
Ideally, to avoid bias, it would have been better to have
endocrine therapy in the previous 3 months. Three
the patients fill out the questionnaires at their leisure,
applied kinesiology treatments were given at 1 monthly
and post the completed forms directly to the statistician.
intervals and after 2 months a self-assessment form was
However, with the before and after evaluations being so
close together, this would have been inadvisable. It is a
Two assessment forms were used in the study, and
difficult task, and prone to error, to evaluate a prior pain
that has since changed some time after this change has
completed by women at their initial visit and compared
pain before and after the first treatment, rated on a0–10 scale. The second form, completed 2 months later,asked patients to rate their pain over this period andconsidered four aspects: severity, frequency, duration
The t-test was used to test the significance of thedifference between the before and after pain scores on
the first questionnaire, and to test for whether changesin pain score for the four different attributes listed in
Between May 1995 and March 1997, 88 sequential
the second questionnaire were significant. As a second
patients were entered into the study. All were seen in a
and more conservative check on these results, a
dedicated Mastalgia Clinic and had self-rated moderate
non-parametric test was also used. For this test,
or severe breast pain. After the initial consultation and
observed changes in scores were coded as 0 (no change),
examination/tests with the doctor, those women who
1 (improvement) or –1 (deterioration). The Wilcoxon
were reassured and no longer appeared worried by their
signed rank test was then used to evaluate the
pain, were not randomized. The study was explained by
probability that there was no overall change (median
the surgeon conducting the clinic and if the patient
score=0). Correlations were quantified using Spear-
agreed to participate, she was treated immediately
man’s correlation coefficient. P values 50.05 were taken
by the kinesiologist. The mean age of the patients
Applied kinesiology for treatment of women
patient experienced an increase of pain after appliedkinesiology.
To ensure that the significance of this result is not
based merely on the women showing small improve-
Of the 88 completed forms, 20 showed that the patient
ments, we re-coded one-point improvements as 0 (i.e. no
had no pain on the day of the visit and these were
change). This still gave a mean improvement of 2.1, and
therefore not evaluable when analyzing improvement in
a t-statistic of 8.21 (P50.00001). Furthermore, re-coding
pain score. One patient had an initial pain score but no
1- and 2-point improvements as 0 gave a mean improve-
post-treatment score and was also unevaluable, leaving
ment of 1.6, and a t-statistic of 5.64 (P50.00001). Thus
67 evaluable cases. As is shown in after the first
the improvements in pain score are still significant, even
treatment there was a rapid and highly significant
when discounting small improvements.
reduction in pain. The mean improvement in pain was2.3, with a standard error for this mean of 23, and at-statistic of 10.1 (P50.00001). The mean starting value
(on a scale of 10) was 4.0, with a standard deviation of3.1. The mean improvement in pain score was 51%. The
This evaluation was carried out at 2 months, after three
Wilcoxon statistic also gave a highly significant result;
applied kinesiology treatments. Patients were asked to
W = 1770, P50.00001. There was a 5 50% reduction
rate severity, duration, frequency and area of extent of
in pain score in 40 out of 67 (60%). There was complete
mastalgia. Forty out of 88 women (45%) did not
resolution of pain in 18%, no change in 12% and no
return for the second evaluation so that results
were available for 48 out of 88 women (55%). The
showing 550% improvement (x2 [trend] = 6.0, P = 0.01).
There was also some correlation with age – older women
worsening of symptoms. There were highly significant
were more likely to return for the last two visits
reductions in all aspects of breast pain (P50.0001). Of
(r = 0.26, P = 0.007); 47% of women under 45 returned
those completing the second questionnaire, 18 (37%)
for the last two visits compared with 80% of women
reported that they carried out the technique themselves
on a regular basis, 27 (56%) occasionally, and 3 (6%)
As measured by the second questionnaire, improve-
ments were still highly significant in all four categories
The reasons for patients not returning for follow-up
describing degree of response to treatment at the initial
could not be determined. One woman cancelled because
visit (see There was a correlation between the
of complete eradication of pain but others either
final pain scores on the second questionnaire and the
cancelled without giving a reason or simply did not
initial % improvements on the first visit rank correla-
turn up. Those who failed to return for the last two visits
tions for severity, duration, area of extent and frequency
were less likely to have reported improvement after the
being respectively 0.42 (P= 0.005), 0.39 (P = 0.009),
first treatment. Of those who had complete resolution of
0.25 (P = 0.07) and 0.31 (P = 0.03). None of the pain
pain at the first visit, 83% returned for the subsequent
scores were correlated with age or menstrual status.
two treatments compared with 57% of those who had
Again, as with the first questionnaire the improvements
pain relief of between 50% and 99%, and 41% of those
were not of a minor degree. For the different categories,namely severity, duration, area, and frequency of pain65%, 58%, 31%, and 69% respectively of women had
Change in pain score after first treatment
This preliminary study has shown that women treated
with an applied kinesiological technique report signifi-
cant reduction in mastalgia. Immediately after treatment
Changes in pain scores on questionnaire at 2 months after three applied kinesiology treatments
Cases with 550% improvement at first visit (n = 11)*Severity
Cases with 50–99% improvement at first visit (n = 16)*Severity
Cases with 100% improvement at first visit (n = 10)*Severity
Cases with no pain at first visit (n = 10)*Severity
*One case had a pain score of 8 at their initial visit before kinesiology but no pain score following kinesiology at their first visit and so is notincluded in this breakdown.
Applied kinesiology for treatment of women
about 90% had improvement in pain score, with an
Applied kinesiology is a relatively new development
average reduction of approximately 50%. This pain
used by chiropractors, which dates back to 1964.
relief persisted at 2 months. In comparison with other
Holistic and eclectic in approach, it embraces concepts
forms of treatment, such as danazol, bromocriptine and
from other disciplines like nutrition, osteopathy and
tamoxifen, this is achieved with no side-effects and it is
acupunture. Applied kinesiologists have also used a
possible that the benefit may be longer lasting. The
whole range of specialized techniques to deal with such
technique appeared to be equally effective in women
common conditions as physical injuries, backache and
with both moderate and severe mastalgia and in no cases
neck pain, learning difficulties, constipation, mental
stress and emotional problems. This study may pave the
Reassurance alone often improves the lot of women
way for future trials of applied kinesiology for a variety
with breast pain, so it might be argued that the
improvements seen were not a result of the kinesiology.
The long-term effects of applied kinesiology were not
Two factors suggest that this is not the case. Firstly, the
addressed in this study but those cases seen after a
women included in this study had relatively intractable
longer time of follow-up reported continued benefit.
moderate to severe pain. This group might be expected
This study did not compare standard drug treatments
to have a limited response to reassurance alone.
for mastalgia with applied kinesiology. The clear and
Secondly, in this study, the kinesiology treatment
immediate effects of the intervention, together with
produced dramatic improvements in a few minutes at
evidence of continued relief after 2 months suggests that
the first treatment. The women had already seen the
this is a contender for a place in the management of
doctor, and received whatever reassurance he or she had
breast pain. Of course, it is possible that the intervention
to offer. They then came to the kinesiologist and
may work through a complex placebo mechanism. This
documented their pain. After the kinesiology treatment
study did not have a control group, and so this cannot
they documented their pain again, and in the vast
be ruled out, although the rapid improvements in pain
majority there were large improvements, including
score following treatment suggests that this is not the
complete eradication of pain. In addition there was a
case. There is a pressing need to carry out a prospective
correlation between this intial improvement and the
randomized trial, albeit with the proviso that this could
overall improvement documented at the second evalua-
not be a double-blind study. It may however be possible
tion after three treatments. This suggests that the overall
to have one control group where a different area of the
improvements were related to the intial treatment,
body is rubbed, making the treatment effectively blind to
namely the kinesiology. These big and immediate
improvements were therefore not simply a result ofreassurance.
The current authors are sure, although it is difficult to
prove, that the dropouts are a result of many factors
1. Mansel R E, Preece P E, Hughes L E. A double-blind trial of the
prolactin inhibitor bromocriptine in benign breast disease. Br J Surg
operating in these women. As mentioned in the text, one
woman dropped out as a result of her pain having
2. Mansel R E, Wisbey J R, Hughes L E. Controlled trial of the anti-
completely resolved, and others may well also have
gonadotrophin danazol in painful nodular benign breast disease. Lancet 1984; ii: 928–931.
dropped out for this reason. It is also probable that
3. Fentiman I S, Brame K, Caleffi M, Chaudary M A, Hayward J L.
some women didn’t return because the improvements
Double-blind trial of tamoxifen therapy for mastalgia. Lancet 1986;
and/or reassurance that they experienced were suffi-
4. Hamed H, Fogelman I, Smith P, Gregory W, Fenitman I S. Effect
ciently great that they no longer considered their pain an
of a GnRH analogue on bone mass in premenopausal patients with
issue. Elderly women were more likely to return for
mastalgia. The Breast: 1993; 2: 79–82.
subsequent visits, although the reason for this is
5. Boyd N, McGuire V, Shannon P, Fish E, Lickley L. A randomized
trial of low-fat, high carbohydrate diet in patients with cyclical
unclear. They may perhaps be more motivated as
mastopathy. Lancet 1988; ii: 128–132.
they get older. The negative correlation between
6. Preece P, Hanslip J I, Gilbert L et al. Evening primrose oil (Efamol)
returning for their final visit and improvement an initial
for mastalgia. In: Horrobin DF. Clinical Uses of Essential FattyAcids. Montreal: Eden Press 1982.
visit suggests that some may have failed to return
7. Butler B H. Breast Care Manual. Surbiton, Surrey: TASK Books 1993.
because they didn’t experience a sufficiently large
8. Walther D S. Applied Kinesiology. CO, USA: Systems D C 1988.
Jean E.T. McLain, Ph.D. Associate Director, University of Arizona Water Resources Research Center (WRRC) Associate Research Scientist, WRRC and Dept. of Soil, Water and Environmental Science 350 N Campbell Avenue, Tucson, Arizona 85719 My current research is directed towards establishing the public health and environmental safety of reclaimed municipal wastewater, with the goal of extendin
Quellen, weitere Informationen und Literatur: Was kann man tun? Vogelgrippe: Glauben sie nicht alles, was man Ihnen (vor allem Informieren Sie sich bei unabhängigen (!) Stellen (siehe Informations- und Literaturliste!), auch über Forum für Impfproblematik, Gesundheit und die frühere Pocken-Pflichtimpfung und deren z.T. Vertrauen Sie Ihrem gesunden Menschenverstand! Deuts
 The Breast (2001) 10, 15–19# 2001 Harcourt Publishers Ltddoi:10.1054/brst.2000.0176, available online at http://www.idealibrary.com on
Applied kinesiology for treatment of women with mastalgia
W. M. Gregory,1 S. P. Mills,2 H. H. Hamed1 and I. S. Fentiman11Hedley Atkins Breast Unit, Guy’s Hospital, London, UK; 2Association of Systematic Kinesiology, Surbiton,Surrey, UK
S U M M A R Y. To determine whether an applied kinesiology technique was of benefit to women with breast pain,an open pilot study was conducted in which 88 newly presenting women with self-rated moderate or severe mastalgiawere treated by applied kinesiology. This involved a hands-on technique consisting of rubbing a series of ‘lymphaticreflex points’ while touching painful areas of the breasts. The women were predominantly pre-menopausal, andpatients with both cyclical and non-cyclical pain were included in the study. Patients’ self-rated pain scores, bothbefore and immediately after applied kinesiology were compared, together with a further score 2 months later.
The Breast (2001) 10, 15–19# 2001 Harcourt Publishers Ltddoi:10.1054/brst.2000.0176, available online at http://www.idealibrary.com on
Applied kinesiology for treatment of women with mastalgia
W. M. Gregory,1 S. P. Mills,2 H. H. Hamed1 and I. S. Fentiman11Hedley Atkins Breast Unit, Guy’s Hospital, London, UK; 2Association of Systematic Kinesiology, Surbiton,Surrey, UK
S U M M A R Y. To determine whether an applied kinesiology technique was of benefit to women with breast pain,an open pilot study was conducted in which 88 newly presenting women with self-rated moderate or severe mastalgiawere treated by applied kinesiology. This involved a hands-on technique consisting of rubbing a series of ‘lymphaticreflex points’ while touching painful areas of the breasts. The women were predominantly pre-menopausal, andpatients with both cyclical and non-cyclical pain were included in the study. Patients’ self-rated pain scores, bothbefore and immediately after applied kinesiology were compared, together with a further score 2 months later.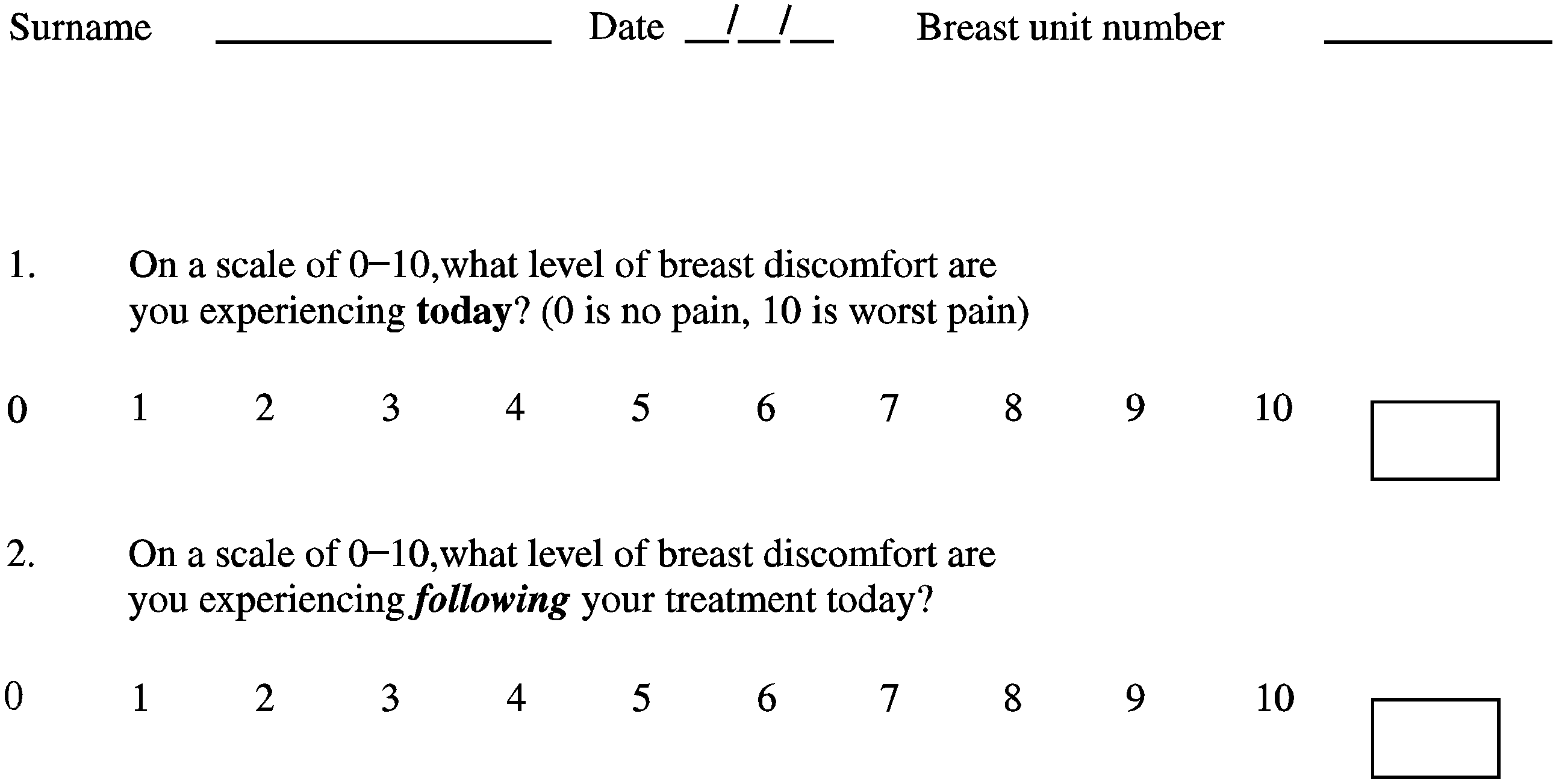 participating was 37 years (range 17–64). Of thepatients, 68 were pre-menopausal, two were perimeno-
All cases had self-rated moderate or severe mastalgia
pausal, six had undergone hysterectomies, and 10 were
with no discrete masses on clinical examination. They
were aged 20–70 years with either cyclical or non-
The patients were seen by just two kinesiologists
cyclical breast pain, and with no evidence of malignancy
(SPM or WMG). The pain evaluation forms were
on mammograms for those aged over 40 years. None
handed out by the kinesiologist and the women
were receiving any other treatment for mastalgia apart
evaluated their pain before and after the treatment.
participating was 37 years (range 17–64). Of thepatients, 68 were pre-menopausal, two were perimeno-
All cases had self-rated moderate or severe mastalgia
pausal, six had undergone hysterectomies, and 10 were
with no discrete masses on clinical examination. They
were aged 20–70 years with either cyclical or non-
The patients were seen by just two kinesiologists
cyclical breast pain, and with no evidence of malignancy
(SPM or WMG). The pain evaluation forms were
on mammograms for those aged over 40 years. None
handed out by the kinesiologist and the women
were receiving any other treatment for mastalgia apart
evaluated their pain before and after the treatment.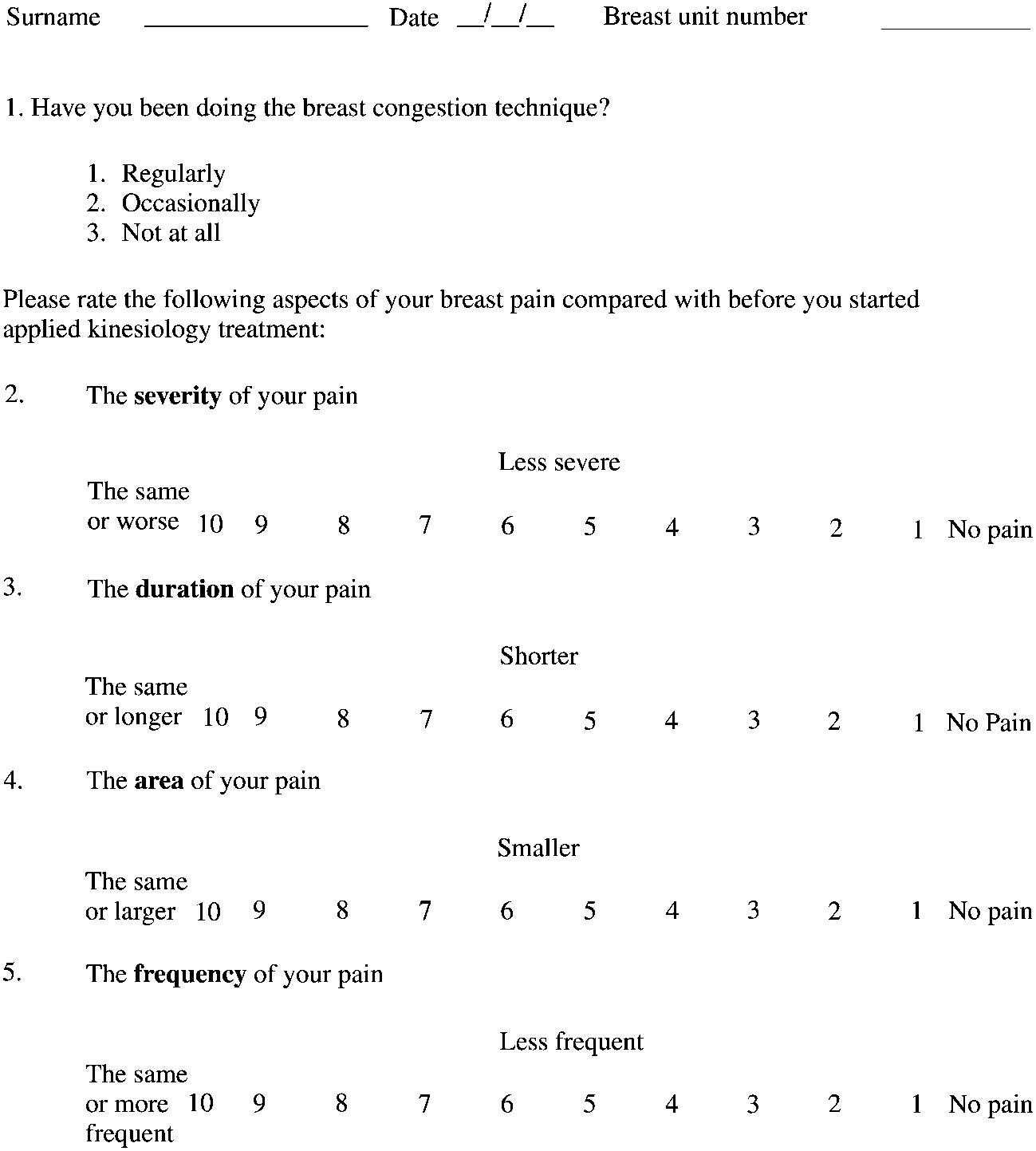 Applied kinesiology for treatment of women
patient experienced an increase of pain after appliedkinesiology.
Applied kinesiology for treatment of women
patient experienced an increase of pain after appliedkinesiology.