Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Doi:10.1016/j.evolhumbehav.2006.03.004
Evolution and Human Behavior 27 (2006) 345 – 356
Age and social position moderate the effect
Jacky Boivina,4, Kathy Sandersb, Lone Schmidtc
aSchool of Psychology, Cardiff University, Cardiff, CF10 3AT Wales, UK
bSchool of Anatomy and Human Biology, University of Western Australia, Crawley WA 6009, Australia
cInstitute of Public Health, Department of Social Medicine, University of Copenhagen, Panum Institute,
Initial receipt 24 October 2005; final revision received 30 March 2006
There is now compelling evidence that psychosocial stress is a cause of reproductive suppression in
humans. However, women continue to conceive in the harshest conditions of war, poverty, or famine,suggesting that suppression can be bypassed. The reproductive suppression model (RSM) proposesthat natural selection should favor factors that reliably predict conditions for reproduction. In thisstudy, we examine two such factors, age and social position, in women undergoing fertility treatment. We hypothesized that stress-related reproductive suppression would be more likely in youngercompared to older women and in women in lower compared to higher social positions. The finalsample consisted of 818 women undergoing fertility treatment. Psychosocial stress and sociodemo-graphic data were collected prior to the start of treatment (Time 1), whereas fertility, as indexed bypregnancy or live birth, was assessed 12 months later (Time 2). The results showed that youngerwomen were four times more likely to suppress than older women, and that unskilled and manualworkers were more likely to suppress than those in middle social positions (e.g., white collar workers). However, significant associations between stress and fertility were also observed for women in highersocial positions (e.g., professionals and executives). The findings provide support for the RSM. D 2006 Elsevier Inc. All rights reserved.
Keywords: Fertility; Infertility; Stress; Reproductive suppression model; IVF
1090-5138/06/$ – see front matter D 2006 Elsevier Inc. All rights reserved. doi:10.1016/j.evolhumbehav.2006.03.004
J. Boivin et al. / Evolution and Human Behavior 27 (2006) 345 – 356
One of the most important life history trade-offs is that between current and future
reproduction). Reproduction, particularly for humans, iscostly, not only because of the requirement for extra nutrients to support pregnancy andlactation, but also in terms of time and the risk to survival because of childbirth. Thus,investment in current reproduction may incur costs that decrease the opportunity for, orsuccess of, future reproductive efforts. But under what environmental conditions is it betterfor the individual’s lifetime reproductive success to defer reproduction? One key assumptionof the reproductive suppression model (RSM)) is that not allenvironmental conditions are equally favorable for investment in reproduction. Similarly, thedevelopmental model of proposes that ovarian function is responsive to thequality of ecological conditions, for example, availability of food resources. These, and other(e.g., flexible response model;), evolutionary models propose that underconditions of environmental stress, reproductive functioning is temporarily suppressedbecause harsh conditions mean that the animal is either unlikely to be able to provideadequately for itself or the offspring, and/or the offspring is unlikely to survive.
The link between stress and reproductive suppression is well established in nonhuman
mammals. In these groups, stress may be indicated by poor resource availability, low socialstatus, competition, and persistent receipt of aggression, and all have been associated withdecrements in reproductive potential Wasser & Barash, 1983). Physiological and demographic studies in humans also demonstratevariations in ovarian function according to the intensity of ecological stressors (for review,).
In addition to ecological highlight the importance of the
psychosocial environment to human survival and reproductive success.(1983), and argue that psychosocialstressors, particularly those that make it difficult to provide adequate care for the child (e.g.,lack of social support, anxiety), should also activate the physiological mechanisms thatsuppress reproductive function. Effects of psychosocial stress on human reproductivefunction have been shown: negative affect (e.g., anxiety, depression) has been associated withlonger cycle lengths) and reduced conception in healthy women tryingto conceive). Further evidence comes from fertility treatment studiesshowing that stress indicators are associated with a poorer ovarian functional response totreatment) and reduced fertilization, implantation, and live birthrates (e.g.,Klonoff-Cohen, Chu, Natarajan, & Sieber, 2001; Sanders & Bruce, 1999a; Smeenk et al.,2001). These associations remain after controlling for obvious confounders, for example,lifestyle (e.g., smoking) and health (e.g., weight) factors& Bruce, 1999a).
Given the harsh realities of life, however, reproductive suppression whenever stress is
experienced would not, in practice, be efficient. Indeed, women continue to conceive in theharshest conditions of war, poverty, or famine. Moreover, despite the converging evidence in
J. Boivin et al. / Evolution and Human Behavior 27 (2006) 345–356
human studies noted previously, not all human studies find an association between stress andfertility potential and/or the effect size varies among studies (e.g., & Mo¨ ller, 2005; Merari, Feldberg, Elizur, Goldman, & Modan, 1992; Sanders & Bruce,1999b). This variability suggests the presence of moderators or constraints on the stress–fertility association.
propose several constraints to reproductive suppression in times
of stress. First, the RSM was based on the relationship of present to future reproductiveconditions with reproductive suppression proposed to be less likely when future reproductiveopportunities were scarce or limited, because the cost of delayed reproduction wouldoutweigh its potential benefits. Consequently, it was proposed that younger women should bemore likely to suppress in times of stress than older women ( & Isenberg, 1986).
Second, because humans are a social species, reproductive suppression should vary
according to the economic and social resources available to the individual because these arefundamental tools in the defense against stressful life events ( p. 531), regardless of future conditions. Individuals with more resources have strongerdefenses and are better able to withstand the physiological effects of stress than those withfewer resources. This is evidenced by, for example, the findings that sustained stress hormoneactivation (e.g., higher baseline cortisol levels) and altered responsivity to stress situations aremore common in individuals from low socioeconomic backgrounds (Sluiter, Starke, & Ursin, 2004), or that socially isolated individuals respond to stress withgreater vascular resistance and slower wound healing than nonisolated individuals (& Hawkley, 2003). Therefore, individuals with poorer resources should be at greater risk forreproductive suppression because they lack environmental bbuffersQ against psychosocialstress (
In the present study, we examine age and social position as moderators of the association
between psychosocial stress and fertility in women undergoing fertility treatment. In thispopulation, the most demanding psychosocial stressor is the fertility problem (FP) itself. Accordingly, stress was defined as the extent to which FPs were perceived to be a threat to theindividual and couple. Fertility-problem stress has been linked with reproductive suppression(i.e., reduced implantation and pregnancy rates) in previous work (e.g., 1995; Klonoff-Cohen et al., 2001 ). We hypothesized that FP stress would be associated withgreater reproductive suppression (i.e., treatment failure) in younger vs. older women. Moreover, we hypothesized that low resources, as indexed by low social position, would beassociated with greater suppression than high social positions.
The final sample consisted of 818 women undergoing treatment at one of five fertility
clinics in Denmark and participating in the Copenhagen Multi-centre Psychosocial Infertility
J. Boivin et al. / Evolution and Human Behavior 27 (2006) 345 – 356
(COMPI)) longitudinal investigation of Danish couples undergoingfertility treatment. The sample consisted of couples who had been referred for fertilitytreatment, with the expectation that they were physically capable of pregnancy withtreatment and who had had at least one cycle of fertility treatment during the 12-monthstudy period. Under the Danish health care system, all couples had equal access tosubsidized treatment. Women who had conceived a child with treatment prior to the start ofthe study, who adopted a child during the study period, and/or who had errors or missingdata in their questionnaires were excluded to increase the homogeneity of the sample. Thefinal sample constituted 76.4% of the initial pool of participating couples (n=1070) atstudy entry.
Women were in their mid-thirties (M=31.5, S.D.=3.5; range, 22 – 40 years) and most,
88.4% (n=723), participated in the labor force. Women had been living with their partnersfor almost 8 years (M=7.6, S.D.=3.6), and the average duration of infertility was 4.09(S.D.=2.12) years. Most couples had had fertility treatment (median, two treatments) prior tostudy entry, but the majority of couples (75.1%, n =614) had no children either together orfrom a previous relationship. Couples with children were not different from those withchildren in their reports of FP stress [t(816)=.14, p =.89] or treatment success rates[v2(1) =.05, p =.83].
Age, social position, and FP stress were assessed at study entry prior to the start of fertility
treatment (Time 1, T1), whereas number of treatments and treatment outcome were assessedat the follow-up assessment 12 months later (Time 2, T2).
2.2.1.1. Fertility-problem stress. The FP stress inventorySchmidt, 1996) was used to assess the overall threat of FPs via ratings of the amount ofdisruption and stress; the FP was perceived to have produced for the individual (e.g., bIt isvery stressful for me to deal with this fertility problemQ) and the marital relationship (e.g.,bFertility problems have caused thoughts of divorceQ). The total score was computed byadding ratings (range, 5–22) with higher scores indicating higher stress.
2.2.1.2. Age and social position. For age, participants provided their year of birth, and thisvariable was converted to a numerical score, which was rounded to the nearest year. Socialposition was based on school education, vocational training, and occupational social class,and is an indicator of both social standing and material reward and resources ). Seven items were combined using a standardized method) to derive threesocial positions. Social Position I comprised unskilled and semiskilled workers (e.g., gasstation attendant); social Position II, white collar and skilled workers (e.g., small-scale self-employed, nurse); and social Position III, professionals and executives (e.g., lawyers, large-scale self-employed). Ninety-five women (11.6%) could not be classified according to this
J. Boivin et al. / Evolution and Human Behavior 27 (2006) 345–356
scheme (i.e., mainly students and people outside of the work force) and were excluded fromsocial position analyses.
2.2.2.1. Treatment outcome. At the 12-month follow-up, participants were asked to indicatewhether they had achieved a pregnancy, and if they had, they were asked whether they werecurrently pregnant or had delivered. Women in the latter two categories comprised thereproductive bsuccessQ group. The remaining women had not achieved a pregnancy, or hadbecome pregnant but had a pregnancy failure (e.g., miscarriage, ectopic). These womencomprised the bno successQ outcome group. We included ongoing pregnancies in thebsuccessQ group because we could not predict whether any of these would result inmiscarriage. However, because only 39 of the ongoing pregnancies were still in the firsttrimester when miscarriage is most likely ( Mouzon, & Nygren, 2005), the number of potential miscarriages was expected to be small(~20% of 39 equals 8) and unlikely to affect the results presented. Participants also indicatedthe number of treatment cycles they had completed between T1 and T2. Treatment includedany type of assisted reproductive intervention [e.g., in vitro fertilization (IVF), insemination].
Infertility clinics were contacted to enlist their participation in the COMPI project, and all
(n =5) agreed to distribute questionnaires. Clinics were provided with questionnaire bookletsand preaddressed stamped envelopes for the return of completed questionnaires. Time 1questionnaires were given to women by clinic staff 2 weeks before the start of treatment. Participants who wished to participate returned completed questionnaires within 10 days,whereas those who did not returned an enclosed nonparticipating form. The procedure for T2data collection was the same, except that questionnaire booklets were mailed directly toparticipants (12 months after Time 1 questionnaires). Data collection occurred betweenJanuary 2000 and August 2001 (T1) and between January 2001 and August 2002 (T2).
Moderation was tested according to the techniques proposed by In
each analysis, the main effect of the potential moderator (i.e., age or social position) wasentered on the first step of the regression analysis alongside the predictor, that is, FP stress. On the second step of the analysis, the product of FP stress and the moderator (i.e.,interaction) were examined. If the specified variable were a moderator, then the interactionterm would be significant. This approach allows one to assess the individual effect of eachpredictor and moderator on the first step and any additional joint effect of predictor andmoderator on the second step of the analysis. Continuous variables (i.e., age, FP stress, and,where applicable, number of treatments between T1 and T2) were transformed to standardscores to reduce colinearity between the main effects and product term. Because social class
J. Boivin et al. / Evolution and Human Behavior 27 (2006) 345 – 356
was a categorical variable with three levels, a set of two dummy variables was created. Thereference category for this set of contrasts was the highest social position (i.e., professionalsand executives). In analyses for social position, age was entered as a covariate to controlfor age effects on fertility.
Treatment outcome (0= no success; 1 =success) was the outcome variable in these
analyses. Because it was dichotomous, logistic regression was used, and the statistics reportedwere the regression coefficient (FS.E.), the Wald statistic, and the probability value. Simpleregression analyses were used to identify the source of significant interactions West, 1991). Analyses with age and social class were repeated, controlling for treatmentexperience before T1, number of treatment cycles between T1 and T2, and type of treatmentundertaken (e.g., IVF vs. insemination), but because these did not substantially alter results ofthe original analyses, the latter are reported.
3.1. Psychological status at Time 1 and treatment outcome at 12-month follow-up (T2)
Fertility-problem stress scores ranged between 5 and 20, and the average score (M=11.14,
S.D.=3.39) indicated that women were reporting moderate levels of FP stress. The majorityof women were in the middle social position (n= 552, 67.5%), with fewer in the low (n=100,12.2%) or high social position (n =71, 8.7%). Fertility-problem stress was not significantlyassociated with age [r(818)=À.039, p =.26] or social position [ F(2,720)=.834, p =.44].
By the 12-month follow-up (T2), women had undergone an average of 2.11 (S.D.=1.19)
treatment cycles. At T2, 59.7% (n =488) of women had become pregnant or had delivered. Women who had become pregnant had had significantly fewer treatments (M=1.83,S.D.=1.14) than those who were unsuccessful (M=2.53, S.D.=1.15) [t(816)=8.56, pb.000].
Logistic analysis was used to examine whether there was an interaction between age
and FP stress in predicting treatment outcome. The overall analysis was significant [modelv2(3)=15.13, p =.002], and the significant main effects indicated that older age [b=À.200F.073, Wald(1)=7.57, p =.006] and greater FP stress [b=À.167F.072, Wald(1)=5.38,p =.020] were associated with treatment failure. The Age by FP stress interaction wasmarginally significant [b = .122F.076, Wald(1) = 2.57, p = .100]. shows the point–biserial correlation between FP stress and treatment outcome for each age between 25 and 38years. As shown, correlations below the median age of 31 were generally more indicative ofsuppression than those above this age. Simple regression follow-up tests revealed thatin younger women (b31 years, n =428), there was a significant suppressive effect ofstress [b=À.292F.106, Wald(1)= 7.61. p =.006], whereas the stress–outcome associationwas not significant in older women (N31 years of age, n=390) [b=À.062F.099, Wald(1)=0.387, p =.534].
J. Boivin et al. / Evolution and Human Behavior 27 (2006) 345–356
Fig. 1. Point–biserial correlation between T1 FP stress and T2 treatment outcome as a function of female age (A)25 to 38 years.
Logistic regression was used to examine the moderating effect of social position on the
stress–fertility association. The logit model was significant [model v2(6) =24.11, pb.000] andas was the case in the previous analysis; the main effects of age [b=À.076F.023,Wald(1)=10.949, p =.001] and FP stress [b=À.193F.078, Wald(1)=6.198, p=.013] were sig-nificant, but the main effect of social position was not [Wald(1)= 2.94, p =.230]. However, theinteraction between social position and FP stress was significant [Wald(2)=6.450, p =.040]. Simple regression follow-up tests revealed that people in lower and higher social positions wereequally likely to suppress, and both did so more than people in the middle social position. Specifically, there was marginally less suppression in people in the middle social position vs. people in (a) the lower [b=À.413F.220, Wald(1)=3.54, p=.060] or (b) higher [b=À.575F.300, Wald(1)=3.68, p = .055] social positions. There was no difference in the stress–fertilityassociation between the lowest and highest social positions [b=.182F.354, ‘Wald(1)=0.264,p=.607]. The point–biserial correlation between FP stress and outcome (controlling for age)was significant for the low [r(97) =À.256, p =.011] and high [r(71)=À.289, p b.015] socialpositions, but not the middle social position [r(549)= À.037, p=.381].
The aim of this study is to identify potential moderators of the association between stress
and fertility potential. According to the RSM, stress conditions, including those associated
J. Boivin et al. / Evolution and Human Behavior 27 (2006) 345 – 356
with psychosocial stressors (e.g., anxiety, depression, and low self-esteem), are expected toproduce lower conception rates). Reproductive suppression isproposed to be adaptive and, in the long term, to lead to increased overall lifetimereproductive success). However, because no organismis advantaged by never conceiving, there should be some constraints on reproductivesuppression. The results of this study provide evidence of reproductive suppression and of thefactors that limit this adaptive strategy.
In line with past evidence, it was found that FP stress was associated with a lower
probability of reproductive success during a 12-month treatment period. This association wasrobust in that it remained significant after controlling for female age, social position, andnumber of treatment cycles. Furthermore, stress ratings were obtained before treatment wasinitiated and, therefore, were not contaminated by perceptions about the success or failure ofthe treatment cycle). Fertility-problem stress, as measured here,indicated the extent to which this medical condition was perceived as threatening to womenbecause it negatively affected their mood, disrupted their marital relations, or created stress intheir everyday life. Reproductive success was defined as an ongoing pregnancy or a live birthwith fertility treatment. The findings are consistent with results showing a decreased live birthrate in women who were highly b reactive Q to infertility) and toresults showing that stress, measured by more general mood states (e.g., depression, anxiety,and hostility), is associated with poorer reproductive outcomesSanders & Bruce, 1999a; Smeenk et al. 2001). In light of the reliability of this effect, thelongitudinal nature of this large-scale study, and the convergence with past research, we feelconfident that this finding demonstrates a genuine psychobiological link between the mentalwell being of the individual and their reproductive functioning.
Stress-induced reproductive suppression has been proposed as an automatic physiological
mechanism to counteract the costs of reproducing in less than ideal conditions Barash, 1983; Ellison, 1990). The mechanisms that trigger reproductive suppression have notbeen fully described but are likely to involve several interacting physiological systemsincluding metabolic signals and activation of the hypothalamic–pituitary–adrenal (HPA) axis). The HPA axis is responsive to a wide range ofpsychosocial, metabolic, and physical stressors (for review see). Moreover, HPA activation has been shown to disrupt the hypothalamic–pituitary–gonadal(HPG) axis by inhibiting the GnRH pulse generator that regulates gonadal function 19 99) . Althou gh the pha rma colo gy of f ertilit y t re atment affe cts t h e n euro end ocr i neenvironment, suppression in women undergoing fertility treatment is expected to alsooperate through modification of HPA–HPG interactions). Stressmay also affect lifestyle factors (e.g., increased smoking, poor diet), but such behavioraleffects do not fully account for stress effects on reproductive function (e.g.,et al., 2001; Sanders & Bruce, 1999a).
It might seem paradoxical that FP stress can perpetuate a lack of fertility in the same way
as do ecological stressors. Moreover, such an effect would seem maladaptive. However, theHPA axis does not appear to discriminate the source of stress triggering its activation,producing the same response across many different types of stressors
J. Boivin et al. / Evolution and Human Behavior 27 (2006) 345–356
1999; Chrousos & Gold, 1992). Indeed, (1992) demonstrated that fertility-related anxiety was capable of producing activation of theHPA axis (e.g., increased cortisol) of the sort reported with other psychosocial stressors (e.g.,bereavement, occupational demand). A system that lacks specificity to the source of stressmay be adaptive because it increases the chance that it will be bturned-onQ at the appropriatetime and, therefore, naturally selected ( We cannot unequivocallysay that this is a maladaptive mechanism because stress reactions to FPs may be indicative ofother psychopathology, which could (eventually) compromise parenting (e.g., postnataldepression) (
Although reproductive suppression in times of stress is a mechanism to redirect valuable
energy away from the costly exercise of pregnancy, deferment of reproduction in favor ofsurvival may itself incur costs if favorable opportunities for future reproduction do not arise. Accordingly, hypothesized that suppression would be less likely inolder women who have fewer remaining reproductive years (and, therefore, presumablyopportunities) than younger women. Consistent with this, we found that the probability ofstress-related suppression decreased with increasing female age. The odds-ratio linking FPstress to treatment outcome was 0.747 in women below or at the median age of 31 years,whereas it was 0.940 in women older than the median age. Thus, for a given level ofperceived stress, the odds of suppression were about four times greater in younger comparedto older women. This effect was not due to fluctuations in the average or variability of FPstress across age groups or age-related variations in sample size.
Age is important because it reflects the greater cost of suppression for older women. All
other factors being equal, older women have fewer remaining reproductive years so that eachreproductive opportunity should be considered precious ( We do nothave direct evidence of the importance of each treatment cycle for women. However, we doknow that in the subgroup of unsuccessful women, those older rated the importance of havingchildren at this time as greater than did younger women [t(300)=3.51, p b.001]. Furthermore,if the remaining reproductive opportunities were the critical factor, then one would expectgreater reproductive suppression in initial vs. later treatment cycles. This was indeed the casein this sample [b=.167F.084, Wald(1)=4.00, p =.048 for interaction between FP stress andtreatment cycles, after taking into account their individual main effects].
also proposed that reproductive suppression would vary
according to economic and social resources. We found a significant link between stress andfertility among those in the lowest social position, which included unskilled and manualworkers. In research among nonhuman mammals, poor resource availability and low socialstatus are both associated with decrements in reproductive function, primarily as aconsequence of increased energetic stress (e.g., 1992). Similarly, several human studies have linked indicators of poor economic resources toreduced ovulatory frequency ( or function ( Our studyextends these findings and shows that social position also moderates the impact ofpsychosocial stress on female reproductive function.
However, we also observed suppression in the highest social position, even after con-
trolling for age and number of treatments cycles. Despite a high level of resources,
J. Boivin et al. / Evolution and Human Behavior 27 (2006) 345 – 356
professionals and executives were as likely to suppress in times of stress as were those in thelowest social position. One possible explanation is that reproductive suppression occurs fordifferent reasons in low and high social positions. In contrast to poor defenses invoked forlow social positions, suppression in higher social positions may be due to the additionalreproductive opportunities this group can create for itself. Although access to treatment is freein Denmark, people with greater economic resources may be able to access other costly waysof achieving parenthood (e.g., specialist treatment in other countries).
Our findings indicate a robust association between stress and fertility, and suggest
possibilities for future research. First, we need more research on the cues that allow theorganism to know when it should proceed with reproduction. Second, the process thattranslates this appraisal or situational awareness into a biological effect needs to beunderstood. How does the human brain communicate to the reproductive system that now is(or is not) a good time to reproduce? Third, given wide variations in baseline levels ofpsychosocial and other ecological stressors), it would be important to examineinterpopulation differences in the typical threshold at which these cues begin to operate.
Several limitations imposed by the design should be noted. The advantages of the clinical
design used in this study is that psychosocial assessments can be taken in advance ofbconception attempts,Q and relevant biological information about the number of attempts andtheir outcome during a specified period can be monitored and easily obtained. However, thereare also drawbacks to this approach. First, from our design, we cannot say whether mentalwell-being was the factor that caused reproductive difficulties to begin with. Second,treatment attempts are emotionally stressful and produce higher stress levels than thatobserved during natural conception cycles), potentially leading toan overestimation of stress effects on fertility. Third and as noted previously, fertilitytreatments modify the endocrine milieu as well as the reproductive context (i.e., treatment vs. sexual intercourse) so that the processes that account for stress effects in couples undergoingfertility treatment may vary according to treatment regimes and differ from those mechanismsinvolved in natural conception cycles. The use of intraindividual comparisons between asuccessful and nonsuccessful reproductive attempt would provide better control fornoncompositional factors that may influence reproductive success. Finally, we focusedexclusively on stress effects in the women being treated, but male partner stress also needs tobe examined because it could impact on reproductive success through direct effects on sexualbehavior or semen parameters) and/or byinfluencing the female partner ’s own perception of stress ). Despite thesedrawbacks, however, we feel that data obtained from this population contribute significantlyto our understanding of stress-induced reproductive suppression.
The infertility cohort is a part of the Copenhagen Multi-centre Psychosocial Infertility
(COMPI) Research Programme initiated by Dr. L. Schmidt, University of Copenhagen, 2000. The program is a collaboration among the public Fertility Clinics at Br&dstrup Hospital; the
J. Boivin et al. / Evolution and Human Behavior 27 (2006) 345–356
Herlev University Hospital; the Juliane Marie Centre, Rigshospitalet; and the OdenseUniversity Hospital. This study has received support from the Danish Health Insurance Fund(Jnr. 11/097-97), the Else and Mogens Wedell–Wedellsborgs Fund, the manager E. Danielsens and Wife’s Fund, the merchant L.F. Foghts Fund, and the Jacob Madsen andWife Olga Madsens Fund.
Abbey, A., Andrews, F. M., & Halman, L. J. (1991). Gender’s role in responses to infertility. Psychology of
Aiken, L. S., & West, S. G. (1991). Multiple regression: Testing and interpreting interactions. Thousand Oaks7
Anderheim, L., Holter, H., Bergh, C., & Mfller, A. (2005). Does psychological stress affect the outcome of in
vitro fertilization? Human Reproduction, 20, 2969 – 2975.
Biondi, M., & Picardi, A. (1999). Psychological stress and neuroendocrine function in humans: The last two
decades of research. Psychotherapy and Psychosomatics, 68, 114 – 150.
Boivin, J., Andersson, L., Shoog-Svanberg, A., Hjelmstedt, A., Collins, A., & Bergh, T. (1998). Psychological
reactions during in vitro fertilisation (IVF): Similar response pattern in husbands and wives. HumanReproduction, 13, 3262 – 3267.
Boivin, J., & Takefman, J. E. (1995). Stress level across stages of in vitro fertilization in subsequently pregnant
and non-pregnant women. Fertility and Sterility, 64, 802 – 810.
Boivin, J., & Takefman, J. E. (1996). The impact of the in vitro fertilization-embryo transfer (IVF-ET) process on
emotional, physical and relational variables. Human Reproduction, 11, 903 – 907.
Cacioppo, J. T., & Hawkley, L. C. (2003). Social isolation and health, with an emphasis on underlying
mechanisms. Perspectives in Biology and Medicine, 46 (Suppl), s39 – s52.
Cameron, J. L. (1997). Stress and behaviorally induced reproductive dysfunction in primates. Seminars in
Reproductive Endocrinology, 15, 37 – 45.
Chisholm, J. S. (1999). Death, hope and sex. Cambridge7 Cambridge University Press. Chrousos, G. P., & Gold, P. W. (1992). The concepts of stress and stress system disorders. Overview of physical
and behavioural homeostasis. Journal of the American Medical Association, 267, 1244 – 1252.
Chrousos, G. P., Torpy, D. J., & Gold, P. W. (1998). Interactions between the hypothalamic–pituitary–adrenal axis
and the female reproductive system: Clinical implications. Annals of Internal Medicine, 129, 229 – 240.
Clarke, R., Klock, S. C., Geoghegan, J., & Travassos, E. (1999). The relationship between psychological stress
and semen quality among in vitro fertilization patients. Human Reproduction, 14, 753 – 758.
deCatanzaro, D., & MacNiven, E. (1992). Psychogenic pregnancy disruptions in mammals. Neuroscience and
Biobehavioral Reviews, 16, 43 – 53.
Demyttenaere, K., Nijs, P., Evers-Kiebooms, G., & Koninckx, P. R. (1992). Coping and the ineffectiveness of
coping influence the outcome of in vitro fertilisation through stress responses. Psychoneuroendocrinology, 17,655 – 665.
Ellison, P. T. (1990). Human ovarian function and reproductive ecology: New hypotheses. American
Ellison, P. T. (1995). Understanding natural variation in human ovarian function. In R. Dunbar (Ed.), Human
reproductive decisions (pp. 22 – 51). New York7 St Martin’s Press.
Facchinetti, F., Matteo, M. L., Artini, G. P., Volpe, A., & Genazzani, A. R. (1997). An increased vulnerability to
stress is associated with a poor outcome of in vitro fertilisation-embryo transfer treatment. Fertility andSterility, 67, 309 – 314.
Ferin, M. (1999). Clinical review 105: Stress and the reproductive cycle. Journal of Clinical Endocrinology and
J. Boivin et al. / Evolution and Human Behavior 27 (2006) 345 – 356
Gallinelli, A., Roncaglia, R., Matteo, M. L., Ciaccio, I., Volpe, A., & Facchinetti, F. (2001). Immunological
changes and stress are associated with different implantation rates in patients undergoing in vitro fertilization-embryo transfer. Fertility and Sterility, 76, 85 – 91.
Hansen, E. J. (1984). Socialgrupper I Danmark [Social class in Denmark]. Copenhagen7 The Danish National
Hjollund, N. H. I., Jensen, T. K., Bonde, J. P. E., Henriksen, T. B., Andersson, A. M., Kolstad, H. A., Ernst, E.,
Giwercman, A., Skakkebaek, N. E., & Olsen, J. (1999). Distress and reduced fertility: A follow-up study offirst-pregnancy planners. Fertility and Sterility, 72, 47 – 53.
Klonoff-Cohen, H., Chu, E., Natarajan, L., & Sieber, W. (2001). A prospective study of stress among women
undergoing in vitro fertilization and gamete intrafallopian transfer. Fertility and Sterility, 76, 675 – 687.
Kristenson, M., Eriksen, H. R., Sluiter, J.K, Starke, D., & Ursin, H. (2004). Psychobiological mechanisms of
socioeconomic differences in health. Social Science and Medicine, 58, 1511 – 1522.
Lancastle, D., & Boivin, J. (2005). Dispositional optimism, trait anxiety, and coping: Unique or shared effects on
biological response to fertility treatment? Health Psychology, 24, 171 – 178.
Lazarus, R. S., & Folkman, S. (1984). Stress, appraisal, and coping. New York7 Springer Publishing Company. Merari, D., Feldberg, D., Elizur, A., Goldman, J., & Modan, B. (1992). Psychological and hormonal changes in
the course of in vitro fertilization. Journal of Assisted Reproduction and Genetics, 9, 161 – 169.
Murray, L., Fiori-Cowley, A., Hooper, R., & Cooper, P. (1996). The impact of postnatal depression and associated
adversity on early mother–infant interactions and later infant outcomes. Child Development, 67, 2512 – 2526.
Nyboe Andersen, A., Gianaroli, L., Felberbaum, R., de Mouzon, J., & Nygren, K. G. (2005). Assisted
reproductive technology in Europe, 2001: Results generated from European registers by ESHRE. HumanReproduction, 20, 1158 – 1176.
Sanders, K.A, & Bruce, N. W. (1997). A prospective study of psychosocial stress and fertility in women. Human
Sanders, K.A, & Bruce, N. W. (1999a). Psychosocial stress and treatment outcome following assisted reproductive
technology. Human Reproduction, 14, 1656 – 1662.
Sanders, K.A, & Bruce, N. W. (1999b). Psychosocial stress and the menstrual cycle. Journal of Biosocial Science,
Schmidt, L. (1996). Psykosociale konsekvenser af infertilitet og behandling [Psychosocial consequences of
infertility and treatment]. Copenhagen7 FADL Book Company.
Schmidt, L., Holstein, B. E., Boivin, J., Tjbrnhbj-Thomsen, T., Blaabjerg, J., Hald, F., Rasmussen, P. E., & Nyboe
Andersen, A. (2003). High ratings of satisfaction with fertility treatment are common: Findings from theCopenhagen Multi-centre Psychosocial Infertility (COMPI) Research Programme. Human Reproduction, 18,2638 – 2646.
Smeenk, J. M. J., Verhaak, C. M., Eugster, A., van Minnen, A., Zielhuis, G. A., & Braat, D. D. M. (2001). The
effect of anxiety and depression on the outcome of in-vitro fertilization. Human Reproduction, 16, 1420 – 1423.
Stearns, S. (1992). The evolution of life histories. New York7 Oxford University Press. Vitzthum, V. J. (2001). Why not so good is still good enough. In P. T. Ellison (Ed.), Reproductive ecology and
human evolution (pp. 179 – 202). New York7 Aldine de Gruyter.
Vitzthum, V. J., Bentley, G. R., Spielvogel, H., Caceres, E., Thornburg, J., Jones, L., Shore, S., Hodges, K. R., &
Chatterton, R. T. (2002). Salivary progesterone levels and rate of ovulation are significantly lower in poorerthan in better-off urban-dwelling Bolivian women. Human Reproduction, 17, 1906 – 1913.
Wasser, S.K, & Barash, D. P. (1983). Reproductive suppression among female mammals: Implications for
biomedicine and sexual selection theory. Quarterly Review of Biology, 58, 513 – 538.
Wasser, S. K., & Isenberg, D. Y. (1986). Reproductive failure among women: Pathology or adaptation? Journal of
Psychosomatic Obstetrics and Gynaecology, 5, 153 – 175.
Wasser, S. K., & Place, N. J. (2001). Reproductive filtering and the social environment. In P. T. Ellison (Ed.),
Reproductive ecology and human evolution (pp. 137 – 157). New York7 Aldine de Gruyter.
Listed below are nonprescription medications that the nurses can give to students only with parent permission. We hope that using these medications, as needed, will reduce both absenteeism and student discomfort while in school. If a student needs routine medications, other arrangements should be made. Medications will be given in age/weight appropriate doses. Please fill out this form, giving y
COMUNE DI VIGONZA (PD) DETERMINAZIONE SETTORE GESTIONE DEL TERRITORIO N. 20 DEL 01/07/2013 UFFICIO: Edilizia Privata, Urbanistica, Catasto OGGETTO: RECUPERO CREDITO NELL'AMBITO DEL RICORSO AL TAR N. 381/2006 - IMPEGNO DI SPESA PER AFFIDAMENTO INCARICO LEGALE ALL'AVV. CARTIA E PREVISIONE INTROITO (CIG ZF80A96553) IL CAPO SETTORE Vista la delibera del C
 Evolution and Human Behavior 27 (2006) 345 – 356
Age and social position moderate the effect
Jacky Boivina,4, Kathy Sandersb, Lone Schmidtc
aSchool of Psychology, Cardiff University, Cardiff, CF10 3AT Wales, UK
bSchool of Anatomy and Human Biology, University of Western Australia, Crawley WA 6009, Australia
cInstitute of Public Health, Department of Social Medicine, University of Copenhagen, Panum Institute,
Initial receipt 24 October 2005; final revision received 30 March 2006
There is now compelling evidence that psychosocial stress is a cause of reproductive suppression in
humans. However, women continue to conceive in the harshest conditions of war, poverty, or famine,suggesting that suppression can be bypassed. The reproductive suppression model (RSM) proposesthat natural selection should favor factors that reliably predict conditions for reproduction. In thisstudy, we examine two such factors, age and social position, in women undergoing fertility treatment.
Evolution and Human Behavior 27 (2006) 345 – 356
Age and social position moderate the effect
Jacky Boivina,4, Kathy Sandersb, Lone Schmidtc
aSchool of Psychology, Cardiff University, Cardiff, CF10 3AT Wales, UK
bSchool of Anatomy and Human Biology, University of Western Australia, Crawley WA 6009, Australia
cInstitute of Public Health, Department of Social Medicine, University of Copenhagen, Panum Institute,
Initial receipt 24 October 2005; final revision received 30 March 2006
There is now compelling evidence that psychosocial stress is a cause of reproductive suppression in
humans. However, women continue to conceive in the harshest conditions of war, poverty, or famine,suggesting that suppression can be bypassed. The reproductive suppression model (RSM) proposesthat natural selection should favor factors that reliably predict conditions for reproduction. In thisstudy, we examine two such factors, age and social position, in women undergoing fertility treatment.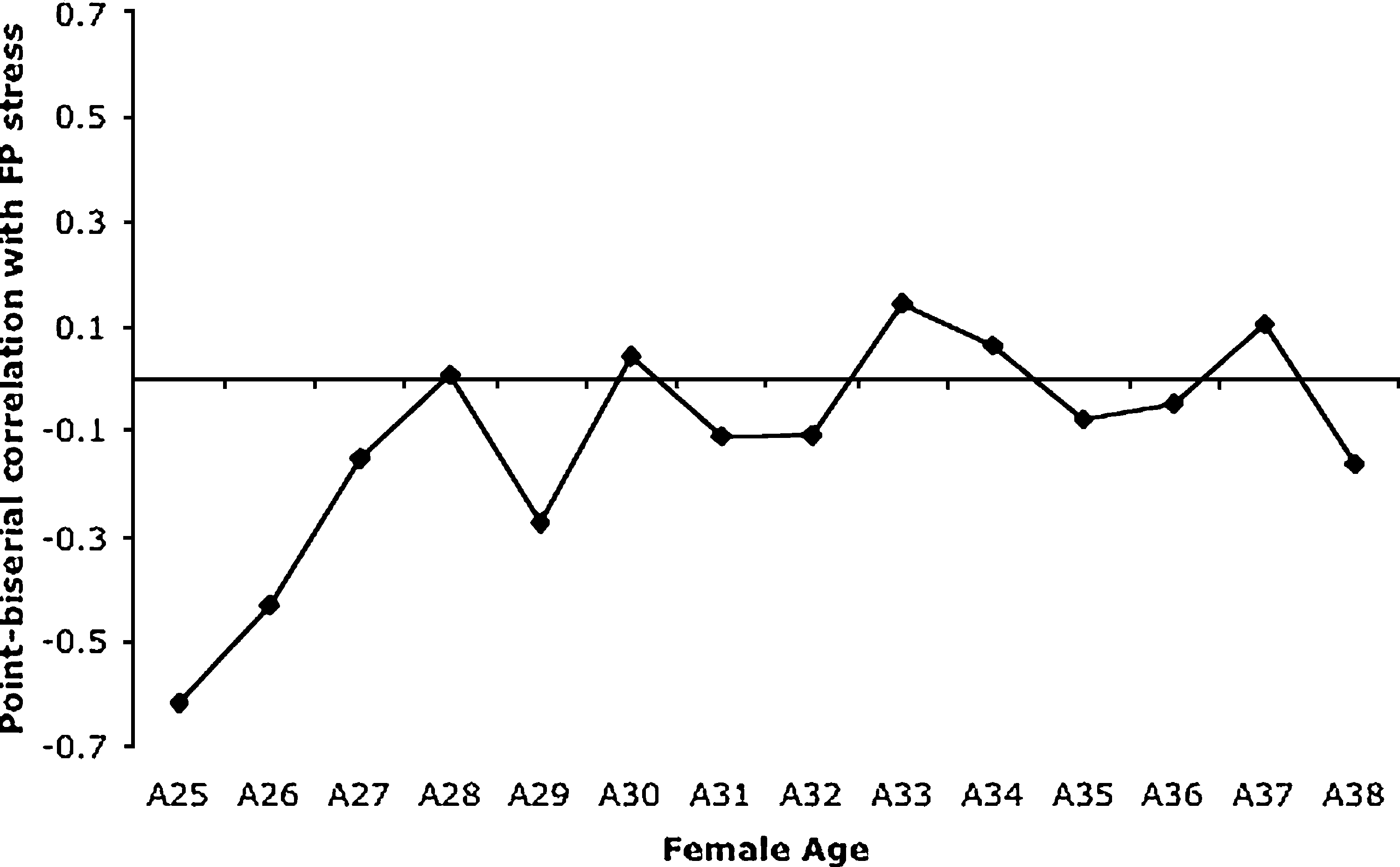 J. Boivin et al. / Evolution and Human Behavior 27 (2006) 345–356
Fig. 1. Point–biserial correlation between T1 FP stress and T2 treatment outcome as a function of female age (A)25 to 38 years.
J. Boivin et al. / Evolution and Human Behavior 27 (2006) 345–356
Fig. 1. Point–biserial correlation between T1 FP stress and T2 treatment outcome as a function of female age (A)25 to 38 years.