Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Pnas201118355 1.5
Chronic stress, glucocorticoid receptor resistance,inflammation, and disease riskSheldon Cohena,1, Denise Janicki-Devertsa, William J. Doyleb, Gregory E. Millerc, Ellen Frankd, Bruce S. Rabine,and Ronald B. Turnerf
aDepartment of Psychology, Carnegie Mellon University, Pittsburgh, PA 15213; bDepartment of Otolaryngology/ENT, Children’s Hospital of Pittsburgh,Pittsburgh, PA 15224; cDepartment of Psychology, University of British Columbia, Vancouver, BC, Canada V6T 1Z4; Departments of dPsychiatry and
ePathology, University of Pittsburgh School of Medicine, Pittsburgh, PA 15213; and fDepartment of Pediatrics, University of Virginia Health SciencesCenter, Charlottesville, VA 22908
Edited* by Bruce S. McEwen, The Rockefeller University, New York, NY, and approved February 27, 2012 (received for review November 7, 2011)
We propose a model wherein chronic stress results in glucocorticoid
of chronic inflammatory diseases such as CVD, and type II di-
receptor resistance (GCR) that, in turn, results in failure to down-
regulate inflammatory response. Here we test the model in two
In the common cold, the typical signs and symptoms of illness
viral-challenge studies. In study 1, we assessed stressful life events,
are primarily caused by the release of the proinflammatory cyto-
GCR, and control variables including baseline antibody to the chal-
kines produced in response to infection (13). A series of studies
lenge virus, age, body mass index (BMI), season, race, sex, educa-
have shown that chronic stress is associated with increased sus-
tion, and virus type in 276 healthy adult volunteers. The volunteers
ceptibility to developing a common cold among persons experi-
were subsequently quarantined, exposed to one of two rhinovi-
mentally exposed to an upper respiratory virus (e.g., refs. 14–17).
ruses, and followed for 5 d with nasal washes for viral isolation
This association has been replicated in cross-sectional and pro-
and assessment of signs/symptoms of a common cold. In study 2,
spective studies conducted in natural settings (18). Although
we assessed the same control variables and GCR in 79 subjects who
attempts to identify behavioral pathways linking stress to cold
were subsequently exposed to a rhinovirus and monitored at base-
susceptibility have not been especially successful (14, 15), there is
line and for 5 d after viral challenge for the production of local (in
evidence consistent with stress effects resulting in increased dis-
nasal secretions) proinflammatory cytokines (IL-1β, TNF-α, and IL-6).
ease risk because of their association with exaggerated local (in
Study 1: After covarying the control variables, those with recent
the nose) release of inflammatory cytokines (16). The explanation
exposure to a long-term threatening stressful experience demon-
for this association has been that stress disrupts the HPA response
strated GCR; and those with GCR were at higher risk of subsequently
and that the regulation of inflammation is under HPA control.
developing a cold. Study 2: With the same controls used in study 1,
However, cortisol levels based on 24-h urine (15) and waking di-
greater GCR predicted the production of more local proinflamma-
urnal assessments in saliva (19, 20) do not play a part in this
tory cytokines among infected subjects. These data provide support
process. Alternatively, what matters may be how the target tissue
for a model suggesting that prolonged stressors result in GCR,
responds to cortisol, rather than the levels of the hormone per se.
which, in turn, interferes with appropriate regulation of inflamma-
To the extent that chronic stress results in GCR, one might expect
tion. Because inflammation plays an important role in the onset and
insufficient control over the inflammatory response to the in-
progression of a wide range of diseases, this model may have broad
fection, and consequently a greater expression of the signs and
implications for understanding the role of stress in health.
The viral-challenge paradigm provides an ideal context to study
lymphocytes | receptor sensitivity | psychological stress | cortisol |
the general model of stress leading to disease via effects on the
hypothalamic–pituitary–adrenocortical axis
HPA and inflammatory regulation. In these studies, stress andGCR are assessed before subjects are exposed to a virus and fol-
Chronic psychological stress is associated with a greater risk of lowed in quarantine to determine whether they develop a clinical
depression, cardiovascular disease (CVD), diabetes, autoim-
illness (infection plus signs of illness). Here we conduct secondary
mune diseases, upper respiratory infections (URIs), and poorer
analyses of two independent studies (15, 21), each using a different
wound healing (1). Although these associations are often attrib-
means of assessing GCR, to address the potential role of target
uted to stress-induced dysregulation of the hypothalamic–pitui-
tissue sensitivity to cortisol in linking stress to disease. In study 1,
tary–adrenocortical axis (HPA) (e.g., refs. 2, 3), few human studies
we attempt to replicate earlier evidence that stress exposure is
include assessments of stressful events, HPA response, and a dis-
associated with increased GCR (5, 6, 9–11) and test whether GCR
ease outcome in the same subjects. The lack of such studies is partly
prospectively predicts who will develop a cold when exposed to
attributable to the as yet incomplete understanding of the effects of
a rhinovirus. In study 2, we address whether GCR is prospectively
prolonged stress on the HPA in human subjects (4) and on de-
associated with the magnitude of the local inflammatory cytokine
termining which stress-induced changes in HPA play a downstream
response to being infected by a cold virus. We predict that GCR
role in disease risk. The simple notion that chronic stress acts
will be associated with experiencing a long-term threateningstressful experience, will interfere with the down-regulation of
through the direct effects of elevated circulating cortisol is be-
proinflammatory cytokine response, and will increase illness ex-
coming less likely (5, 6). What may matter more is how target tis-
pression among persons infected with a cold virus.
sues respond to cortisol, rather than levels of the hormone per se.
GCR refers to a decrease in the sensitivity of immune cells to
glucocorticoid hormones that normally terminate the inflammatory
Author contributions: S.C., W.J.D., and G.E.M. designed research; S.C., W.J.D., E.F., B.S.R.,
response (6–9). Evidence for GCR in response to chronic stress
and R.B.T. performed research; E.F. and R.B.T. contributed new reagents/analytic tools;
has been found in parents of children with cancer (10), spouses of
S.C. and D.J.-D. analyzed data; and S.C., D.J.-D., W.J.D., G.E.M., E.F., B.S.R., and R.B.T.
brain-cancer patients (11) and in persons reporting high levels of
loneliness (5). Without sufficient glucocorticoid regulation, the
The authors declare no conflict of interest.
duration and/or intensity of the inflammatory response increases,
*This Direct Submission article had a prearranged editor.
heightening risk for acute exacerbations such as occur in asthma
Freely available online through the PNAS open access option.
and autoimmune diseases, as well as for the onset and progression
1To whom correspondence should be addressed. E-mail:
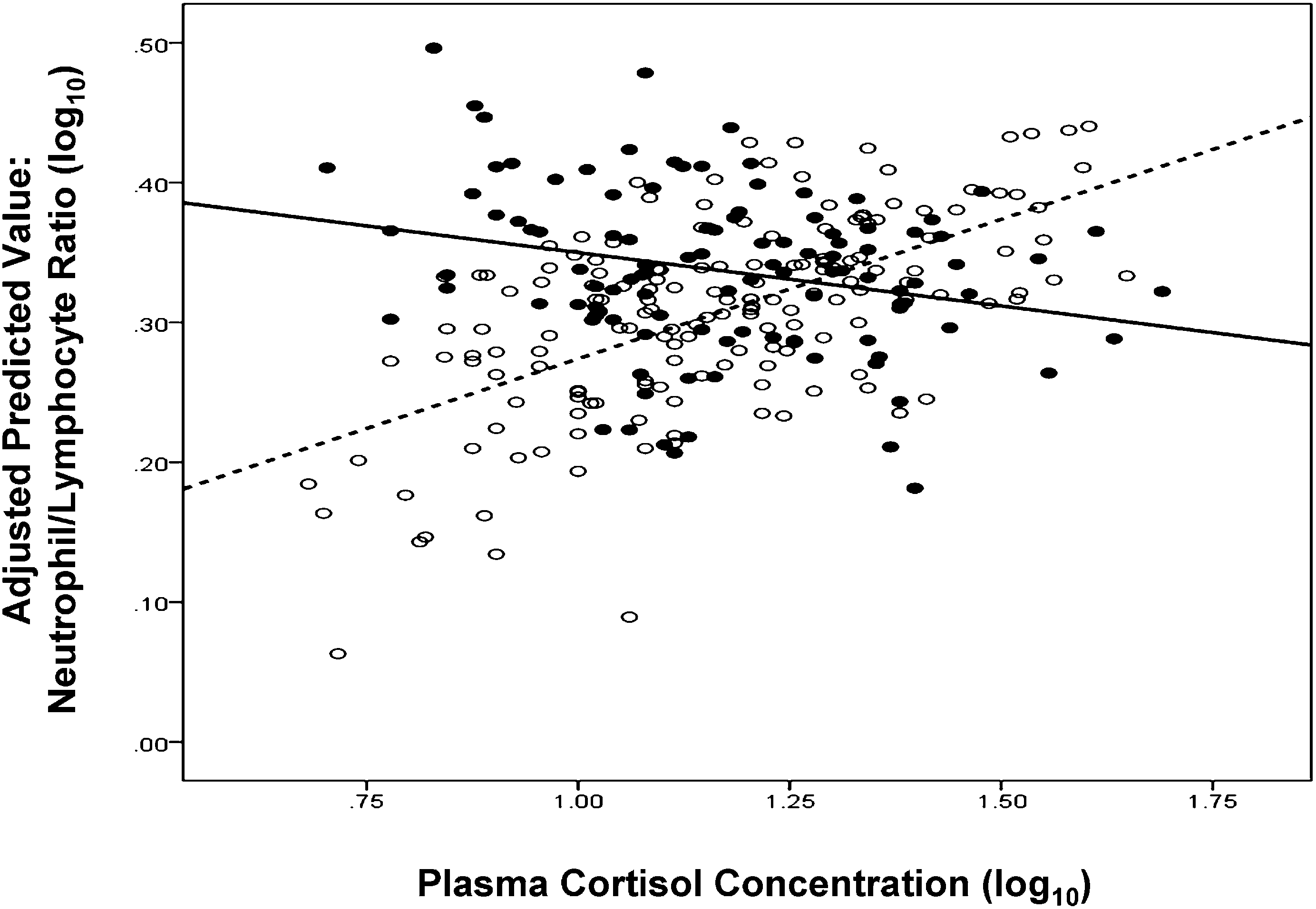
GCR and colds. Similarly we find the expected associations between
All analyses include seven covariates: prechallenge viral-specific
cortisol and leukocyte counts for persons who did not develop
antibody titers, age, body mass index [BMI: weight (kg)/height
a cold following viral challenge (n = 167). In contrast, and con-
(m)2], season (spring or fall), race (white or not), sex, and edu-
sistent with GCR putting people at greater risk for illness, there
cation (study 1: less than high school, high school graduate, some
were no associations between cortisol and leukocyte counts
college, bachelor’s degree or greater; study 2: years of educa-
among those who did develop a cold (n = 109). (Fig. 2, N/L ratio.)
tion). In study 1, where subjects receive one of two viruses,
Here linear regressions indicate stress-by-cortisol interactions for
analyses also control for virus type [rhinovirus (RV)21 or RV39].
lymphocytes (P = 0.02), neutrophils (marginal at P = 0.08), andN/L ratio (P = 0.02). For all three analyses, simple slopes among
Study 1. Stress and colds. As reported in similar analyses of these
those who did not develop a cold were significantly different from
data (14), in a multiple logistic regression, exposure to a recent
0, whereas slopes for those who did develop a cold were not
major stressful life event was associated with an increased risk
(Table 2). As expected, plasma cortisol levels did not predict who
for developing a cold following exposure to RV (OR = 1.99,
developed a cold (OR = 1.27, CI = 0.20, 7.94). Together, results
CI = 1.04, 3.08). This association was similar across the two
from these prospective analyses support the hypothesis that GCR
viruses (P > 0.16 for stress-by-virus interaction).
predicts an increased risk for colds following viral exposure,
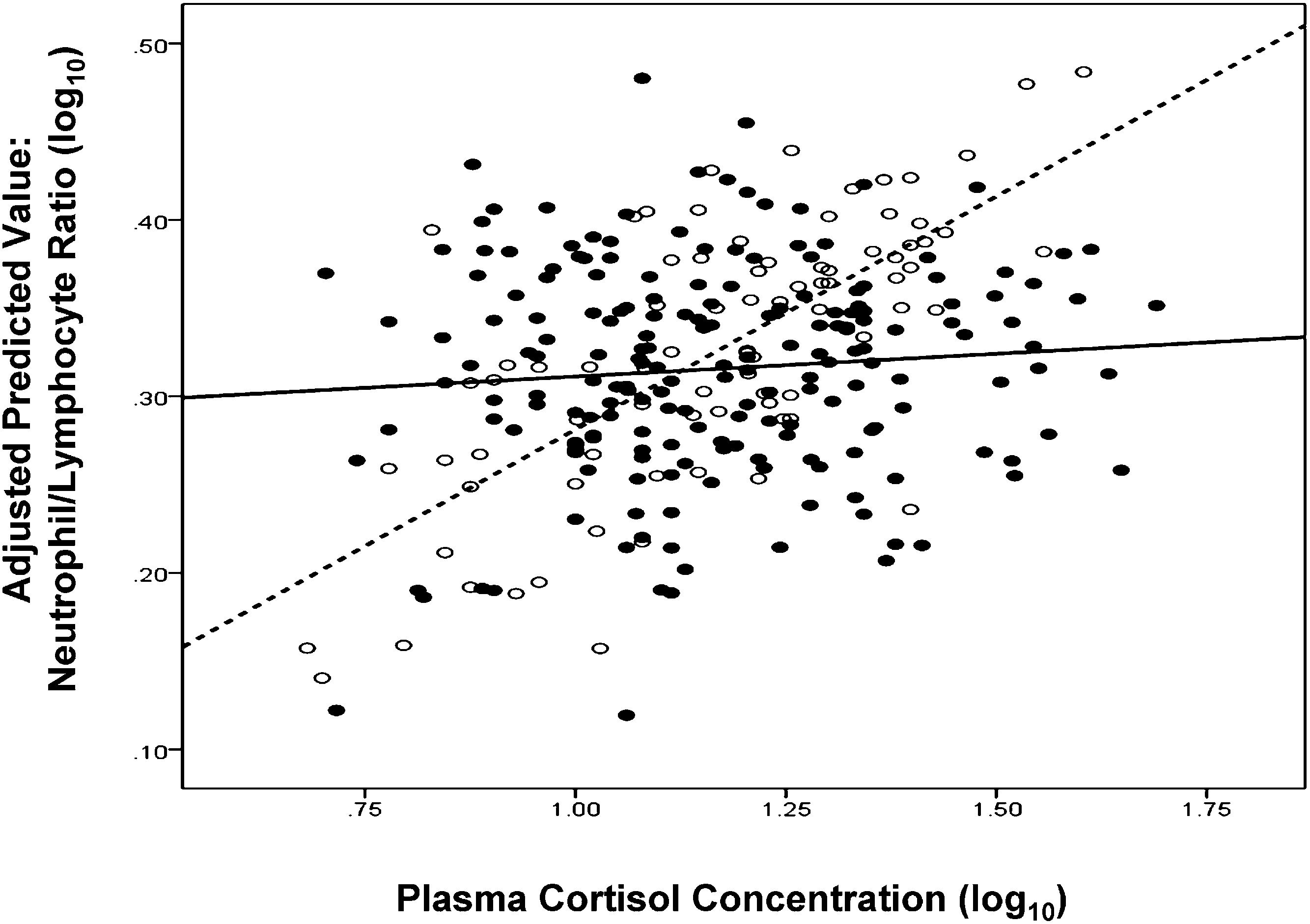
Stress, GCR, and colds. Greater levels of glucocorticoid are associated
whereas levels of circulating cortisol do not.
with higher numbers of circulating neutrophils, lower numbers
Consideration of alternative explanations. To evaluate the possibility
of circulating lymphocytes, and a lower neutrophil-to-lymphocyte
that sympathetic nervous system hormones that often increase
(N/L) ratio—an overall marker of the trafficking of these cells (e.g.,
with cortisol may be driving the redistribution of cells, we con-
refs. 22, 23). Cole and his colleagues (5, 24) showed that this as-
ducted all of the same analyses described earlier replacing cor-
sociation can be used to indirectly assess GCR. The logic of the
tisol with epinephrine (E) and with norepinephrine (NE). These
measure is that there is a strong physiologic correlation between
hormones were not associated with numbers of any of the cell
cortisol levels and the number of circulating leukocytes only if
types in relevant subgroups of subjects defined by either stress
leukocyte glucocorticoid receptors are sensitive (i.e., signaling cells
to redistribute). Stress and GCR. We found the expected associations between
Study 2. GCR and nasal cytokines. We suggest that the association of
leukocyte numbers and cortisol among those who did not expe-
GCR with colds reflects inadequate control of local inflammatory
rience a major stressor (n = 83). In contrast, consistent with the
responses to the virus. To test this hypothesis, we examine
hypothesis that stress results in GCR, there were no associations
whether GCR predicts the production of local proinflammatory
between cortisol and leukocytes among those who did experience
cytokines when subjects are exposed to a rhinovirus. Data for this
a stressor (n = 193). Fig. 1 displays these findings graphically
study were collected from a subsample of subjects in a larger viral-
using the relation of cortisol to N/L ratio as an example. That the
challenge trial (15). Here GCR was assessed before viral chal-
slopes of the stressed and nonstressed subjects were different
lenge using a standard ex vivo model (6), wherein leukocytes were
from each other is supported by stress-by-cortisol level inter-
coincubated with lipopolysaccharide and dexamethasone, and
actions found in linear regressions predicting lymphocytes (P =
proinflammatory cytokine production measured in supernatants.
0.03), neutrophils (P = 0.03) and the N/L ratio (P = 0.03). For
The logic behind this assay is that dexamethasone should inhibit
all three analyses, simple slopes for those without stress were
cytokine production only to the extent that leukocytes are sensi-
significantly different from 0, whereas slopes for those with stress
tive to its effects. This study had enough subjects with the required
were not (Table 1). These analyses support GCR emergence
data to examine cytokine response (a continuous variable) but not
among those experiencing major stressors.
Association between plasma cortisol and the ratio of neutrophils to lymphocytes for subjects experiencing and not experiencing a significant stressful
life event during the last year. Lack of correlation is a marker of GCR. Filled circles/solid line, major stressful life event; open circles/dashed line, no stressful event.
Simple effect associations of stress status with
developing a cold following exposure to a rhinovirus (also reported
in ref. 15). New analyses indicate that this same stress measurewas also associated with GCR, with stressed persons showing less
sensitivity of lymphocyte and neutrophil counts to distributional
changes associated with greater circulating levels of cortisol. In
turn, GCR was prospectively associated with increased risk of
developing a common cold following experimental inoculation
with a cold virus. These data are consistent with a model whereinstress leads to GCR, which in turn results in greater risk for de-
Analyses control for age, sex, race, body mass index, education, prechal-
veloping a cold. In study 2, GCR predicted how much local
fic antibody titers, season, and virus type. **P < 0.01.
proinflammatory cytokine was produced in response to infection. Because the analyses in both studies were prospective, we can
Table 3 presents the partial correlations between GCR and
eliminate reverse causation (colds did not cause stress, colds did
proinflammatory cytokine levels in the nasal cavity during the 5 d
not cause GCR, and cytokine release did not cause GCR) as an
following viral challenge. For both IL-6 and TNF-α, increases in
alternative explanation. The use of multiple control variables also
the resistance curve were associated with increased production of
eliminates many potential spurious explanations.
the matching local inflammatory cytokine. Greater IL-1β GCR
The GCR measure used in study 1 is indirect. However, exper-
was also associated with greater local IL-6 production. The cor-
imental studies have shown that glucocorticoid-induced leukocyte
relation of IL-1β GCR with local IL-1β release was in the expected
redistribution is specifically attributable to glucocorticoid receptor
direction, but was not significant. All of these results are the same
signaling (25), and that the indirect assessment used here corre-
whether the analyses include all subjects, or are limited to those
lates with blunting of lymphocyte redistribution in response to
infected by the virus. Cortisol levels as assessed by multiple sam-
dexamethasone injection (24). Even so, it is possible that the action
ples of saliva collected across the day before viral challenge were
of another hormone or mechanism both highly correlated with
unrelated to any of the three GCR measures (all P > 0.20) or to
cortisol and having the same impact on leukocyte trafficking as
proinflammatory cytokine levels (all P > 0.40). Overall, these data
cortisol could account for these effects. Likely alternative explan-
are consistent with the hypothesis that a decreased sensitivity of
ations include that the associations are attributable to subject
leukocytes to the inhibitory effects of cortisol (increased GCR)
health (e.g., infections) or to receptor sensitivity to E and/or NE.
reflects a decreased ability of cortisol to regulate the production of
Health is not an issue here, because subjects are carefully
local proinflammatory cytokines in response to infection.
screened for excellent health. Further, we found that neither Enor NE were correlated with leukocyte counts under any of the
relevant conditions (similar results in ref. 5). We also found
We proposed that exposure to a major stressful life event can result
consistent evidence across studies 1 and 2, even though study 2
in GCR, which, in turn, would interfere with HPA down-regulation
used a standard direct assessment of GCR.
of local proinflammatory cytokine response to an infectious agent.
We found no effects of cortisol levels on disease risk (e.g., refs.
Without appropriate cortisol regulation of the local cytokine re-
19, 20), GCR, or inflammation. This apparent lack of a role for
sponse, there would be an exaggerated expression of the signs of
circulating cortisol levels is consistent with the possibility that
URI, which are generated by the proinflammatory response. In
impaired target tissue response to the regulatory effects of this
study 1, stress—defined as a recent stressful life experience asso-
hormone may overshadow any modulatory influences that might
ciated with long-term threat—predicted an increased risk of
result from changes in circulating concentrations of cortisol itself.
Association between plasma cortisol and the ratio of neutrophils to lymphocytes for subjects who developed and did not develop a cold after exposure
to a rhinovirus. Lack of correlation is a marker of GCR. Filled circles/solid line, meets cold criterion; open circles/dashed line, does not meet cold criterion.
Simple effect associations of cold status with
Study 1. Subjects and design. The subjects were 125 men and 151 women, meanage 29.13 y (SD = 9.09 y) who responded to newspaper advertisements and
were judged to be in good health after a medical examination. Subjects
were paid $800 for their participation.
After we assessed life stress, complete blood counts, cortisol, demographics,
anthropomorphics, and virus-specific antibody levels, subjects were quaran-
tined in separate rooms, exposed to one of two RVs and followed for 5 d with
nasal washes for viral isolation and assessment of symptoms and signs of a
Analyses control for age, sex, race, body mass index, education, prechallenge
Experimental plan. At the medical screening, age, education, race, sex, body
fic antibody titers, season, and virus type. *P < 0.05, **P < 0.01.
weight, and height were also assessed and used as baseline data for thosedeemed eligible. Eligible subjects returned to the hospital 4 and 5 wk later
In the case of the common cold, a disease for which expression
(1–2 wk before viral challenge) for two blood samples for determination of
of the signs/symptoms of illness is driven by the inflammatory
complete blood counts, antibody to the challenge virus, and plasma cortisoland for the stressful life event interview.
response, the failure of the HPA to regulate the production of
After completing the baseline assessments, subjects entered quarantine.
local proinflammatory cytokines contributes to the risk for clinical
During the first 24 h of quarantine (before viral challenge), they had a nasal
illness. Because inflammation plays a role in progression of mul-
examination (including a nasal wash culture for RV) and were excluded if there
tiple diseases, this model not only provides an explanation for the
was any indication of recent or current URI or illness. An update stressful life
increased risk for URI under stress, but might provide a more
event interview was administered at this time to identify events occurring
general explanation for why prolonged stress would play a role in
between the initial interview and quarantine. Baseline respiratory signs (nasalmucociliary clearance and nasal mucus production) and symptoms were
other inflammatory diseases as well. Moreover, although the focus
assessed. At the end of the first 24 h of quarantine, subjects were given nasal
here has been on GCR in circulating leukocytes and neutrophils,
drops containing a low infectious dose of either RV21 (N = 129) or RV39 (N =
stress could also be associated with illness expression through its
147). Quarantine continued for 5 d after challenge. Nasal secretion samples
effect on the glucocorticoid sensitivity of other cells involved in
for virus culture were collected on each of the 5 d. Subjects were also tested
immune defenses (26). For example, glucocorticoid receptors (GR)
on each day for respiratory symptoms, nasal mucociliary clearance, and nasal
are expressed by cells involved with antigen presentation, such as
mucus production. Approximately 28 d postchallenge, a blood sample wascollected for assaying convalescent antibodies to the challenge virus. All
dendrocytes and macrophages, not only in circulation but also at
investigators were blinded to subjects’ status on all baseline assessments.
specific sites of infection and in draining lymph nodes.
Stressful life events. Life events were assessed by a standardized semistructured
Parodoxically, proinflammatory cytokines are thought to both
interview, the Bedford College Life Events and Difficulties Schedule (LEDS)
up-regulate immunity to the virus and produce cold symptoms
(29), and conducted by trained interviewers. We considered only those events
(13). However, here stress and GCR, conditions associated with
that occurred during the last 12 mo. Ratings of events were performed in an
increased levels of local proinflammatory cytokine, predicted a
independent laboratory by consensus groups consisting of at least fourtrained interviewers. The interview staff was blind to other study measures.
greater risk of clinical illness. These data are consistent with
Raters were also blind to individuals’ subjective responses to the stressful
those of other viral-challenge studies that found a positive as-
events and used “dictionaries” of precedent examples to rate each stressful
sociation between proinflammatory cytokine levels and symptom
experience reported during the interview on long-term threat (i.e., threat
that is sustained beyond the immediate experience of the event). Dictionary
An unexplained inconsistency in the data from study 2 is that
ratings are based on the likely response of an average person to a stressor
local IL-6 and TNF-α, but not IL-1β, were correlated with GCR
occurring in the context of the subject’s particular set of biographical cir-
measured by the whole blood ex vivo assay. It is possible that this
cumstances. It is the long-term threat of an experience that is thought todetermine its implications for health. Here, we define stress as a life experi-
discrepancy is due to the relative insensitivity of the IL-1β assay.
ence, irrespective of duration (including both acute events and chronic dif-
Alternatively, it may reflect a differential sensitivity of these
ficulties in LEDS parlance), that was rated as having high moderate or marked
cytokines to glucocorticoid suppression (27).
long-term threat. We excluded stress resulting from physical illness to avoid
Finally, future research on GCR would benefit from quanti-
confounding a chronic health condition with susceptibility and stressful
fication of GR subtypes, whose relative abundance might un-
events in which the subject was not a major focus.
derlie the findings observed here. Chronic stress does not appear
GCR. We conducted a complete blood count and assayed for cortisol in each oftwo blood samples collected 1 and 2 wk prechallenge. Correlations between cell
to affect expression of GRα, the active isoform of the receptor
counts from the two blood draws ranged from 0.61 to 0.76, P < 0.001. Plasma
(11). However, there is evidence linking stress and cytokines to
cortisol was measured using a double-antibody competitive RIA. The correla-
higher levels of GRβ and a lower GRα/GRβ ratio (28). This
tion between cortisol in the two samples was 0.70, P < 0.001. Because we were
could prove important because GRβ is a dominant negative re-
concerned with stable differences in cortisol and in cell distributions that occur
ceptor for cortisol, which can suppress GRα activity and thereby
in response to prolonged stress, we averaged the two values in both cases.
We found no associations between monocyte percentage and cortisol in the
entire sample or in sample subsets split by stress or colds. Thus, we could not usewhether cortisol was associated with monocytes as a marker of GCR. Our dataare therefore based on the associations of cortisol with percentages of lym-
Partial correlations of glucocorticoid resistance curves
phocytes and neutrophils. We also use the ratio of neutrophils to lymphocytes
(AUC) with nasal cytokine AUCs: Entire sample and infected subset
(log10) as an overall marker of the trafficking of these cells (5, 24). Epinephrine and Norepinephrine. Urine was obtained from 24-h collections that
began on day 0 of quarantine. E and NE were measured using high per-
formance liquid chromatography with electrochemical detection. Values areexpressed in micrograms per milligram of creatinine (log10).
Infection. Nasal washes were performed daily during quarantine to provide
samples of nasal secretions for virus culture (30). Neutralizing antibodies to
the challenge virus were tested in prechallenge and 28-d postchallenge se-rum samples (30).
Signs of illness. On each day of quarantine, we collected two objective signs of
disease—mucus weights and mucociliary clearance function. Mucus weights
Analyses control for age, sex, race, years of education, body mass index,
were determined by collecting used tissues in sealed plastic bags (31). The
prechallenge antibody, and season. *P < 0.10, **P < 0.05, ***P < 0.01.
bags were weighed and the weight of the tissues and bags subtracted. To
adjust for baseline, mucus weight on the day before challenge (mode = 0)
maximized the rate of infection by including only subjects with prechallenge
was subtracted from each daily mucus weight after challenge. Adjusted
viral-specific antibody titers ≤4.
weights with negative values were scored as 0. The adjusted postchallenge
During the first 24 h of quarantine (before viral challenge) nasal muco-
weights were summed to create an adjusted total mucus weight.
ciliary clearance and nasal mucus production were assessed. Volunteers were
Nasal mucociliary clearance function refers to the effectiveness of nasal cilia
excluded if they had signs or symptoms of a cold and excluded from analysis if
in clearing mucus from the nasal passage toward the nasopharnyx. Clearance
a viral pathogen was isolated from the nasal lavage obtained at that time.
function was assessed as the time required for a dye administered into the nose
Subjects were then given nasal drops containing an infectious dose of
to reach the nasopharnyx (31). Each daily time was adjusted (by subtracting)
RV39. On each day of quarantine nasal lavage samples were collected for
for baseline (negative values were scored as 0) and the adjusted average time
virus culture and assessment of local proinflammatory cytokines. Approxi-
in minutes was calculated across the postchallenge days of the trial.
mately 28 d postchallenge, blood was collected for serological testing. The
Clinical illness. Subjects were considered to have a cold if they were both
investigators were blinded to all baseline measures.
infected and met objective illness criteria. They were classified as infected if the
Infection. Infection was assessed with the same procedures used in study 1.
challenge virus was isolated on any of the 5 postchallenge study days or if there
GCR. We used a standard in vitro assay to measure GCR that assessed the
was a fourfold or greater rise in virus-specific serum neutralizing antibody titer
ability of dexamethasone (0, 10, 50, and 250 nM) to suppress lipopolysac-
between prechallenge and 28-d postchallenge. Illness criterion was based on
charide (30 ng/mL) stimulated lymphocyte production of IL-1β, IL-6, and TNF-
objective indicators of illness—a total adjusted mucus weight of ≥10 g or an
α. The remaining procedures were the same as those used in Miller et al. (6).
adjusted average mucociliary nasal clearance time of ≥7 min (21).
Area under the dexamethasone curve (adjusted for an unstimulated control)
Statistical analyses. We conducted two sets of regression analyses, each pre-
dicting the percentage of neutrophils, lymphocytes, and the N/L ratio. The
Proinflammatory cytokines. We measured IL-1β, IL-6, and TNF-α in nasal secre-
first set included the standard covariates, a dichotomous variable repre-
tions. Nasal wash fluid was assayed for cytokine protein using the BioSource
senting life stress (1 = stress, 0 = no stress), continuous plasma cortisol, and the
Ten-plex bead immunoassay and methods provided by the manufacturer
interaction of life stress and cortisol. We predicted an interaction with leu-
(BioSource International). Assays were performed in duplicate using a Luminex
kocyte counts increasing (neutrophils and N/L ratio) or decreasing (lym-
100 bead-based immunoassay system. To control for basal nasal cytokine
phocytes) with increasing cortisol levels for those without a major stressful life
levels, prechallenge cytokine values were subtracted from the values obtained
event but not for those with an event. The second set included standard
on each of the 5 postchallenge days. Nasal cytokine area under the curve (AUC)
covariates, dichotomous variables for life stress, and cold status (1 = cold, 0 =
was derived from these baseline-adjusted values and computed using the
no cold) and the interaction of life stress and cold status. We again predicted
an interaction with cortisol associated with leukocyte counts among those
Cortisol. Subjects provided seven saliva samples (collected at wake-up and at 1,
without colds but not among those with colds. We also calculated the simple
2, 4, 7, 9, and 14 h after wake-up) on the day preceding viral challenge by
slopes for each group in all analyses and tested whether they were signifi-
chewing on cotton rolls until saturated and then storing the rolls in plastic
salivettes. Code numbers provided by hand-held computers were used to
guarantee timely collection of samples. Saliva cortisol level was determined
Study 2. Subjects and design. The subjects were 39 men and 43 women (mean
age = 36.9 y, SD = 9.2 y) who responded to advertisements and were judged to
10 AUC adjusted for wake-up time was used to represent
be in good health. They were paid $800 for their participation. Three subjectswere excluded due to incomplete nasal cytokine data.
After we assessed GCR and the standard control variables, subjects were
ACKNOWLEDGMENTS. Preparation of this paper was supported by GrantAT006694 from the National Center for Complementary and Alternative
quarantined in separate rooms, exposed to a rhinovirus and followed for 5 d with
Medicine; conducting the studies, by Grants MH47234 and MH50430 from
nasal washes to assess viral shedding and local proinflammatory cytokines.
the National Institute of Mental Health and Grants HL65111 and HL65112
Experimental plan. At the medical screening we also collected specific serum
from the National Heart, Lung, and Blood Institute; and the assay of
antibody titer to the challenge virus, demographics, weight, and height.
glucocorticoid resistance in study 2, by the MacArthur Foundation Research
Because we were interested in inflammatory response to infection, we
Network on Socioeconomic Status and Health.
1. Cohen S, Janicki-Deverts D, Miller GE (2007) Psychological stress and disease. JAMA
18. Pedersen A, Zachariae R, Bovbjerg DH (2010) Influence of psychological stress on
upper respiratory infection—a meta-analysis of prospective studies. Psychosom Med
2. McEwen BS (1998) Protective and damaging effects of stress mediators. N Engl J Med
19. Cohen S, et al. (2008) Objective and subjective socioeconomic status and susceptibility
3. McEwen BS, Seeman T (1999) Protective and damaging effects of mediators of stress.
to the common cold. Health Psychol 27:268–274.
Elaborating and testing the concepts of allostasis and allostatic load. Ann N Y Acad Sci
20. Edwards S, Hucklebridge F, Clow A, Evans P (2003) Components of the diurnal cortisol
cycle in relation to upper respiratory symptoms and perceived stress. Psychosom Med
4. Miller GE, Chen E, Zhou ES (2007) If it goes up, must it come down? Chronic stress and
the hypothalamic-pituitary-adrenocortical axis in humans. Psychol Bull 133:25–45.
21. Cohen S, Doyle WJ, Skoner DP, Rabin BS, Gwaltney JM, Jr. (1997) Social ties and
5. Cole SW (2008) Social regulation of leukocyte homeostasis: The role of glucocorticoid
susceptibility to the common cold. JAMA 277:1940–1944.
sensitivity. Brain Behav Immun 22:1049–1055.
22. Fauci AS, Dale DC, Balow JE (1976) Glucocorticosteroid therapy: Mechanisms of action
6. Meagher MW, Johnson RR, Good E, Welsh TH (2006) Psychoneuroimmunology, eds
and clinical considerations. Ann Intern Med 84:304–315.
Ader R, Felton D, Cohen N (Academic, New York), 4th Ed, Vol II, pp 1107–1124.
23. Dhabhar FS, Miller AH, McEwen BS, Spencer RL (1996) Stress-induced changes in blood
7. Marques AH, Silverman MN, Sternberg EM (2009) Glucocorticoid dysregulations and
leukocyte distribution. Role of adrenal steroid hormones. J Immunol 157:1638–1644.
their clinical correlates. From receptors to therapeutics. Ann N Y Acad Sci 1179:1–18.
24. Cole SW, Mendoza SP, Capitanio JP (2009) Social stress desensitizes lymphocytes to
8. Bailey M, Engler H, Hunzeker J, Sheridan JF (2003) The hypothalamic-pituitary-adre-
regulation by endogenous glucocorticoids: Insights from in vivo cell trafficking dy-
nal axis and viral infection. Viral Immunol 16:141–157.
namics in rhesus macaques. Psychosom Med 71:591–597.
9. Stark JL, et al. (2001) Social stress induces glucocorticoid resistance in macrophages.
25. Miller AH, et al. (1994) Effects of selective type I and II adrenal steroid agonists on
immune cell distribution. Endocrinology 135:1934–1944.
10. Miller GE, Cohen S, Ritchey AK (2002) Chronic psychological stress and the regulation
26. Webster JI, Tonelli L, Sternberg EM (2002) Neuroendocrine regulation of immunity.
of pro-inflammatory cytokines: A glucocorticoid-resistance model. Health Psychol 21:
27. DeRijk R, et al. (1997) Exercise and circadian rhythm-induced variations in plasma
11. Miller GE, et al. (2008) A functional genomic fingerprint of chronic stress in humans:
cortisol differentially regulate interleukin-1 β (IL-1 β), IL-6, and tumor necrosis factor-α
Blunted glucocorticoid and increased NF-kappaB signaling. Biol Psychiatry 64:266–272.
(TNF α) production in humans: High sensitivity of TNF α and resistance of IL-6. J Clin
12. Nathan C (2002) Points of control in inflammation. Nature 420:846–852.
13. Hendley JO (1998) The host response, not the virus, causes the symptoms of the
28. Derijk RH, et al. (2001) A human glucocorticoid receptor gene variant that increases
common cold. Clin Infect Dis 26:847–848.
the stability of the glucocorticoid receptor beta-isoform mRNA is associated with
14. Cohen S, Tyrrell DAJ, Smith AP (1991) Psychological stress and susceptibility to the
rheumatoid arthritis. J Rheumatol 28:2383–2388.
common cold. N Engl J Med 325:606–612.
29. Brown GW, Harris TO (1989) Life Events and Illness (Guilford, New York).
15. Cohen S, et al. (1998) Types of stressors that increase susceptibility to the common
30. Gwaltney JM, Jr., Colonno RJ, Hamparian VV, Turner RB (1989) Diagnostic Procedures
cold in healthy adults. Health Psychol 17:214–223.
for Viral, Rickettsial and Chlamydial Infections, eds Schmidt NJ, Emmons RW (Amer-
16. Cohen S, Doyle WJ, Skoner DP (1999) Psychological stress, cytokine production, and
ican Public Health Association, Washington, DC), 6th Ed, pp 579–614.
severity of upper respiratory illness. Psychosom Med 61:175–180.
31. Doyle WJ, McBride TP, Swarts JD, Hayden FG, Gwaltney JM, Jr. (1988) The response of
17. Stone AA, et al. (1992) Development of common cold symptoms following experimental
the nasal airway, middle ear, and Eustachian tube to provocative rhinovirus chal-
rhinovirus infection is related to prior stressful life events. Behav Med 18:115–120.
DESERT DE DANAKIL ET ERTA ALE Ethiopie - B972 Ce voyage aurait pu s'intituler à la naissance du monde ou rendez-vous avec les entrailles de la Terre. Au cœur du désert du Danakil, l'un des plus chauds de la planète, se trouvent deux des plus impressionantes représentations de la vie volcanique de notre planète. Tout d'abord le volcan Erta Ale et son lac de magma de plus de 3000
KENMERKENBLAD Sigma Renova Isotop Matt OMSCHRIJVING Watergedragen, geurarme, isolerende muurverf voor binnen op basis van speciale acrylaatdispersies. GEBRUIKSDOEL In combinatie met Sigma Renova Isotop Primer te gebruiken voor het isoleren van ondergronden die middelzwaar tot zwaar vervuild zijn met doorslaggevoelige verontreinigingen (nicotine-, rook- en roetaanslag, wate
 Chronic stress, glucocorticoid receptor resistance,inflammation, and disease riskSheldon Cohena,1, Denise Janicki-Devertsa, William J. Doyleb, Gregory E. Millerc, Ellen Frankd, Bruce S. Rabine,and Ronald B. Turnerf
aDepartment of Psychology, Carnegie Mellon University, Pittsburgh, PA 15213; bDepartment of Otolaryngology/ENT, Children’s Hospital of Pittsburgh,Pittsburgh, PA 15224; cDepartment of Psychology, University of British Columbia, Vancouver, BC, Canada V6T 1Z4; Departments of dPsychiatry and
ePathology, University of Pittsburgh School of Medicine, Pittsburgh, PA 15213; and fDepartment of Pediatrics, University of Virginia Health SciencesCenter, Charlottesville, VA 22908
Edited* by Bruce S. McEwen, The Rockefeller University, New York, NY, and approved February 27, 2012 (received for review November 7, 2011)
We propose a model wherein chronic stress results in glucocorticoid
of chronic inflammatory diseases such as CVD, and type II di-
receptor resistance (GCR) that, in turn, results in failure to down-
regulate inflammatory response. Here we test the model in two
In the common cold, the typical signs and symptoms of illness
viral-challenge studies. In study 1, we assessed stressful life events,
are primarily caused by the release of the proinflammatory cyto-
GCR, and control variables including baseline antibody to the chal-
kines produced in response to infection (13). A series of studies
lenge virus, age, body mass index (BMI), season, race, sex, educa-
have shown that chronic stress is associated with increased sus-
tion, and virus type in 276 healthy adult volunteers. The volunteers
ceptibility to developing a common cold among persons experi-
were subsequently quarantined, exposed to one of two rhinovi-
mentally exposed to an upper respiratory virus (e.g., refs. 14–17).
Chronic stress, glucocorticoid receptor resistance,inflammation, and disease riskSheldon Cohena,1, Denise Janicki-Devertsa, William J. Doyleb, Gregory E. Millerc, Ellen Frankd, Bruce S. Rabine,and Ronald B. Turnerf
aDepartment of Psychology, Carnegie Mellon University, Pittsburgh, PA 15213; bDepartment of Otolaryngology/ENT, Children’s Hospital of Pittsburgh,Pittsburgh, PA 15224; cDepartment of Psychology, University of British Columbia, Vancouver, BC, Canada V6T 1Z4; Departments of dPsychiatry and
ePathology, University of Pittsburgh School of Medicine, Pittsburgh, PA 15213; and fDepartment of Pediatrics, University of Virginia Health SciencesCenter, Charlottesville, VA 22908
Edited* by Bruce S. McEwen, The Rockefeller University, New York, NY, and approved February 27, 2012 (received for review November 7, 2011)
We propose a model wherein chronic stress results in glucocorticoid
of chronic inflammatory diseases such as CVD, and type II di-
receptor resistance (GCR) that, in turn, results in failure to down-
regulate inflammatory response. Here we test the model in two
In the common cold, the typical signs and symptoms of illness
viral-challenge studies. In study 1, we assessed stressful life events,
are primarily caused by the release of the proinflammatory cyto-
GCR, and control variables including baseline antibody to the chal-
kines produced in response to infection (13). A series of studies
lenge virus, age, body mass index (BMI), season, race, sex, educa-
have shown that chronic stress is associated with increased sus-
tion, and virus type in 276 healthy adult volunteers. The volunteers
ceptibility to developing a common cold among persons experi-
were subsequently quarantined, exposed to one of two rhinovi-
mentally exposed to an upper respiratory virus (e.g., refs. 14–17).
 GCR and colds. Similarly we find the expected associations between
All analyses include seven covariates: prechallenge viral-specific
cortisol and leukocyte counts for persons who did not develop
antibody titers, age, body mass index [BMI: weight (kg)/height
a cold following viral challenge (n = 167). In contrast, and con-
(m)2], season (spring or fall), race (white or not), sex, and edu-
sistent with GCR putting people at greater risk for illness, there
cation (study 1: less than high school, high school graduate, some
were no associations between cortisol and leukocyte counts
college, bachelor’s degree or greater; study 2: years of educa-
among those who did develop a cold (n = 109). (Fig. 2, N/L ratio.)
tion). In study 1, where subjects receive one of two viruses,
Here linear regressions indicate stress-by-cortisol interactions for
analyses also control for virus type [rhinovirus (RV)21 or RV39].
GCR and colds. Similarly we find the expected associations between
All analyses include seven covariates: prechallenge viral-specific
cortisol and leukocyte counts for persons who did not develop
antibody titers, age, body mass index [BMI: weight (kg)/height
a cold following viral challenge (n = 167). In contrast, and con-
(m)2], season (spring or fall), race (white or not), sex, and edu-
sistent with GCR putting people at greater risk for illness, there
cation (study 1: less than high school, high school graduate, some
were no associations between cortisol and leukocyte counts
college, bachelor’s degree or greater; study 2: years of educa-
among those who did develop a cold (n = 109). (Fig. 2, N/L ratio.)
tion). In study 1, where subjects receive one of two viruses,
Here linear regressions indicate stress-by-cortisol interactions for
analyses also control for virus type [rhinovirus (RV)21 or RV39].
 Simple effect associations of stress status with
developing a cold following exposure to a rhinovirus (also reported
in ref. 15). New analyses indicate that this same stress measurewas also associated with GCR, with stressed persons showing less
sensitivity of lymphocyte and neutrophil counts to distributional
changes associated with greater circulating levels of cortisol. In
turn, GCR was prospectively associated with increased risk of
developing a common cold following experimental inoculation
with a cold virus. These data are consistent with a model whereinstress leads to GCR, which in turn results in greater risk for de-
Analyses control for age, sex, race, body mass index, education, prechal-
veloping a cold. In study 2, GCR predicted how much local
fic antibody titers, season, and virus type. **P < 0.01.
Simple effect associations of stress status with
developing a cold following exposure to a rhinovirus (also reported
in ref. 15). New analyses indicate that this same stress measurewas also associated with GCR, with stressed persons showing less
sensitivity of lymphocyte and neutrophil counts to distributional
changes associated with greater circulating levels of cortisol. In
turn, GCR was prospectively associated with increased risk of
developing a common cold following experimental inoculation
with a cold virus. These data are consistent with a model whereinstress leads to GCR, which in turn results in greater risk for de-
Analyses control for age, sex, race, body mass index, education, prechal-
veloping a cold. In study 2, GCR predicted how much local
fic antibody titers, season, and virus type. **P < 0.01. Simple effect associations of cold status with
Study 1. Subjects and design. The subjects were 125 men and 151 women, meanage 29.13 y (SD = 9.09 y) who responded to newspaper advertisements and
were judged to be in good health after a medical examination. Subjects
were paid $800 for their participation.
Simple effect associations of cold status with
Study 1. Subjects and design. The subjects were 125 men and 151 women, meanage 29.13 y (SD = 9.09 y) who responded to newspaper advertisements and
were judged to be in good health after a medical examination. Subjects
were paid $800 for their participation. adjust for baseline, mucus weight on the day before challenge (mode = 0)
maximized the rate of infection by including only subjects with prechallenge
was subtracted from each daily mucus weight after challenge. Adjusted
viral-specific antibody titers ≤4.
adjust for baseline, mucus weight on the day before challenge (mode = 0)
maximized the rate of infection by including only subjects with prechallenge
was subtracted from each daily mucus weight after challenge. Adjusted
viral-specific antibody titers ≤4.