Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Pseudo Renal Failure Acute Renal Failure
NSAIDs, CyA/Tacrolimus, ACEI/ARB, Diuretics
ATN – Aminoglycosides, Amphotericin B,
↑ BUN due to protein catabolism
↑ SCr due to competitive inhibition of creatinine
15-35% rise SCr fully expressed after 3 days
More sig in pts with pre-existing renal dysfunction
Completely reversible when drug is discontinued
(J Int Med 1999l246:247-52; TDM 1987;9:161-5)
baseline creatinine 159umol/L; BP 148/92
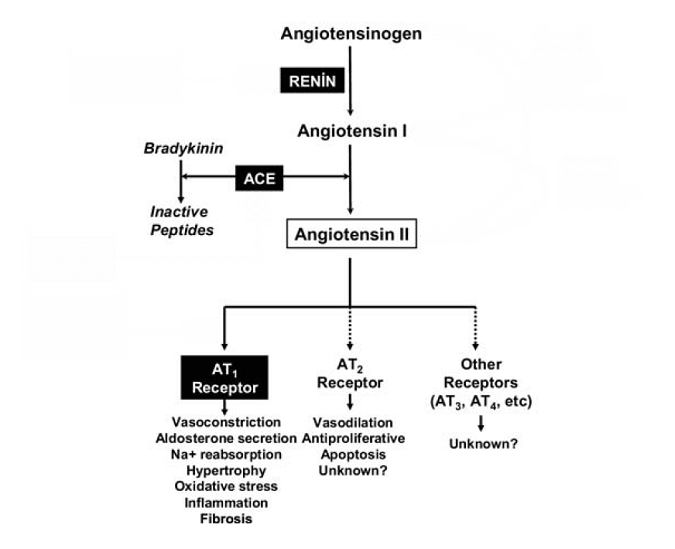
Non-ACE
Ramipril 5 mg daily started and 2 weeks later:
Pathways (e.g. chymase,
Case 2: 82 yo female with osteoarthritis
Admitted to hospital for CAP & dehydration
Meds: Losartan 100mg daily + Naproxen 250mg BID
Benefits of ACEI/ARB: decreased intraglomerular
Glomerular Capillary Pressure → ↑ Permeability → ↑ Proteinuria
Decreased intravascular volume (dehydration,
diuretic overuse, CHF, vomiting, diarrhea)
Use of afferent vasoconstrictor agents
Renal function becomes dependent on sustained
constriction of efferent arteriole from angiotensin II
(NEJM 2002;347:1256-61, Arch Int Med 2000;160:685-93)
Case 1: Creatinine ↑ 159 to 194 in 2 weeks Case 2: Creatinine on admission 250
accept 20-30% increase in serum creatinine within 1-2
umol/L in patient with CAP and dehydration
in fact, this could be an indication that the drugs are
exerting their desired actions to help preserve renal
discontinue NSAID and hold ARB until infection
treated and patient is rehydrated/creatinine
check serum creatinine 1-2 weeks after initiation, then in
resume ARB and monitor serum creatinine
if > 30% change, decrease ACEI/ARB dose by 50% and
repeat Ser Cr in 4 weeks (exclude hypovolemia/NSAIDs,
if > 50% rise in Ser Cr – rule out RAS
repeat serum creatinine in this patient in 1-2 weeks to
Case # 2: Constitutive Inducible
Physician would like to switch previous patient
Selective COX-2 Inhibitors
Are Cox II inhibitors less likely to cause acute
Protection of Gastric Mucosa Renal Effects Pain, Inflammation, Fever Platelet Aggregation Inhibits Platelet Aggregation Note: ASA has an irreversible effect, while other NSAIDS are competitiveIn Vitro Selectivity: COX-2/COX-1 Ratio lumiracoxib rofecoxib etoricoxib valdecoxib > 50-fold COX-2 selective
Use with caution in CKD (grade 3 or greater)
etodolac meloxicam
Inhibit renal vasodilatory prostaglandins E2 & I2
celecoxib 5- 50-fold COX-2 selective diclofenac sulindac
Produced by COX-2 fenoprofen < 5-fold COX-2 selective ibuprofen tolmetin
Higher risk if intravascular volume depletion
naproxen indomethacin
Management: D/C drug, use alternate analgesia
ketoprofen flurbiprofen ketorolac Increasing COX-2 Selective Increasing COX-1 Selective Range of COX Selectivity for COX-1 and COX-2 COX-2/1)
Adapted from: Warner et al. FASEB J. 2004:18:790-804
mediated) or chronic interstitial nephritis
preglomerular arteriolar vasoconstriction or direct
↑ SCr ~ 30% More common in first 6 mos of therapy
Reversible with lowering dose (caution rejection) Monitor blood levels Renal biopsy to distinguish acute CyA
Clinical Features Urinalysis
Tubular epithelial cell damage leading to obstruction of
Diganosis
RF should begin to recover ~7d; Usually reversible and
Non-oliguria > 500mL/day; granular casts in urine
Treatment
related); if persists: Prednisone** (can be dose-related)
Combination therapy with other nephrotoxic drugs
Total cumulative dose; trough levels > 2 mg/L; repeated
courses of A/G therapy; prolonged therapy > 10 days
Other: NSAIDs, PPI, Cimetidine, Contrast Media, Cisplatin
Management – Reversible if D/C drug, adequate
*NSAIDs - onset 2-3mos; no eosinophilia/uria, fever or rash; proteinuria > 3g/24h;
**Reserve if delayed renal recovery (> 1 wk), prolonged exposure to agent (> 2-3 wks)
Theory why once daily A/G therapy works:
Concentration-dependent kill (10x MIC) Post-antibiotic effect
Burns > 20%, Septic Shock, Synergy GFR < 60 mL/min, Dialysis
Proximal tubular A/G update appears to be limited during
Low A/G concs for a greater proportion of dosing interval
Only 1/4 meta-analyses showed reduced nephrotoxicity
(from 7.7% to 5.5%); rest showed no difference
Incidence: ~80% when cumulative dose reaches 2 g
Are Liposomal formulations less nephrotoxic
Direct tubular epithelial cell damage; binds to cell wall
resulting in ↑ tubular permeability and necrosis
↑ SCr, BUN, ↓ Mg, K (urinary wasting) – monitor q1-2d Distal RTA, polyuria (nephrogenic DI)
Combination therapy with other nephrotoxic drugs Total cumulative dose; daily dose > 0.5mg/kg/day Dehydration
Management – Reversible if D/C drug, Hydration (1L NS
Reduced nephrotoxicity by enhancing the delivery to
Voriconazole (~$100
Fluconazole – 1st line for
sites of infection, thus reducing exposure to
Cochrane review April 2000 – all lipid-based preps
decreased the occurrence of nephrotoxicity
Echinocandin
AKI still occurs, esp if concurrent exposure to other
Amphotericin B deoxycholate vs Liposomal
VGH guidelines: only prescribe Ampho B if GFR >
Drawback Liposomal - Very expensive ($440-
Incidence: 40-50% in high risk pts (CKD, DM)
Which is best proven prevention strategy?
Onset: within 12-24 hrs, SCr peaks 2-5 days
o NS 1-2 mL/kg/hr starting 12 hours pre and
after exposure, recovery usually after 4-10 days
Direct tubular necrosis, renal ischemia
o Sodium Bicarbonate 150mEq/L D5W infused at
3mL/kg/h x 1 hours pre, then 1mL/kg/h x 6 hours
Typically non-oliguric (high risk may require HD)
Urinalysis – hyaline and granular casts, low F Na
Risk Factors: DM, CKD, prestudy dehydration
o N-acetylcysteine 600mg PO BID x 4 doses on
Management – Low-osmolality nonionic contrast
day prior to and on day after admin of contrast
agents (eg. Iohexol), smallest dose, Hydration
Recommended Interventions for Prevention of Contrast Nephrotoxicity Contrast Medications Normal Saline Bicarbonate 150 mEq/L D5W post contrast Acetylcysteine
aStrength of Recommendation A, B, C (Good, Moderate, Poor)
Quality of Evidence: 1 (R, Controlled), 2 (R, Cohort), 3 (Expert opinion)
Rhabdomyolysis
Drug insoluble in urine and crystallizes in distal tubule
Intratubular precipitation of myoglobulin
Statins: simvastain, atorvastatin – risk ↑‘ed with Cyp 3A4
inhibitors (clarithromycin, erythro, itraconazole) or
High concentration of drug in tubular fluid
Prevention
↑ amount of drug excreted per functioning nephron
Hold Statin while on clarithro/erythro or itraconazole
Pravastatin, Rosuvastatin not metabolized by CYP 3A4
Dosage adjustment for underlying renal failure Volume expansion to enhance urinary output Urinary alkalinization (for weak acids)
(Drug insoluble in urine and crystallizes in distal tubule)
Methotrexate
Acyclovir
Indinavir
Sulphonamides
Risks/Prevention
Risk/Prevention
Prevention
Risk/Prevention Meperidine metabolite (normeperidine) is neurotoxic and may cause seizures – C/I GFR < 50 mL/min Fentanyl and Methadone preferred for chronic pain
Guo X, Nzerue C. How to prevent, recognize, and treat
drug-induced nephrotoxicity. Clev Clinic J Med
Hydromorphone preferred over Morphine (less 3-
glucuronide metabolite - myoclonus, hallucinations)
Nolin TD, Himmelfarb J. Drug-induced kidney disease. In.
Caution if GFR < 30-60 mL/minute ARF, ↑ K, hypertension
Molony DA, Craig JC (eds). Evidence-based Nephrology.
Sulfonylureas Chlorpropamide –↑’ed half-life, prolongs hypoglycemia Glyburide has active metabolite - ↑ t1/2 hypoglycemia
Bakris GL, Weir MR. ACEI-associated elevations in serum
Gliclazide preferred agent – no active metabolite (needs SA)
creatinine. Is this a cause for concern? Arch Int Med
(glyburide 5mg = gliclazide 80mg = gliclazide MR 30mg)
Metformin
Do not use if GFR < 30-60 mL/min lactic acidosis
Brar SS et al. Sodium bicarbonate for the prevention of
contrast induced-acute kidney injury: A systematic reivew
↓ renal clearance – potential for hypoglycemia
and meta-analysis. Clin J Am Soc Nephrol 2009;4:1584-
Allopurinol
Dosage adjustment; 100mg/day max in Stage 5 (dialysis)
Infectieux - Informations & Publications - Manuel de neurochirurgie - SUPPURATIONS INTRACRÂNIENNES ABCÈS DU CERVEAU Les abcès du cerveau représentent 2% des lésions intra -crâniennes de l'adulte (8% en Inde), 17 % de l'enfant. 35%des abcès se développent avant l'âge de 15 ans. NEUROPATHOLOGIE Topographie . Voisine des cavités ORL ; multiples dans 30% des cas. Exce
B) Disposiciones y Actos Alcaldía "Primero.- Cesar a D. Álvaro Marco Novillo en su cargo de VocalVecino del Grupo Municipal de Izquierda Unida en la Junta Municipal Vecino en la Junta Municipal del Distritode Ciudad Lineal. Segundo.- Nombrar a Dª Cristina Hernández Carrera Vocal Vecinadel Grupo Municipal de Izquierda Unida en la Junta Municipal delDistrito de Moncloa-Aravaca"





 Pseudo Renal Failure Acute Renal Failure
NSAIDs, CyA/Tacrolimus, ACEI/ARB, Diuretics
ATN – Aminoglycosides, Amphotericin B,
↑ BUN due to protein catabolism
Pseudo Renal Failure Acute Renal Failure
NSAIDs, CyA/Tacrolimus, ACEI/ARB, Diuretics
ATN – Aminoglycosides, Amphotericin B,
↑ BUN due to protein catabolism


 Benefits of ACEI/ARB: decreased intraglomerular
Glomerular Capillary Pressure → ↑ Permeability → ↑ Proteinuria
Decreased intravascular volume (dehydration,
diuretic overuse, CHF, vomiting, diarrhea)
Use of afferent vasoconstrictor agents
Renal function becomes dependent on sustained
constriction of efferent arteriole from angiotensin II
(NEJM 2002;347:1256-61, Arch Int Med 2000;160:685-93)
Case 1: Creatinine ↑ 159 to 194 in 2 weeks
Benefits of ACEI/ARB: decreased intraglomerular
Glomerular Capillary Pressure → ↑ Permeability → ↑ Proteinuria
Decreased intravascular volume (dehydration,
diuretic overuse, CHF, vomiting, diarrhea)
Use of afferent vasoconstrictor agents
Renal function becomes dependent on sustained
constriction of efferent arteriole from angiotensin II
(NEJM 2002;347:1256-61, Arch Int Med 2000;160:685-93)
Case 1: Creatinine ↑ 159 to 194 in 2 weeks