Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Microsoft word - lyrinel pi jul12 cl.doc
ו קדבנ ונכותו תואירבה דרשמ י ע
MEDICINAL PRODUCT Tradename LYRINEL 5mg, 10mg® International Non-Proprietary Name QUALITATIVE AND QUANTITATIVE COMPOSITION
Each extended [prolonged] release tablet contains 5 mg or 10 mg of oxybutynin chloride
3. PHARMACEUTICAL
Extended [prolonged] release tablets for oral use:
• 5 mg: Pale yellow, round, tablet with “5 XL” printed on one side with black ink. • 10 mg: Pink, round, tablet with “10 XL” printed on one side with black ink.
4. CLINICAL PARTICULARS 4.1. Therapeutic Indications
Once daily controlled-release tablet indicated for the treatment of overactive bladder with symptoms of urge urinary incontinence, urgency and frequency.
4.2. Posology and Method of Administration LYRINEL is administered orally once daily.
The recommended starting dose of LYRINEL is 5 or 10 mg once daily. Dosage may be adjusted in 5-mg increments to achieve a balance of efficacy and tolerability (up to a maximum of 30 mg/day). In general, dosage adjustment may proceed at approximately weekly intervals.
[Patients already taking immediate release oxybutynin may be switched to the nearest equivalent total daily dose of LYRINEL.]
LYRINEL must be swallowed whole with the aid of liquids, and must not be chewed, divided, or crushed.
LYRINEL may be administered with or without food (see Section 5.2, Pharmacokinetic Properties).
Elderly[≥65 years old]: 4.3. Contraindications LYRINEL is contraindicated:
- Hypersensitivity to oxybutynin or any of the excipients
- Narrow-angle glaucoma or shallow anterior chamber
- Gastrointestinal obstructive disorder, paralytic ileus or intestinal atony
- Urinary frequency and nocturia due to heart or renal failure
4.4. Special Warnings Special Precautions for Use
Oxybutynin is associated with anticholinergic central nervous system (CNS) effects (See Section 4.8 Undesirable Effects). Patients should be monitored for signs of anticholinergic CNS effects, particularly in the first few months after beginning treatment or increasing the dose. If a patient experiences anticholinergic CNS effects, dose reduction or drug discontinuation should be considered.
Angioedema of the face, lips, tongue and/or larynx has been reported with oxybutynin. In some cases, angioedema occurred after the first dose. Angioedema associated with upper airway swelling has the potential to become life-threatening. If involvement of the tongue, hypopharynx, or larynx occurs, oxybutynin should be promptly discontinued and appropriate therapy and/or measures necessary to ensure a patent airway should be promptly provided.
Heat prostration (fever and heat stroke due to decreased sweating) can occur when anticholinergics such as oxybutynin chloride are administered in the presence of high environmental temperature.
Because anticholinergic agents such as oxybutynin may produce drowsiness (somnolence) or blurred vision, patients should be advised to exercise caution.
LYRINEL should be given with caution in patients with the following conditions:
• hepatic or renal impairment; • clinically significant bladder outflow obstruction because of the risk of urinary
retention (see Section 4.3, Contraindications);
• gastrointestinal obstructive and gastrointestinal motility disorders because of risk of
gastric retention (see Section 4.3, Contraindications);
• conditions such as ulcerative colitis due to the potential for decreased gastrointestinal
• myasthenia gravis due to the risk of symptom aggravation; • gastroesophageal reflux and/or who are concurrently taking drugs (such as
bisphosphonates) that can cause or exacerbate esophagitis;
• preexisting severe gastrointestinal narrowing (pathologic or iatrogenic); • preexisting dementia treated with cholinesterase inhibitors due to the risk of
TRADENAME must be swallowed whole with the aid of liquids, and must not be chewed, divided, or crushed. The medication is contained within a nonabsorbable shell designed to release the drug at a controlled rate. The tablet shell is eliminated from the body; patients should not be concerned if they occasionally notice something that looks like a tablet in their stool.
Oxybutynin hydrochloride is not recommended for use in children below age 5 years due to insufficient data on safety and efficacy.
There is limited evidence supporting the use of Oxybutynin in children with monosymptomatic nocturnal enuresis (not related to detrusor overactivity).
In children over 5 years of age, Oxybutynin hydrochloride should be used with caution as they may be more sensitive to the effects of the product, particularly the CNS and psychiatric adverse reactions.
4.5. Interactions with Other Medicinal Products and Other Forms of Interaction
The concomitant use of oxybutynin with other anticholinergic medicinal products or drugs with anticholinergic activity, such as amantadine and other anticholinergic antiparkinsonian drugs (e.g. biperiden, levodopa), antihistamines, antipsychotics (e.g. phenothiazines, butyrophenones, clozapine), quinidine, tricyclic antidepressants, atropine and related compounds like atropinic antispasmodics, dipyridamole, may increase the frequency or severity of dry mouth, constipation and drowsiness.
Anticholinergic agents may potentially alter the absorption of some concomitantly administered drugs due to anticholinergic effects on gastrointestinal motility. They may also antagonize the gastrointestinal prokinetic effects of metoclopramide and domperidone. However, the interaction between prokinetics and oxybutynin has not been established.
Sublingual nitrates may fail to dissolve under the tongue owing to dry mouth, resulting in reduced therapeutic effect.
Oxybutynin is metabolised by cytochrome P450 isoenzyme CYP3A4. Mean oxybutynin chloride concentrations were approximately 2 fold higher when Lyrinel XL was administered with ketoconazole, a potent CYP3A4 inhibitor. Other inhibitors of cytochrome P450 3A4 enzyme system, such as antimycotic agents (e.g. itraconazole and fluconazole) or macrolide antibiotics (e.g. erythromycin), may alter oxybutynin pharmacokinetics. The clinical relevance of such potential interaction is not known. Caution should be used when such drugs are co-administered.
4.6. Pregnancy and Lactation Reproduction studies with oxybutynin chloride in the mouse, rat, hamster, and rabbit showed no evidence of impaired fertility or harm to the animal fetus. The safety of LYRINEL administered to women who are or who may become pregnant has not been established. Consequently, risks and potential benefits should be considered before this drug is administered to pregnant patients.
It is not known whether oxybutynin is excreted in human milk. Caution should be exercised if LYRINEL is administered to a nursing woman.
4.7. Effects on Ability to Drive and Use Machines No studies have been performed on the effect of LYRINEL on the ability to drive and use machines. Because anticholinergic agents such as oxybutynin may produce drowsiness (somnolence) or blurred vision, patients should be advised to exercise caution. 4.8. Undesirable
The table below reflects the data obtained with Lyrinel XL in clinical trials and from postmarketing experience. In clinical trials with Lyrinel XL (n=1006), adverse events were associated mainly with the anticholinergic actions of oxybutynin. Adverse events were generally dose related. As with other oxybutynin formulations, dry mouth was the most frequently reported adverse reaction. However, in clinical studies, dry mouth has been less frequently reported with Lyrinel XL than with oxybutynin immediate release formulations. For patients who required final doses of 5 or 10 mg of Lyrinel XL, the relative incidence of dry mouth that occurred at any dose level was 1.8 times lower compared with patients who required final doses > 10 mg.
Uncommon Not Known* 1/100 to <1/10 1/1,000 to 1/10,000 to <1/100 <1/1000 Infections infestations
cystitis, pharyngitis, nasopharyngitis, upper respiratory tract infection,, bronchitis, sinusitis,
Blood and Lymphatic disorders: Disorders Metabolism & Nutrition Disorders Psychiatric disorders Disorders Eye disorders disorders
bradycardia, bundle branch block, nodal arrhythmia, supraventricular extrasystoles
Vascular disorders Respiratory, thoracic and mediastinal disorders Gastrointesti nal Disorders mouth
gastroesophagea stomatitis gastroenteritis l reflux disease,
gastric atony, tongue disorder, tongue oedema
dry skin, pruritus acne, urticaria, hair disorder,
subcutaneous disorders Musculoskele connective tissue disorders Renal and disorders Reproductive system and disorders disorders and administratio conditions Investigations
blood aspartate, aminotransferase increased, blood alanine aminotransferase increased
poisoning and procedural complications
*Cannot be estimated from the available clinical data.
Undesirable effects noted with other oxybutynin hydrochloride formulations:
In addition, cyclopegia, mydriasis and suppression of lactation have been reported with the use of other oxybutynin hydrochloride formulations. 4.9. Overdose The symptoms of overdose with oxybutynin progress from an intensification of the usual CNS disturbances (from restlessness and excitement to psychotic behaviour), circulatory changes (flushing, fall in blood pressure, circulatory failure etc.), respiratory failure, paralysis and coma.
2) physostigmine by slow intravenous injection:
Fever should be treated symptomatically with tepid sponging or ice packs.
In pronounced restlessness or excitation, diazepam may be given by intravenous injection. Tachycardia may be treated with intravenous propranolol and urinary retention managed by bladder catheterisation.
In the event of progression of curare-like effects to paralysis of the respiratory muscles, mechanical ventilation will be required.
The continuous release of oxybutynin from Lyrinel XL should be considered in the treatment of overdose. Patients should be monitored for at least 24 hours.
5. PHARMACOLOGICAL PROPERTIES 5.1. Pharmacodynamic Properties
[Pharmacotherapeutic group: ATC code: G04B D04 Urologicals]
Oxybutynin chloride is a synthetic tertiary amine with direct spasmolytic and anticholinergic action on the smooth musculature of the detrusor muscle of the bladder. It increases bladder capacity, reduces the frequency of uninhibited detrusor contractions, and delays the first urge to urinate. Oxybutynin thus decreases the symptoms of urinary incontinence due to either idiopathic detrusor instability or detrusor hyperreflexia.
5.2. Pharmacokinetic Properties Absorption
Following the first dose of LYRINEL , oxybutynin plasma concentrations rise for 4 to 6 hours; thereafter steady concentrations are maintained for up to 24 hours, minimizing fluctuations between peak and trough concentrations associated with oxybutynin immediate release formulations.
The relative bioavailabilities of R- and S-oxybutynin from LYRINEL are 156% and 187%, respectively, compared with oxybutynin. The mean pharmacokinetic parameters for R- and S-oxybutynin are summarized in Table [4 or 5]. The plasma concentration-time profiles for R-and S-oxybutynin are similar in shape. Table [4 or 5] Mean (SD) R- and S-Oxybutynin Pharmacokinetic Parameters Following a Single Dose of LYRINEL 10 mg (n=43) Parameters R-Oxybutynin S-Oxybutynin
Steady-state oxybutynin plasma concentrations are achieved by Day 3 of repeated TRADENAME dosing, with no observed drug accumulation or change in oxybutynin and desethyloxybutynin pharmacokinetic parameters.
LYRINEL steady-state pharmacokinetics was studied in 19 children aged 5-15 years withdetrusor overactivity associated with a neurological condition (e.g., spina bifida). Thechildren were on LYRINEL total daily dose ranging from 5 to 20 mg (0.10 to 0.77 mg/kg). Sparse sampling technique was used to obtain serum samples. When all available data arenormalized to an equivalent of 5 mg per day LYRINEL, the mean pharmacokineticparameters derived for R- and S-oxybutynin and R- and S-desethyloxybutynin are summarizedin Table [5 or 6]. The plasma-time concentration profiles for R- and S-oxybutynin are similarin shape; Figure 1 shows the profile for R-oxybutynin when all available data are normalizedto an equivalent of 5 mg per day. Table [5 or 6] Mean ± SD R- and S-Oxybutynin and R- and S-Desethyloxybutynin Pharmacokinetic Parameters in Children Aged 5-15 Following Administration of 5 to 20mg LYRINEL Once Daily (N=19) All Available Data Normalized To An Equivalent of LYRINEL 5 mg Once Daily R-Oxybutynin S-Oxybutynin R-Desethyl-oxybutynin S-Desethyl-oxybutynin Figure 1 Mean steady state (±SD) R-oxybutynin plasma concentrations following administration of 5 to 20 mg LYRINEL once daily in children aged 5-15. All available data normalized to an equivalent of LYRINEL 5 mg once daily
Based on two separate pharmacokinetic studies that evaluated the concomitant use of LYRINEL with an antacid and with a proton pump inhibitor, drugs that increase gastric pH do not affect the release of drug from the tablet or resulting plasma concentrations of oxybutynin and its metabolite, desethyloxybutynin.
Dose Proportionality
Pharmacokinetic parameters of oxybutynin and desethyloxybutynin (Cmax and AUC) following administration of 5-20 mg of LYRINEL are dose proportional.
Distribution
Oxybutynin is widely distributed in body tissues following systemic absorption. The volume of distribution is 193 L after intravenous administration of 5 mg oxybutynin chloride . Both enantiomers of oxybutynin are highly bound (>99%) to plasma proteins. Both enantiomers of desethyloxybutynin are also highly bound (>97%) to plasma proteins. The major binding protein is alpha-1 acid glycoprotein.
Metabolism and Excretion
Oxybutynin is metabolized primarily by the cytochrome P450 enzyme systems, particularly CYP3A4 found mostly in the liver and gut wall. Its metabolic products include phenylcyclohexylglycolic acid, which is pharmacologically inactive, and desethyloxybutynin, which is pharmacologically active. Following LYRINEL administration, plasma concentrations
of R- and S-desethyloxybutynin are 73% and 92%, respectively, of concentrations observed with oxybutynin.
Oxybutynin is extensively metabolized by the liver, with less than 0.1% of the administered dose excreted unchanged in the urine. Also, less than 0.1% of the administered dose is excreted as the metabolite desethyloxybutynin.
Food Effects
The rate and extent of absorption and metabolism of oxybutynin are similar under fed and fasted conditions.
Special Populations Gender: There are no significant differences in the pharmacokinetics of oxybutynin in healthy male and female volunteers following administration of LYRINEL.
Geriatric: The pharmacokinetics of LYRINEL were similar in all patients studied (up to 78 years of age).
Race: Available data suggest that there are no significant differences in the pharmacokinetics of oxybutynin based on race in healthy volunteers following administration of LYRINEL.
Renal Insufficiency: There is no experience with the use of LYRINEL in patients with renal insufficiency.
Hepatic Insufficiency: There is no experience with the use of LYRINEL in patients with hepatic insufficiency.
5.3. Preclinical Safety Data A 24-month study in rats at dosages of oxybutynin chloride of 20, 80 and 160 mg/kg/day showed no evidence of carcinogenicity. These doses are approximately 6, 25 and 50 times the maximum human exposure, based on surface area.
Oxybutynin chloride showed no mutagenic activity when tested in Schizosaccharomyces pompholiciformis, Saccharomyces cerevisiae, and Salmonella typhimurium test systems.
Reproduction studies with oxybutynin chloride in the mouse, rat, hamster, and rabbit showed no evidence of impaired fertility.
6. PHARMACEUTICAL PARTICULARS 6.1. List of Excipients LYRINEL also contains the following inert ingredients: cellulose acetate, hypromellose, , magnesium stearate, polyethylene glycol, polyethylene oxide 200K, polyethylene oxide 2000K, Black iron oxide : lactose 95:5
5 mg: iron oxide green:lactose 95:5, opadry YS-1-12871-A light yellow
10 mg: red ferric oxide, opadry pink YS-1-14518-A
6.2. Incompatibilities None known. 6.3. Special Precautions for Storage
Do not store above 25°C . Keep container tightly closed. Keep out of the reach of children.
6.4 Nature and contents of containers
High density polyethylene bottles with child resistant closure (polypropylene) and desiccant. Pack sizes 30 tablets
MARKETING AUTHORISATION HOLDER
J-C Health Care Ltd. Kibbutz Shefayim 60990
Manufacturer
QUALITY, QUANTITY AND INTELLIGIBILITY OF VOWELS IN VIETNAMESE-ACCENTED ENGLISH UNA CUNNINGHAM Introduction This paper attempts to describe and explain some of the phonetic and phonological characteristics of the English spoken by Vietnamese speakers from Hanoi and the particular challenges faced by these speakers in acquiring functional English language skills. Vietnam is in a pro
Note to Parent/Guardians: To comply with State Law governing the administration of medication at school, the Pendleton County School system requires that all students who need medication during school hours do the following: 1. The parent or legal guardian must sign the written consent form for both non-prescription and prescription medication. (The school does not provide non-prescriptio



























 4.7. Effects on Ability to Drive and Use Machines
4.7. Effects on Ability to Drive and Use Machines  In pronounced restlessness or excitation, diazepam may be given by intravenous injection. Tachycardia may be treated with intravenous propranolol and urinary retention managed by bladder catheterisation.
In the event of progression of curare-like effects to paralysis of the respiratory muscles, mechanical ventilation will be required.
The continuous release of oxybutynin from Lyrinel XL should be considered in the treatment of overdose. Patients should be monitored for at least 24 hours.
5. PHARMACOLOGICAL
In pronounced restlessness or excitation, diazepam may be given by intravenous injection. Tachycardia may be treated with intravenous propranolol and urinary retention managed by bladder catheterisation.
In the event of progression of curare-like effects to paralysis of the respiratory muscles, mechanical ventilation will be required.
The continuous release of oxybutynin from Lyrinel XL should be considered in the treatment of overdose. Patients should be monitored for at least 24 hours.
5. PHARMACOLOGICAL 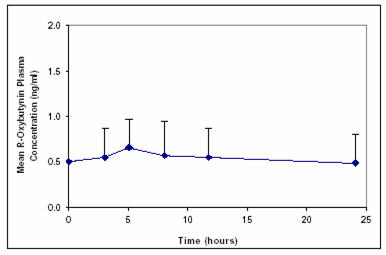 Based on two separate pharmacokinetic studies that evaluated the concomitant use of LYRINEL with an antacid and with a proton pump inhibitor, drugs that increase gastric pH do not affect the release of drug from the tablet or resulting plasma concentrations of oxybutynin and its metabolite, desethyloxybutynin.
Dose Proportionality
Based on two separate pharmacokinetic studies that evaluated the concomitant use of LYRINEL with an antacid and with a proton pump inhibitor, drugs that increase gastric pH do not affect the release of drug from the tablet or resulting plasma concentrations of oxybutynin and its metabolite, desethyloxybutynin.
Dose Proportionality