Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Vincenzoparisi.it
Graefes Arch Clin Exp Ophthalmol (2011) 249:715–721DOI 10.1007/s00417-010-1612-6
Retinal functional changes measured by frequency-doublingtechnology in patients treated with hydroxychloroquine
Lucia Tanga & Marco Centofanti & Francesco Oddone & Mariacristina Parravano &Vincenzo Parisi & Lucia Ziccardi & Barbara Kroegler & Roberto Perricone &Gianluca Manni
Received: 1 September 2010 / Revised: 20 December 2010 / Accepted: 29 December 2010 / Published online: 21 January 2011
frequency-doubling technology (FDT) in patients treated
Background Antimalarial drugs such as chloroquine (CQ)
and hydroxychloroquine (HCQ) are mainly used in the
Methods Forty-eight eyes of 48 subjects treated with
treatment of rheumatologic diseases, and their use may be
hydroxychloroquine (HCQ), with no signs of retinal
associated with irreversible retinal toxicity. Previous studies
toxicity, and 36 eyes of 36 age and sex-matched healthy
indicate early paracentral visual field loss (Humphrey 10-2)
subjects were enrolled in this cross-sectional, prospective,
in patients taking HCQ". These paracentral defects appear
observational, case control study. Functional testing includ-
before changes in other clinical parameters as visual acuity
ed frequency-doubling Humphrey-matrix perimetry (FDP),
and fundoscopy. The mechanism of CQ toxicity remains
white-on-white Humphrey visual field perimetry (HFA),
unclear. It was reported that toxic doses of CQ administered
using the 24-2 and 10-2 threshold programs, multifocal
for as long as 4.5 years to Rhesus monkeys caused an initial
electroretinogram (mfERG, Veris 4.9) and low contrast
dramatic effect on ganglion cells, followed later by photo-
receptors and RPE degeneration. The purpose of this study
Results FDP mean deviation (MD) was found to be
is to explore early retinal functional changes measured by
significantly reduced in HCQ-treated patients compared tocontrols both in the 24-2 (−1.38±2.41 dB vs 0.21±1.83dB,p<0.01) and in the 10-2 program (−0.97 ±2.88 dB vs 0.15±
The authors have no financial relationships.
1.72dB, p<0.01). FDP pattern standard deviation (PSD)
The authors have the full controls off all primary data and are agree to
was found to be significantly worse in HCQ-treated patients
allow Graefe’s Archives for clinical and Experimental Ophthamology
compared to controls both in the 24-2 (2.70±0.65 dB vs
2.41±0.31 dB, p<0.01 and in the 10-2 program (2.86±
L. Tanga (*) M. Centofanti F. Oddone M. Parravano
0.48 dB vs 2.48 ±0.39 dB, p<0.01). HFA PSD and CS was
also significantly reduced in HCQ patients, while response
Fondazione G.B. Bietti for Study and Research in Ophthalmology,
amplitude densities (RAD) were similar between patients
and controls. A statistically significant difference in the
ratio of the 5°–10° RAD and the 0°–2.5° RAD (0.31±0.08
vs 0.36±0.07 respectively, p<0.05) was found between
M. Centofanti G. ManniUOSD Glaucoma, University of Tor Vergata,
Conclusion Frequency doubling perimetry could be useful
to detect early retinal impairment in patients treated with
B. Kroegler R. PerriconeU.O.C. Reumatologia, Policlinico Tor Vergata,
Keywords Frequency doubling perimetry . Retinal
Graefes Arch Clin Exp Ophthalmol (2011) 249:715–721
Chloroquine (CQ) and hydroxychloroquine (HCQ) are
Patients treated with HCQ for rheumatological diseases
currently used in the treatment of malaria and in treatment
were included in this cross-sectional case-control study.
of rheumatologic diseases such as rheumatoid arthritis,
Healthy subjects were included in the control group. The
systemic lupus erythematosus, sarcoidosis, dermatomyositis
study was carried out in accordance with the Declaration of
Helsinki, was approved by the ethics committee of the
Retinal toxicity represents the major and potentially
institution and written informed consent was obtained from
most serious irreversible side-effect of this type of
treatment, occurring in approximately 10–20% of patients
The inclusion criteria for patients included: treatment
who received CQ and in 3% of patients who received HCQ
with HCQ for at least 3 months, age >18 years and
Hystological analysis of human and animal retinas with
Control subjects needed to meet the following inclusion
CQ toxicity has shown multilamellar structures through the
criteria: no history of treatment with HCQ, age >18 years
retina, followed by loss of retinal ganglion cells (RGCs),
photoreceptors and retinal pigment epilthelium (RPE)
The exclusion criteria were the same for both groups:
atrophy. The accumulation of these multilamellar struc-
spherical refractive error >±6 diopters, astigmatism >±3
tures was thought to result either from inhibition of
diopters, any active or past retinal pathologies (including
lysosomal phospholipases or from inhibition of protein
diabetic retinopathy or age-related macular degeneration),
diagnosis of glaucoma or ocular hypertension (intraocular
Funduscopically, the early stages of retinal toxicity can
pressure >22 mmHg), opacities of optic media that could
be characterized as a reversible loss of foveal reflex,
bias functional and structural retinal testing, history of
followed by a development of abnormalities of the retinal
pigmented epithelium (RPE) associated with paracentral
All subjects underwent a complete ophthalmologic
scotomas, and, in the advanced stage, by the classical bull’s
examination including: best-corrected visual acuity (BCVA)
eye maculopathy, associated with a central scotoma and
with Early Treatment Diabetic Retinopathy Study (ETDRS)
charts at 4 meters, contrast sensitivity (CS) with Multi-
Anatomically, a retinal nerve fiber layer (RNFL) loss has
Contrast Sloan Letter Flip Book at 2 meters testing over a
been shown in patients under long-term CQ treatment
range of contrasts to 100%, 25%, 10%, 5%, 2,5%, 1,25%.
Goldmann applanation tonometry, slit-lamp examination and
Nevertheless, the identification of early functional retinal
indirect ophthalmoscopy were also performed. Functional
impairment of CQ/HCQ retinal toxicity appears to be
testing included frequency-doubling Humphrey-matrix peri-
difficult before the development of anatomic changes at
metry (FDP, Carl Zeiss Meditec), white-on-white Humphrey
fundoscopy and symptomatic loss of vision.
visual field perimetry (HFA, Carl Zeiss Meditec, Dublin,
Examination tests that are commonly used in evalua-
CA, USA), and multifocal electroretinogram (mfERG, Veris
tion of CQ/HCQ retinal toxicity include Amsler grid, VA
4.9). The primary objective was to explore by FDP a
testing, ophthalmoscopy and visual field testing [,
possible retinal sensitivity reduction in HCQ-treated
patients. Secondary objectives included the evaluation of
Standard achromatic perimetry is considered more
additional functional retinal changes at HFA and mfERG,
sensitive in the early detection of functional changes than
and the influence of the duration of the therapy on the
VA, color test and retinal changes at fundoscopy ,
Functional retinal changes, such as contrast sensitivity
] and multifocal electroretinographic (mfERG) response
abnormalities [have been detected at early stages inHCQ-treated patients, even in the preclinical phases.
All enrolled subjects performed two FDP tests within
Recently, frequency-doubling perimetry (FDP) has been
2 weeks using the 24-2 and 10-2 threshold program, in
introduced as a visual field testing technology that allows
order to assess the test–retest variability and to rule out a
selective stimulation of the low redundant magnocellular
relevant learning curve ]. In addition, subjects per-
sub-population of ganglion cells, allowing early detection
formed two white-on-white 24-2 and 10-2 SITA standard
HFA tests. Reliability criteria were defined as fixation
The aim of this study is to explore early retinal
errors <15%, false-positives and false-negatives <15%. If
functional changes measured by frequency-doubling tech-
the second test was unreliable, a third exam was performed
nology (FDT) in patients treated with HCQ.
and considered for statistical analysis. In the case of a third
Graefes Arch Clin Exp Ophthalmol (2011) 249:715–721
unreliable test, the subject was excluded from the study.
a dose of HCQ >6.5 mg/kg//day with those that received a
Mean deviation (MD) and pattern standard deviation (PSD)
dose <6.5 mg/kg/day in our sample population.
values were considered for the analysis.
With 84 patients enrolled in the study, the power to
Contrast sensitivity was performed with Multi-Contrast
detect a 1.5dB difference of FDP mean deviation between
groups was 80%, with a standard deviation of 2.4 and a
These charts are retroilluminated, presented in a dark
type II error set at 0.05. The analysis was performed using
room, and allow testing over a range of contrasts (1.25%,
JMP 7.0 (SAS Institute Inc. Cary, NC, USA)
2.5%, 5%, 10%, 25%, and 100%). They use a logarithmicprogression of letter size (0.1 per row), a constant numberof letters per row, and letters of equal legibility, making task
difficulty constant regardless of the level of acuity tested. Testing was conducted monocularly in the study eye at 2 m
Forty-eight patients treated with HCQ (51.40 ±11.57 years,
under the same mesopic luminance level for all subjects.
range 27–69, M/F 12/36) and 36 age- and sex- matched
Patients were tested with the best optical correction, and
healthy control subjects (47.7±10.50 years, range 27–69,
results are reported as the logarithm of the logMAR.
M/F 7/29) were included in the analysis.
VERIS Clinic™ 4.9 (Electro-Diagnostic Imaging, San
Most of the included patients suffered from rheumatoid
Mateo, CA, USA) was used for mfERG assessment, using a
arthritis (91.7 %), and only four patients (8.3 %) from
previously published method []. In all patient and
control eyes, mfERG was recorded in the presence of
Patients were treated with HCQ at a dosage of 400 mg/
day for an median time of 36 months (range 3.5 months to
The average response amplitude densities (RAD in
nanovolt/degree between the first negative peak, N1,
Age, BCVA and IOP values were similar between
and the first positive peak, P1 obtained from five concentric
anular retinal regions (rings) centered on the fovea were
FDP MD was found to be significantly reduced in HCQ-
analysed. The N1-P1 RADs derived from 0 to 2.5 degrees
treated patients compared to controls, both in the 24-2
(ring 1, R1), from 2.5 to 5 degrees (ring 2, R2), from 5 to
(−1.38±2.41 dB vs 0.21±1.83 dB, p<0.01) and in the 10-2
10 degrees (ring 3, R3), from 10 to 15 degrees (ring 4, R4)
program (-0.97 ±2.88 dB vs 0.15±1.72 dB, p<0.02). The
and from 15 to 20 degrees (ring 5, R5) were also
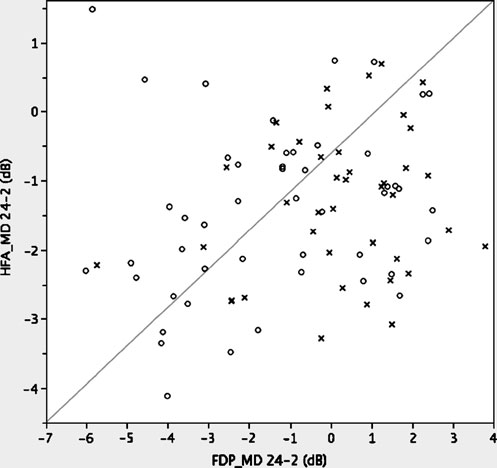
relationship between 24-2 HFA MD and FDP MD is
investigated. Furthermore, the ratio between R3/R1 and
R2/R1 was calculated and compared between groups.
FDP pattern standard deviation (PSD) was found to be
A signal-to-noise ratio of ≥3 was accepted for mfERG
significantly worse in HCQ-treated patients than in controls
both in the 24-2 (2.70 ±0.65 dB vs 2.41±0.31 dB, p<0.01)and in the 10-2 program (2.86±0.48 dB vs 2.48 ±0.39 dB,
HFA PSD was found to be significantly worse in
Demographic and descriptive data were expressed as
HCQ-treated patients compared to controls in 24-2
program (1.54 ± 0.34 dB vs 1.40 ±0.33 dB, p < 0.05) Fig .
Normal distribution of data was assessed by the
HFA MD 24-2, HFA MD 10-2 and HFA PSD 10-2 were
Shapiro–Wilk test. The right eye was arbitrarily chosen
similar between patients and controls.
for statistical analysis. Frequencies of categorical variables
The CS was found to be significantly reduced in HCQ-
were compared between groups by Chi-squared and Fisher’s
treated patients compared to controls at the range of
exact test as appropriate. Comparisons of continuous variablesbetween groups were performed by independent samples
t-test or Mann–Whitney U test as appropriate.
The relationship between functional parameters and
duration of HCQ treatment was explored by linearregression analysis.
It has been reported in the literature that HCQ retinal
toxicity is correlated with the dose of the drug per body
weight, and the American Academy of Opthalmology
considers 6.5 mg/kg/day to be the highest safe dose of
treatment, at least in the first 5 years []. We then
compared retinal sensitivity between patients that received
Graefes Arch Clin Exp Ophthalmol (2011) 249:715–721
FDP and HFA parameters were found to be significantly
different between each HCQ group and controls. Moreover,FDP and HFA parameters were found to be worse inpatients treated for a longer time than in patients treated forashorter time (<36 months).(Tables , )
Furthermore, FDP MD was found to be statistically
significantly different between patients treated with a dosageof HCQ >6.5 mg/kg/day compared to patients treated withlower dosage (−2.43±2.13 vs −0.75±1.95 dB respectively,p<0.05). No significant differences were detected in FDPPSD (2.9±0.65 vs 2.71±0.71 dB respectively p=0.13) or HFAglobal indices (MD: −1.61±1.2 vs 1.52±1.16 dB , p=0.73;PSD: 1.77±0.49 vs 1.47±0.25 dB respectively, p=0.08).
This study supports previous knowledge of an early retinalfunctional impairment in HCQ-treated patients without any
Fig. 1 Scatterplot between frequency-doubling perimetry (FDP) mean
deviation (MD) and Humphrey field analyzer (HFA) MD. HCQ-treated patients are indicated by circles and control subjects by crosses
We found that HCQ-treated patients, without any
clinically detectable RPE abnormalities, showed a de-
contrast of 10% (0.09±0.07 vs 0.04±0.10; p<0.02), 5%
creased threshold of retinal sensitivity as measured by
(0.17±0.10 vs 0.12±0.98; p<0.05), 2.5% (0.31±0.12 vs
FDP and HFA. FDP mean deviation and pattern standard
deviation have been found to be significantly worse in the
In the mfERG no statistically significant difference was
treated patients than in control subjects. Furthermore, we
found at any ring between the two groups in the response
found a reduction of contrast sensitivity, of HFA pattern
amplitude density (RAD): R1 RAD N1-P1 (HCQ patients
standard deviation and of mfERG R3/R1 ring ratio.
84.77±26.60 vs controls 79.31±23.81, p=0.50), R2 RAD
Retinal toxicity is probably due to the inhibition of
N1-P1 (HCQ patients 42.45±11.10 vs controls 42.14±12.98,
lysosomal phospholipases and/or of protein synthesis with
p=0.93), R3 RAD N1-P1 (HCQ patients 25.79±7.15 vs
multilamellar structures accumulation through the retina.
controls 26.73±8.07, p=0.58), R4 RAD N1-P1 (HCQ
Histologically, this accumulation is followed by retinal
patients 17.78±5.90 vs controls 18.68±5.83, p=0.50), R5
ganglion cell loss, photoreceptor loss and RPE atrophy
RAD N1-P1 (HCQ patients 13.85±4.02 vs controls 13.93±4.23, p=0.70). Furthermore, the mean amplitude ratio of R3/R1 and R2/R1 between the groups has been explored, and astatistically significant difference between HCQ-treatedpatients and controls was found for the R/3/R1 ratio (0.31±0.08 vs 0.36±0.07 respectively, p<0.05), but not for the R2/R1 ratio (0.51±0.09 vs 0.54±0.09 respectively, p=0.22).
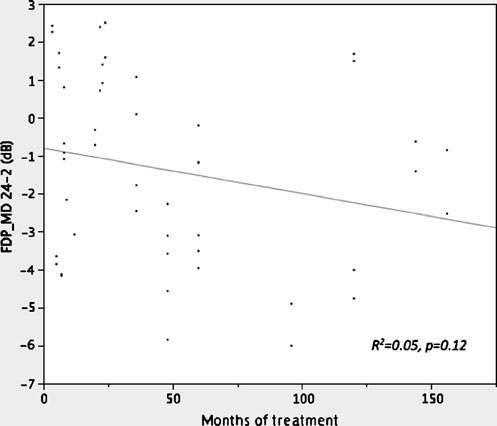
No significant linear relationship was found between any
functional parameters and the duration of therapy. The Rof FDP 24-2 MD and PSD versus treatment durationwas 0.05 (p=0.12) and 0.06 (p=0.09) respectively.
Differences between functional parameters obtained with
FDP, HFA and mfERG were evaluated by dividing thepatients according to the duration of the HCQ therapy. Patients were divided into three groups: patients takingHCQ for less than 36 months (26 patients, group 1), patientstaking HCQ for more than 36 months (22 patients, group 2)and healthy control subjects (36 patients, group 3). The valueof 36 months was chosen as the cut-off time because it was the
Fig. 2 Relationship between frequency-doubling perimetry (FDP)
median value of treatment duration in our sample.
mean deviation (MD) and treatment duration (months)
Graefes Arch Clin Exp Ophthalmol (2011) 249:715–721
Table 2 Comparison between controls and HCQ-treated patients
taking HCQ for more than 36 months (22 patients); group 3: healthy
based on duration of therapy in Humphrey-matrix; group 1: patients
taking HCQ for less than 36 months (26 patients); group 2: patients
Rosenthal et al. reported that toxic doses of CQ adminis-
temporal characteristics of Humphrey-matrix 10-2 test do
tered to Rhesus monkeys caused an initial dramatic effect
not allow to the stimulus to appear to be frequency-
on RGCs, followed by photoreceptor loss and RPE
doubled, so the threshold determination is a flicker
degeneration []. Hallberg et al. found that morphological
sensitivity response, which corresponds to a contrast
and biochemical signs of phospholipidosis were evident
sensitivity test. The changes of Humphrey-matrix 10-2
found in this study are consistent with the results of Bishara
Bonanomi et al. showed that patients under long-term
et al., who showed that contrast sensitivity is reduced in the
CQ treatment could present a significantly reduced RNFL
early phases of retinal toxicity ]. Also the low-contrast
thickness compared to healthy subjects by means of
sensitivity, evaluated with Multi-Contrast Sloan Letter Flip
scanning laser polarimetry GDx Nerve Fibre Analyser
Book at 2 meters, was found to be reduced early in HCQ-
(software v.2.0.01), and that the RNFL loss was correlated
treated patients in the present study.
The Humphrey-matrix parameters showed abnormalities
Clinically advanced retinal toxicity could be easily
even in the presence of normal mfERG;, indeed, no
evaluated with different tests as VA, standard visual field
statistically significant differences have been found be-
testing and ophthalmoscopy, but those tests do not seem to
tween HCQ-treated patients and controls in the RAD in the
detect early stages For this reason, this study explored
mfERG in all rings. In the mfERG, the bioelectrical signal
the possible detection of early functional retinal impairment
is derived from cones and bipolar cells, with smaller
using frequency-doubling technology.
contribution from other retinal neurons. Since RGCs could
The finding of a generalized reduction of retinal
be affected first, even in the absence of a defect in
sensitivity to frequency-doubled stimuli in HCQ-treated
photoreceptor or bipolar cell function, we evaluated the
patients might be related to a higher susceptibility of the
abnormalities in Humphrey-matrix results that selectively
magnocellular RGCs to HCQ; this might be responsible for
study the MGCs. Early HCQ-induced changes could be
the early selective loss of this cell component. Nonetheless,
detected early by detecting changes in the M-y ganglion
another possible explanation is that the MGCs have similar
cell population, which represents a low-redundancy system,
susceptibility to HCQ compared to other RGCs, but are
and therefore could be followed with frequency-doubling
simply less redundant than the whole RGC population, with
no overlap between receptive fields, allowing the earlier
It has been described in the literature that the first
detection of MGC loss if selectively stimulated with
changes in mfERG occur in the paracentral regions, where
the ratio of the rings may be affected [Although the
In this study, patients were tested both 24-2 and 10-2
mean ring amplitudes appeared to be similar in this study
programs with both HFA and FDP. The spatial and
between HCQ and controls, a statistically significant
Table 3 Comparison between controls and HCQ-treated patients based on duration of therapy in HFA. Group 1: patients taking HCQ for lessthan 36 months (26 patients); group 2: patients taking HCQ for more than 36 months (22 patients); group 3: healthy control subjects (36 pts)
Graefes Arch Clin Exp Ophthalmol (2011) 249:715–721
difference was found in the ratio between the outer ring R3
The presence of functional retinal changes in late-stage
and the inner ring R1, supporting the finding of subtle early
HCQ retinopathy could be related to the long duration of
the HCQ therapy, but also to the long duration of the
It should be also highlighted that more sophisticated,
disease. In fact, a limitation of this study is that control
non-conventional methods of stimulation with mfERG have
subjects are healthy, rather than patients with rheumatic
been described as detecting pre-clinical retinal function
changes in HCQ-treated patients, emphasizing second-order
In conclusion, functional retinal testing by frequency-
adaptational effects such as modulated multifocal flashes
doubling perimetry could be useful for the identification of
with interleaved global flashes, as previously described in
early retinal impairment in HCQ-treated patients without
any sign of clinically detectable retinal abnormalities,
No statistically significant relationship between func-
although broader diagnostic studies are required to accu-
tional data versus treatment duration was found, as explored
rately assess its sensitivity and specificity in clinical
by linear regression analysis in the present study. Never-
settings, for screening purposes and follow-up.
theless, a difference in functional parameters between long-term treated and short-term treated patients was found,indicating that there might be a threshold effect of treatment
duration on visual function change, rather than a linearcontinuous effect causing a continuous decay over time.
1. Rynes RI (1997) Antimalarial drugs in the treatment of rheumato-
Nevertheless, despite the fact that the spectrum of treatment
logical diseases. Br J Rheumatol 36:799–805
duration was broad in our sample population (3.5 to
2. Mavrikakis I, Sfikakis PP, Mavrikakis E, Rougas K, Nikolaou A,
156 months), most of the patients were treated between
Kostopoulos C, Mavrikakis (2003) The incidence of irreversible
3.5 and 50 months (32/48) and only 16/48 for a longer
retinal toxicity in patient treated with hydroxychloroquine: areappraisal. Ophthalmology 110:1321–1326
time, indicating that the lack of relationship found between
3. Levy GD, Munz SJ, Paschal J, Cohen HB, Pince KJ, Peterson T
functional data and HCQ treatment duration should be
(1997) Incidence of hydroxychloroquine retinopathy in 1,207
patients in a large multicenter outpatient practice. Arthritis Rheum
Furthermore, the patients_ stratification according to the
4. Tzekov R (2005) Ocular toxicity due to chloroquine and
duration of the therapy indicated that patients that assumed
hydroxychloroquine: electrophysiological and visual function
therapy for a short period of time showed only minimal
retinal functional changes, compared to larger changes
5. Marmor MF, Carr RE, Easterbrook M, Farjo AA, Mieler WF,
observed in patients taking therapy over a longer period of
Academy A, American Academy of Ophthalmology (2002)Recommendations on screening for chloroquine and hydroxy-
time. Moreover, previously published studies reported that
chloroquine retinopathy: a report by the American Academy of
retinal toxicity related to HCQ treatement is related to the
Ophthalmology. Ophthalmology 109:1377–1382
daily dosage per kg of body weight, and the American
6. Hallberg A, Naeser P, Andersson A (1990) Effects of long-term
Academy of Opthalmology considers 6.5 mg/kg/day to be
chloroquine exposure on the phospholipids metabolism in retinaand pigment epithelium of the mouse. Acta Ophthalmol (Copenh)
the highest safe dose of treatment, at least in the first
5 years []. In our study, the prescribed dose is constant
7. Rosenthal AR, Kolb H, Bergsma D, Huxsoll D, Hopkins JL
(400 mg/day), and we assume that patients are fully
(1978) Choroquine retinopathy in the rhesus monkey. Invest
compliant, but this could be a source of error in the
8. Easterbrook M (1999) Detection and prevention of maculop-
evaluation of the relationship between retinal toxicity and
athy associated with antimalarial agents. Int Ophthalmol Clin
The results of our study indicate that retinal sensitivity as
9. Carr RE, Gouras P, Gunkel RD (1966) Chloroquine retinopathy.
expressed by FDP MD in patients treated with a daily
Early detection by retinal threshold test. Arch Ophthalmol75:171–178
dosage >6.5 mg/kg is reduced compared to patients treated
10. Pasadhika S, Fishman GA (2010) Effects of chronic exposure to
with lower daily dosages, while no differences were
hydroxychloroquine or chloroquine on inner retinal structures.
detected for other retinal function measures.
The Humphrey-matrix changes are present in the early
11. Bonanomi MT, Dantas NC, Medeiros FA (2006) Retinal nerve
fibre layer thickness measurements in patient using chloroquine.
phases, and they could be considered as good candidates
for an early detection of the HCQ retinopathy and for its
12. Browning DJ (2002) Hydroxychloroquine retinopathy: screening
for drug toxicity. Am J Ophthalmol 133:649–656
The differences in FDP values found in this study are
13. Elder M, Rahman AM, McLay J (2006) Early Paracentral Visual
Field Loss in Patients Taking Hydroxychloroquine. Arch Oph-
moderate. This is a limitation for their use in clinical
practice, even if these results are consistent with pathoge-
14. Bishara SA, Matamoros N (1989) Evaluation of several tests in
netic mechanism of HCQ retinal toxicity.
screening for chloroquine maculopathy. Eye 3:777–782
Graefes Arch Clin Exp Ophthalmol (2011) 249:715–721
15. Maturi RK, Yu M, Weleber RG (2004) Multifocal electroretino-
macular drusen in age-related macular degeneration. Prognosis
graphic evaluation of long-term hydroxychloroquine users. Arch
and risk factors. Ophthalmology 1101:1522–1528
20. Parisi V, Perillo L, Tedeschi M, Scassa C, Gallinaro G,
16. Lai TY, Chan WM, Li H et al (2005) Multifocal electroretino-
Capaldo N, Varano M (2007) Macular function in eyes with
graphic changes in patients receiving hydroxychloroquine therapy.
early age-related macular degeneration with or without contra-
lateral late age-related macular degeneration. Retina 27:879–
17. Johnson CA, Cioffi GA, Van Buskirk EM (1999) Frequency-
doubling technology perimetry using 24-2 stimulus presentation
21. Lyons JS, Severns ML (2007) Detection of early hydroxy-
chloroquine retinal toxicity enhanced by ring ratio analysis of
18. Centofanti M, Fogagnolo P, Oddone F, Orzalesi N, Vetrugno M,
multifocal electroretinography. Am J Ophthalmol 143(5):801–
Manni G, Rossetti L (2008) Learning effect of humphrey matrix
frequency doubling technology perimetry in patients with ocular
22. Penrose PJ, Tzekov RT, Sutter EE, Fu AD, Allen AW Jr, Fung
WE, Oxford KW (2003) Multifocal electroretinography evalua-
19. Holz FG, Wolfensberger TJ, Piguet B, Gross-Jendroska M, Wells
tion for early detection of retinal dysfunction in patients taking
JA, Minassian DC, Chisholm IH, Bird AC (1994) Bilateral
hydroxychloroquine. Retina 23(4):503–512
Attenuation of SSRI-induced increases in extracellular brain 5-HT by benzodiazepines Chapter 8 Attenuation of SSRI-induced increases in extracellular brain 5-HT by benzodiazepines. Abstract Enhanced serotonergic neurotransmission is generally thought to be the neurochemical basisof the antidepressant effects of Selective Serotonin Reuptake Inhibitors (SSRIs). The anxiolytic benzodiaz
What do the threshold learning outcomes in pharmacy mean Introduction to questionnaire design and analysis James Green and Pauline Norris Hunter Centre Computer Lab Conference Opening / Mihi Whakatau (Hunter Centre Atrium, Cnr Frederick & Great King Streets) Mark Brunton, Research Manager Māori, University of Otago Peter Crampton, Pro-Vice-Chancellor, Health Sciences, Dunedin School of M
 Graefes Arch Clin Exp Ophthalmol (2011) 249:715–721
FDP and HFA parameters were found to be significantly
different between each HCQ group and controls. Moreover,FDP and HFA parameters were found to be worse inpatients treated for a longer time than in patients treated forashorter time (<36 months).(Tables , )
Furthermore, FDP MD was found to be statistically
significantly different between patients treated with a dosageof HCQ >6.5 mg/kg/day compared to patients treated withlower dosage (−2.43±2.13 vs −0.75±1.95 dB respectively,p<0.05). No significant differences were detected in FDPPSD (2.9±0.65 vs 2.71±0.71 dB respectively p=0.13) or HFAglobal indices (MD: −1.61±1.2 vs 1.52±1.16 dB , p=0.73;PSD: 1.77±0.49 vs 1.47±0.25 dB respectively, p=0.08).
Graefes Arch Clin Exp Ophthalmol (2011) 249:715–721
FDP and HFA parameters were found to be significantly
different between each HCQ group and controls. Moreover,FDP and HFA parameters were found to be worse inpatients treated for a longer time than in patients treated forashorter time (<36 months).(Tables , )
Furthermore, FDP MD was found to be statistically
significantly different between patients treated with a dosageof HCQ >6.5 mg/kg/day compared to patients treated withlower dosage (−2.43±2.13 vs −0.75±1.95 dB respectively,p<0.05). No significant differences were detected in FDPPSD (2.9±0.65 vs 2.71±0.71 dB respectively p=0.13) or HFAglobal indices (MD: −1.61±1.2 vs 1.52±1.16 dB , p=0.73;PSD: 1.77±0.49 vs 1.47±0.25 dB respectively, p=0.08).