Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Ovulatory
OVULATORY DISTURBANCES: THEY DO MATTER from: The Canadian Journal of DIAGNOSIS February 1997
For the woman who isn't trying to get pregnant, does it matter if an ovulatory pattern is normal? Recent studies indicate that it does. One study showed that women with only one nonovulatory cycle a year lost an average of 4% of their spinal bone. Strong evidence suggests that lack of cyclic normal progesterone is detrimental to good health.
Dr. Prior is a professor, Division of Endocrinology, University of British Columbia, Vancouver, B.C and Scientific Director of the Centre for Menstrual Cycle and Ovulation Research.
Women aged 25 to 40 rarely complain about their menstrual cycles. Irregular cycles and problems with flow and cramps are typical of the beginning and end of reproductive life. Women with regular cycles, however, are likely to be experiencing some cycles with disturbed ovulation.
It is also likely that you and your 30-year-old patient have never reviewed her menstrual cycle in detail. If you have, you likely asked whether her cycles were regular. If she answered yes, you assumed all was well. And so did she. When cycles that are ideal in length (averaging 28 days) are explored for progesterone levels and not just estrogen production, a surprising finding emerges. Approximately one-third of regular, asymptomatic menstrual cycles of healthy women will have disturbances of ovulation that, based on biologic principles, could lead to significant health risks.
It is quite common and probably normal for women to experience irregular menstrual cycles during adolescence and in the transition toward menopause. Most of us expect that women in their 30’s, however, will have perfectly normal cycles. This, as I discovered in an observational study performed a number of years ago, is not always the case.1
IN BRIEF: OVULATORY DISTURBANCES DEFINITION
Refers to both anovulatory and short luteal phase cycles
TYPES OF DISTURBANCES Understimulated.Occurs when hypothalamic pituitary stimulation of the ovary is decreased OverstimulatedLuteinizing hormone levels and pulsatility are increased and the ovary is stimulated to make high levels of estrogen TREATMENT
Medroxyprogesterone (10 mg daily, cycle days 14-27) OR
Oral micronized progesterone. (three 100-mg capsules taken at bedtime, cycle days 14-27)
Spironolactone (100 mg once or twice daily) for women with androgen excess
SEE PATIENT INFORMATION SHEET- page 19 STUDY RESULTS SURPRISING
I first began to understand that cycles could be perfectly regular, cause a woman no problems or symptoms and still be associated with important health risks after studying 66 ovulatory women for an entire year. The purpose of the study was to determine whether women training for a marathon develop amenorrhea. We enrolled women of differing exercise habits who were of normal weight, were not taking oral contraceptives, reported regular cycles and had two consecutive cycles that met
criteria for normal cycle lengths (21 to 36 days) and normal ovulatory characteristics (meaning
KEYPOINT
luteal phase lengths of at least 10 days)2 Subtle
The healthy women in our
ovulation disturbances could be detected
study who experienced only
because we made the old-fashioned method of
one nonovulatory cycle
oral basal temperature recording into a scientific
during the year lost an average of 4% of their spinal bone while those with consistently normal ovulation
Progesterone is known to act on hypothalamic
tended to gain bone have no
neurons that cause an elevation of temperature.
That elevation is best detected in the morning before it is obscured by food, activity and
circadian changes in temperature. Basal temperatures taken orally by women first thing in the morning-are recorded and analyzed using a computer program that we validated against the serum midcycle luteinizing hormone (LH) peak.3 When the 66 women kept daily basal temperature records, well over one-half experienced some disturbance of ovulation. These disturbances occurred despite the fact that only 3% of all cycles were abnormal in length.1
This study showed that ovulation disturbances are common.1 It also showed that these disturbances are no more prevalent in runners than in sedentary women. Is this the only evidence that ovulation is abnormal when the period is regular? No. All of the studies examining ovulation over several cycles have shown that the luteal phase may be short or absent, despite regular flow.2,4-6 Although running does shorten the luteal phase during increasing or intense exercise, trained runners are no more likely to have disturbed ovulation than women doing normal activity.7
HEALTHY WOMEN ARE LOSING BONE
The next question is: Who cares whether ovulation is normal or not? Clearly women who want to become pregnant care. Other than those women, does it matter? The answer is an increasingly strong yes. The healthy women in our study who experienced only one nonovulatory cycle during the year lost an average of 4% of their spinal bone, while those with consistently normal ovulation tended to gain bone or have no loss.1 This is the strongest evidence that lack of cyclic normal progesterone is important for health.1
This article reviews the variations within the normal menstrual cycle interval, their causes and consequences and diagnosis and treatment. I will give you some ways to understand and to explain to your patients the reasons for what they are experiencing.
The good news for you, and most importantly your patients, is that the majority of hormonal changes within menstrual cycles are caused by an imbalance of hypothalamic origin. They are rarely caused by disease. These mixedup cycles are also highly treatable, using physiologic and acceptable therapies.
Menstrual cycle interval (days) This graph shows that cycles of a mean 28 days in length may vary markedly in progesterone production and ovulatory characteristics. Note that a cycle that is oligomenorrheic can still be ovulatory. HOW MANY TYPES OF OVULATORY DISTURBANCES ARE THERE?
For convenience, the term “ovulation disturbance" is used to refer to both anovulatory (in which an egg is not released) and short luteal phase cycles (ovulation with a luteal phase that is less than 10 days long, commonly called short luteal phase defect). Figure 1 shows that cycles can be perfectly normal in length and not be ovulatory. Paradoxically, cycles that are too long can be ovulatory.
It is useful to think of ovulation disturbances as falling into two very different types, depending on the intensity (in hormone levels and in pulse amplitude and frequency)
of hypothalamic-pituitary signals that are sent to the ovaries (Table 1). These types - both of which usually occur in cycles of regular, normal intervals - can be nicknamed "overstimulated" and "understimulated" ovulation disturbances. Separating them into two types does not mean that these categories do not blend into each other and that women cannot change from one category to the other.
TYPES OF OVULATION DISTURBANCES THEIR HORMONAL AND CLINICAL CHARACTERISTICS
Understimulated Overstimulated
Molimina increased or premenstrual syndrome
+ Body mass index is weight (kg) divided by the square of height (M); normal range is 19 – 24.34
The first category - occurring when hypothalamic-pituitary stimulation of the ovary is decreased (Table 1) - is usually silent and subclinical. In "understimulated" anovulation, the follicle usually produces the minimum estrogen levels necessary to stimulate endometrial shedding at normal intervals (although they may tend to be 32 to 36 days apart); however, ovulation either does not occur or there is shortening of the luteal phase. It was understimulated ovulation disturbances that we documented in our study of 66 ovulatory women. Women with occasional cycles, in which ovulation is not normally stimulated, commonly have no complaints, feel well, have regular cycles and are happy with few or no premenstrual symptoms and light flow. These women will be the hardest to detect clinically, but may be those found to have spine fractures near or shortly after menopause.
The second category - LH levels and pulsatility are increased and the ovary is stimulated to make high levels of estrogen-is commonly associated with obesity and signs and symptoms of androgen excess. This kind of ovulation disturbance can be understood by visualizing several follicles per cycle being stimulated, enlarging and each producing its own compliment of estrogen. (This situation is mimicked by ovulation-induction therapy for infertility using LH injections. In infertility treatment, however, ovulation is triggered by an injection of the role of the LH peak. Sometimes, this form of ovulation disturbance is called polycystic ovarian disease. In the past, we termed it Stein Leventhal syndrome. Multiple cysts are formed from stimulated follicles that did not ovulate. Women experiencing this kind of ovulation (with high estrogen levels) often come to their physician with concerns about flow. They may report menorrhagia (heavy or flooding flow, more than 16 pads soaked per menstrual period) or metoarrhagia (periods at less than 21-day intervals, midcycle spitting or flow lasting far more than six days). Other common symptoms include mastalgia, premenstrual mood changes or weight gain related to high estrogen levels.8
Ovarian androgen production increases when LH is chronically high (along with increased estrogen production) and ovulation is absent or disturbed. One of the intriguing new findings is that increased insulin levels and/or insulin resistance are also common. These women - in addition to concerns about weight gain and flow - may complain of acne and hair growing on the chin, upper abdomen or around the nipples.
WHAT ARE THE HEALTH CONSEQUENCES ASSOCIATED WITH DISTURBED OVULATION?
Having said that there are different types of ovulation disturbance, and that they present with different clinical concerns, it is obvious that the health consequences would differ. A variety of conditions are linked to ovulation disturbances (Table
2). In the understimulated ovulation disturbances-usually asymptomatic-the primary health consequence results from inadequate progesterone production. Without adequate progesterone to stimulate bone formation, normal levels of bone resorption result in bone loss. This is probably the major consequence of understimulated ovulation disturbances. Our study of normal-weight women observed this most subtle kind of ovulation disturbance in which estrogen levels were normal or only minimally decreased, yet bone loss was measurable and significant.1 Epidemiologic data in a large, population-based study confirmed our observation.9
HEALTH CONSEQUENCES OF OVULATION DISTURBANCES IN REGULAR CYCLES
Subfertility Irregular. unpredictable flow. spotting Dysfunctional uterine bleeding Endometrial hyperplasia and cancer
Anemia due to excess uterine blood loss Distressing premenstrual symptoms Acne. hirsutism, oily skin, androgenic alopecia Polycystic ovarian changes Mastalgia and fibrocystic breast disease Increased risk for breast cancer Accelerated bone loss/low bone density Potential cardiovascular risks/androgen excess (maybe from lack of
KEYPOINT Although the precise
Not all ovulation disturbances are subtle. In
mechanisms for
overstimulated ovulation disturbances, the health
ovulatory disturbances
consequences resulting from excess estrogen are
are poorly understood,
coupled with progesterone deficiency and sometimes
clear that they originate
androgen excess. If estrogen levels are high, flow
with an imbalance or
increases, troubling premenstrual symptoms occur or
incoordination in the
signs and symptoms of androgen excess are present.
signals sent from the
Based on known physiologic effects of estrogen and
hypothalamus and
progesterone, and despite incomplete epidemiologic
pituitary gland to the
data, it is now possible to show health risks related to
ovarian follicle.
chronically disturbed ovulation (Table 2). Ovulation
disturbances with high estrogen levels are associated with irregular and heavy uterine bleeding,10 anemia due to excess menstrual blood loss and sometimes disturbing premenstrual symptoms, termed "the premenstrual syndrome" or PMS.8 If anovulation and high estrogen levels are chronic, endometrial hyperplasia and cancer risks are substantial, and the risk for breast cancer also appears to increase.10-12 In chronic anovulation with high estrogen levels, breast symptoms are increased, mastalgia sometimes develops and breasts tend to be fibrocystic.13 Acne and hirsutism - often with accompanying cystic enlargement of the ovary-are also strongly and causally related to nonovulation 14 Importantly (good news for women with past acne and hirsutism) the bone loss shown in understimulated anovulation does not appear to occur in women with androgen excess who are relatively protected against low bone density.15
Knowing that health risks are associated with disturbances of the menstrual cycle and especially with absent or abnormal ovulation, we need to understand how they develop and how to diagnose them.
THE PATHOPHYSIOLOGY OF OVULATORY DISTURBANCES
Most ovulatory disturbances and changes in menstrual cycles during the reproductive years are caused by adaptations related to life cycle, changes in weight, psychosocial stresses, excessive exercise or illness.16
Although the precise mechanisms for ovulatory disturbances are poorly understood, it is clear that they originate with an imbalance or incoordination in the signals sent from the hypothalamus and pituitary gland to the ovarian follicle. They are rarely an ovarian problem or disease. Few researchers, however, have prospectively studied sequential menstrual cycles. Ovulatory disturbances are both variable from cycle to cycle and entirely reversible to normal.
The first concept is that ovulation disturbances commonly occur during vulnerable times within the normal life cycle, such as immediately after puberty, following pregnancy and in the transition into menopause.2'10~17 Changes during puberty are expected, as the entire hypothalamic-pituitary-ovarian axis is developing into its adult reproductive potential. Childbirth is associated with major decreases in hormonal levels as placental hormones are removed, prolactin rises and sleep is disturbed with a demanding new infant. It is less clear why perimenopause should have disturbances of ovulation. There is evidence, however, that intraovarian and ovarian feedback to the pituitary and hypothalamus may be altered.17-19 I have postulated that inhibin (an ovarian protein hormone made within the granulosa and corpus luteum cells whose job is to suppress follicle-stimulating hormone [FSH]) may be made in lower quantities and, thus, allow higher pituitary FSH secretion.20
The pituitary and hypothalamic signals to the ovary appear to be variable and suppressed in response to many changes in the external and internal environments. Four categories of fundamental threats have been shown to disturb ovulation: physical illness, weight loss, emotional distress and intense exercise training (usually combined with young age, stress and weight.21 The most prevalent and difficult to diagnose reasons for ovulation disturbances are subtle but emotionally important. The belief that one must limit food intake to prevent obesity is such a stressor. This phenomenon, called dietary restraint, has been shown in three different groups of women to occur in association with luteal-phase defects.6,22,23
The best evidence that illness causes suppression of hypothalamic-pituitary messages comes from a study of menopausal women admitted to coronary or intensive care units. On admission, their serum FSH levels were abnormally low for menopausal women and increased toward normal with recovery.24 Weight loss is associated with the development of anovulation25 or with an increased prevalence of luteal-phase disturbances in exercising women who lost weight compared with similarly exercising women without weight loss.7 Exercise training in normal-weight women has been shown to temporarily and reversibly suppress ovulation.26-27 Ovulation disturbances are common during the school year in young women studying to become nurses-these ovulatory changes improve during the summer away from school.5 As mentioned before, very subtle stresses arising from attitudes toward food, without differences in weight, diet or exercise, are associated with luteal-phase defects. The state of being stressed is so individual and so variable, however, that measuring serum cortisol levels does not help with the diagnosis.
Times of ovarian hormonal change appear to produce vulnerable times for the development of ovulation disturbances. Such transitions include recovery following amenorrhea, a sudden decrease in an athlete's training and when the oral contraceptive pill (OCP) is stopped. Following use of OCPs, the hypothalamus-used to suppressive high levels of exogenous hormones-may need time to find its own cyclic rhythm, especially if ovulation was never firmly established before starting OCPs. It appears that weight gain and/or major stress during such a transition may
predispose toward estrogen excess and overstimulated anovulation. Because we have shown that spontaneous recovery occurred within one year for almost 50% of women enrolled in the study of abnormal menstrual cycles, ranging from amenorrhea to subclinical ovulatory disturbances, these hormonal imbalances are highly reversible and/or treatable.28
KEYPOINT THE SUBTLE SIGNS OF OVULATION AND OVULATION DISTURBANCES Spontaneous recovery occurred within one year
Diagnosis of menstrual cycle disturbances is
for almost 50% of women
usually made with blood or other tests. Blood tests,
enrolled in the study of
however, are of limited diagnostic usefulness for
abnormal menstrual
several reasons. The first reason is that the
cycles; these hormonal
hormonal changes of the menstrual cycle vary
imbalances are highly
from cycle to cycle within a particular woman and
reversible and/or treatable.
certainly between women. The second reason is that estrogen, progesterone, testosterone, LH and
FSH are pulsatile, so a single value may be misleading. Finally, daily serum samples for progesterone are necessary to make the diagnosis of a short luteal phase.
THE MOLIMINA QUESTION: CAN YOU TELL BY THE WAY YOU FEEL THAT YOUR PERIOD IS COMING?
Molimina present: (spontaneously volunteered, no prompting)
Report of side of the breast (not nipple) tenderness
Breast tenderness in addition to appetite, fluid and mood changes
Molimina possible:
Patient responds positively to question about breast changes saying that she experiences soreness on the sides of her breasts before her period
Fluid retention and disappearance of midcycle mucus volunteered
Molimina absent-anovulation
Nothing is volunteered or elicited with open-ended questions
Mood symptoms are volunteered (with nothing else)
CONFIRMATION OF THE SENSITIVITY AND SPECIFICITY OF THE MOLIMINA QUESTION
In 61 consecutive women with androgen excess and usually regular cycles. Gold standard for ovulation = progesterone level >= 16 nmol/L days -11 to –1 before flow.
Progesterone <16 Progesterone >= 16
Given all the difficulties with usual laboratory testing for ovulation, it is useful to ask whether there exist certain symptoms that can be found in a patient's history that indicate hormonal actions. If these experiences exist, they could potentially be used as predictable, reliable diagnostic indicators. Molimina (a word meaning the set of experiences before flow that indicate ovulation) although needing further validation, is probably useful to diagnose ovulation. We have shown that the absence of molimina is a highly sensitive and specific test for anovulation (Table 3 and 4).29 Molimina - as it is most specifically used-means physical and emotional experiences that are postovulatory and variably noticeable. By definition, these experiences are neither sufficiently intense nor chronic to interfere with a woman's quality of life. If these symptoms make a woman miserable, we would call her concerns PMS. In other words, molimina includes many of the same experiences as PMS, but these experiences are less intense. As presently used, PMS does not mean ovulation. As discussed under overstimulated ovulation disturbances, the most severe mood, breast and fluid symptoms occur when ovulation is absent and estrogen high.8
The most specific of the moliminal symptoms indicating ovulation, in my experience, is high lateral breast tender-ness (i.e., sensitivity toward the axillae but never the nipple soreness or generalized mastalgia that are signs of high estrogen). Diagnosis of ovulation is more secure if lateral breast tenderness is associated with fluid retention or bloating and increases in appetite with or without emotional sensitivity (e.g., frustration, sense of sadness or anxiety).
To use molimina as a test of ovulation (Table 3),
KEYPOINT
ask your patient: "Can you tell by the way you feel
Because progesterone
that your period is coming?" Let your patient
causes an average luteal
volunteer an answer. Encourage her recollections
phase basal temperature
until she can remember no other experiences. Then,
increase of O.3° C,
if you need to prompt her, ask "Are you ever aware
documentation of
of changes in your breasts?" If she says "yes,"
temperature is a reliable
watch her hands. If she makes no gesture, ask her
way of confirming the
where in her breasts she has tenderness. If she
presence of ovulation
volunteers high-lateral breast tenderness, I would
and the duration of the
believe she is ovulatory. If she gestures toward
luteal phase
and/or mentions front or whole breast soreness, however, she is likely to be nonovulatory because
estrogen is usually not high before flow.
Another sign useful for diagnosing ovulation is the characteristic time pattern of normal cervical mucus. Increasing estrogen levels stimulate cervical glands to produce a characteristic clear, glistening, stretchy mucus. Mucus typically increases from a few days after flow to a maximum in volume and stretchiness at the midcycle estrogen peak. The amount of stretch is roughly proportional to the estrogen level. Mucus that stretches 4 cm to 5 cm is diagnostic of estrogen levels in the range of 800 pmol/L to 1,000 pmol/L, typical midcycle peak levels. Following midcycle, if ovulation occurs, mucus disappears entirely. Progesterone inhibits the cervical glandular secretions, which is one of the reasons that progestins are used in oral contraceptives. The presence of stretchy mucus, therefore, is a way to diagnose high estrogen levels. The presence of stretchy mucus (about cycle day 12 to 16) and then its disappearance is highly supportive of the clinical diagnosis of ovulation. On the other hand, abundant, stretchy mucus just before or during flow is diagnostic of anovulatory, dysfunctional uterine bleeding.
If, following a history, physical examination and upon review of records (including asking your patient to keep records concerning breast tenderness and mucus), the diagnosis of ovulation disturbances is still unclear, daily oral morning temperature records should be kept. Because progesterone causes an average luteal phase basal temperature increase of 0.3°C, documentation of temperature is a reliable way of confirming the presence of ovulation and the duration of the luteal phase.
Basal temperature methods have been faulted in the past, not because there is any doubt that progesterone influences temperature, but because other variables, such as eating, illness and change in the time of day in which the temperature is taken, all influence oral basal temperature readings. Basal temperature has also been criticized because many nonsystematic methods have been used to identify the onset of temperature rise. These difficulties can be overcome if the temperatures are taken with a digital thermometer, recorded in a list to two decimal places (rather than being graphed by the woman in which error is common) and a quantitative rather than "eyeball" method for analysis is used. We have shown that the basal temperature shift day lags behind the LH peak day by about three days but is highly correlated with it.
To analyze the data, using the most simple method, average all of the temperatures in one cycle. Then, starting on the first day of the same cycle, compare that average
to the list of temperatures. The day that the temperature rises above the mean and stays above until the next flow is the onset of the luteal phase.3 The luteal phase length includes all of the days from the temperature increase to the day before the next period starts.
HOW DO I TREAT OVULATION DISTURBANCES?
Ovulatory disturbances represent a variable and temporary imbalance for many women. Because there is a very important etiologic connection between emotional stresses, eating attitudes and other aspects of personhood, increased self-understanding may play an important role in developing normal ovulation. Women who are underweight or over-exercising may only need to gain a little weight or try to understand more about exercise as a stress reducer to restore normal ovulation. Certainly, explaining both the variability of cycles as being normal and teaching your patient about how she can "read" her body will also help. Remember to reassure her that pregnancy is possible. If, following these measures, ovulation disturbances persist, there are easy, effective and acceptable medical therapies available.
LUTEAL PHASE REPLACEMENT THERAPY
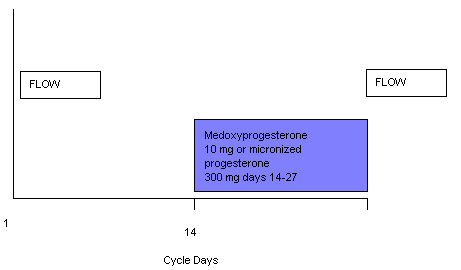
The goal of treating ovulatory disturbances is to
KEYPOINT
restore the normal balance of estrogen and progesterone. This restoration is accomplished by
The goal of treating
prescribing progesterone in doses and on a schedule
ovulatory disturbances
that mimics the missing normal progesterone
is to restore the normal
secretion. Progesterone treatment can be given either
balance of estrogen
as medroxyprogesterone (10 mg/day) or oral
and progesterone. This
micronized progesterone (three 100-mg capsules at
is accomplished by
bedtime) for a minimum of 14 days per cycle (Figure
prescribing
2). If ovulation disturbances are from ovarian
progesterone in doses
overstimulation, treatment of high androgen levels
and on a schedule that
(that interfere with follicle development toward
mimics the missing
ovulation) must be part of the treatment. If your patient
normal progesterone secretion.
reports or you observe acne, male-pattern facial and body hair or temporal balding, a prescription for the antiandrogen spironolactone will be necessary in addition to cyclic progesterone replacement. Spironolactone - a hypertension therapy designed to be an antagonist to aldosterone-is a true nuclear androgenreceptor blocking agent and is effective in a dose of 100 mg once or twice a day.30 Spironolactone given without progesterone, however, will cause irregular and sometimes heavy flow. Cyclic progesterone or medroxyprogesterone in this circumstance needs to be given earlier in the cycle (e.g., cycle days 10 to 25) or in higher doses of 15mg/day to 20 mg/day of medroxyprogesterone acetate (MPA) for 16 or 18 days to control flow. If your patient is overweight, the dose needs to be increased from 10 mg/day to 15 mg/day of medroxyprogesterone given for at least 14 days/month.
For the woman with hypothalamic disturbances of
KEYPOINT
ovulation and normal estrogen levels, the same progesterone prescription can be given, but she
There are no serious side
should start on day 14 and continue until day 27 of
effects with cyclic
her cycle. The earlier flow starts-in relationship to
progesterone therapy; it
the onset of progesterone therapy-the higher the
does not increase or cause
estrogen effect on the endometrium. If flow starts
migraine headaches,
before day 12 (which rarely occurs except in
thrombosis or breast cancer and clearly
perimenopause), progesterone should be started
prevents endometrial
earlier in the cycle (e.g., day 10) and continued for
14 days. If flow starts before the ninth day of MPA
therapy, for the next three cycles the dose should be increased and given for 16 days per cycle. Should no flow occur following any cycle of MPA (if pregnancy is possible, it must be excluded), the next dose should be begun 14 days after stopping the last 14-day cycle. (These instructions are explained in the patient information sheet.)
If a woman chooses to take oral micronized progesterone and flow starts early, it is more difficult to control flow. I would suggest continuing the bedtime micronized progesterone and adding MPA in a dose of 10 mg/day for the same cycle days as described above. Because these flow disturbances can be upsetting, it is important to explain to your patient that it will take a few cycles before balance is restored.
Most women are grateful for therapy that restores their normal hormonal balance; it prevents health risks associated with anovulation, such as endometrial cancer, anemia, loss of bone and breast soreness and cysts. Medroxyprogesterone therapy (for only 10 days per cycle) increased spinal bone density by 2% per year in a randomized, placebo-controlled trial.28 There are no serious side effects with cyclic progesterone therapy; it does not increase or cause migraine headaches, thrombosis or breast cancer31 and clearly prevents endometrial cancer. Although adverse experiences are reported when medroxyprogesterone is given to women taking conjugated equine estrogen after menopause, randomized, placebo-controlled trials involving women using transdermal estrogen therapy as well as menopausal women not on estrogen showed no adverse mood symptoms related to progesterone.32'33 The use of cyclic progesterone therapy will prevent the need for hysterectomy in women with abnormal bleeding or otherwise asymptomatic fibroids. Cyclic
progesterone therapy should be used before OCP, dilatation and curettage or hysterectomy for a woman with dysfunctional bleeding.
CONCLUSION
Ovulatory disturbances, such as short luteal phase or anovulatory cycles, are common in reproductive-age women and carry many health consequences. Although some women will come to see you with reproductive hormone-related problems, most will not complain. Some women will see you because of severe breast swelling and only be found incidently to have multiple ovarian cysts. Alternatively, the patient may report spotting or heavy flow. Most commonly, the diagnosis is suspected only when a woman with regular periods has difficulty getting pregnant or is specifically asked and reports no molimina. If androgen excess occurs in conjunction with ovulatory disturbances, it is treated with the spironolactone (100 mg/day continuously) along with cyclic medroxyprogesterone or oral micronized progesterone for 14 days per cycle. Cyclic progesterone therapy provides "luteal-phase replacement" that restores the normal cyclic estrogen/progesterone balance and increases bone density.
REFERENCES
Prior JC, Vigna YM, Schechter MT, et al: Spinal bone loss and ovulatory disturbances. N Engl J Med 1990; 323:1221-7.
Vollman RF: The menstrual cycle. In: Friedman EA (ed.): Major Problems in Obstetrics and Gynecology. vol 7. W.B. Saunders Company, Toronto, 1977, pp.11-193.
Prior JC, Vigna YM, Schulzer M, et al: Determination of luteal phase length by quantitative basal temperature methods: validation against the midcycle LH peak. Clin Invest Med 1990; 13:123-31.
Doring GK: The incidence of anovular cycles in women. J Reprod Fertil 1969; (Suppl. 6): 77-81.
Nagata I, Kato K, Seki K, et al: Ovulatory disturbances. Causative factors among Japanese student nurses in a dormitory. J Adolesc Health 1986; 7:1-5.
Barr SI, Janelle KC, Prior JC: vegetarian versus nonvegetarian diets, dietary restraint, and subclinical ovulatory disturbances: prospective six month study. Am J Clin Nutr 1994; 60:887-94.
Bullen BA, Skrinar GS, Beitins IZ, et al: Induction of menstrual disorders by strenuous exercise in untrained women. N EngI J Med 1985; 312:1349-53.
Hammarback 5, Damber J, Backstrom T: Relationship between symptom severity and hormone changes in women with premenstrual syndrome. J Clin Endocrinol Metab 1989; 68:125-30.
Sowers MF, Shapiro J, Zhang B: Urinary ovarian and gonadotrophin hormones in premenopausal women with low bone mass. J Bone Miner Res 1995; 10 (S):M377.
10. Fraser IS, Baird DT: Endometrial cystic glandular hyperplasia in adolescent girls. J Obstet Gynaecol 1972; 79:1009-13.
11. Coulam CB, Annegers JF, Kranz JS: Chronic anovulation syndrome and associated neoplasia. Obstet Gynaecol 1983;
12. Cowan LO, Gordis L, Tonascia JA, et al: Breast cancer incidence in women with a history of progesterone deficiency. Am
13. Sitruk-Ware LR, Stenkers N, Mowezowicz, et al: Inadequate corpus luteal function in women with benign breast disease. J
14. Berga SL. Yen SSC: Opicidergic regulation of LH pulsatility in women with polycystic ovary syndrome. Cm Endocrinol
15. Di Carlo C, Shaham Z, MacDougall J, et al: Polycystic ovaries as a protective factor for bone mineral loss in young women
with amenorrhea. Fertil Steril 1992; 57:314-9
16. Prior JC: Exercise-associated menstrual disturbances. In: Adashi EY, Rock JA, Rosenwaks Z, (eds.): Reproductive
Endocdnology Surgery and Technology. Raven Press, New York, 1996, p. 1077-91.
17. Van Look PF, Lothian H, Hunter WM, et al: Hypothalamic-pituitary-ovarian function in penmenopausal women. Clin
18. Metcalf MG, Donald RA, Livesey JH: Pituitary-ovarian function in normal women during the menopausal transition. Clin
19. Hee JP, MacNaughton J, Bangah M, et al: Perimenopausal patterns of gonadotrophins, immunoreactive inhibin, oestradiol
and progesterone. Maturitas 1993; 18:9-20.
20. Prior JC: The perimenopause: Pathophysiology, symptoms and therapy. In: Medifacts Healthcare Communications (tape).
21. Prior JC: Endocrine “conditioning” with endurance training: A preliminary review. Canadian Journal of Applied Sport
22. Schweiger U, Tuschi RJ, Platte P, et al: Everyday eating behavior and menstrual function in young women. Fertil Steril
Barr SI, Prior JC, Vigna YM: Restrained eating and ovulatory disturbances: Possible implications for bone health. Am J Clin
23. Warren MP; Siris ES, Petrovich C: The influence of severe illness on gonadotropin secretion in the post-menopausal
female. J Clin Endocrinol Metab 1977; 45:99-104.
24. Pirke KM, Schweiger U, Strowitzki T, et al: Dieting causes menstrual irregularities in normal weight women through
impairment of luteinizing hormone. Fertil Steril 1989; 51:263-8.
25. Shangold MM, Freeman R, Thysen B, et al: The relationship between long-distance running, plasma progesterone, and
luteal phase length. Fertil Steril 1979; 31:130-3.
26. Prior JC, Ho Yeun B, Clement P, et al: Reversible luteal phase changes and infertility associated with marathon training.
27. Prior JC, Vigna YM, Barr SI, et al: Cyclic medroxyprogesterone treatment increases bone density: A controlled trial in
active women with menstrual cycle disturbances. Am J Med 1994; 96:521-30.
28. Prior JC, Vigna YM: Absence of molimina: The clinical or self-diagnosis of anovulation. Soc Menst Cycle Res 1987;
29. Corrol P; Michaud A, Menard J, et al: Anti-androgenic effect of spironolactone: Mechanism of action. Endocrinology 1975;
30. Chang KJ, Lee TTY, Linares-Cruz G, et al: Influence of percutaneous administration of estradiol and progesterone on
human breast epithelial cell cycle in vivo. Fertil Steril 1995; 63:785-91
31. Kirkham C, Hahn PM, van vugt DA, et al: A randomized, double-blind, placebo-controlled cross-over trial to assess the
side effects of medroxyprogesterone acetate in hormone replacement therapy. Obstet Gynecol 1991; 78:93-7
32. Prior JC, Alojado N, McKay DW, et al: No adverse effects of medroxyprogesterone treatment without estrogen in
postmenopausal women: Double-blind, placebo-controlled, cross-over trial. Obstet Gynaecol 1994; 83:24-8.
33. Thomas AE, McKay DA, Cutlip MB: A nomograph method for assessing body weight. Am J Clin Nutr 1976; 29:302-304.
FOR MDL WEBSITE MAZAGON DOCK LIMITED ADVERTISEMENT REF. NO. MDL/HR-CR/REC/24/2013 Mazagon Dock Limited (MDL) is India’s leading Shipbuilding Company with ISO 9001:2008 accreditation. It is a profit-making Central Government Schedule ‘A’ PSU under the Ministry of Defence, Department of Defence Production, engaged primarily in the building of Warships and Submarines for the Indian
Knapp, W.M., R.F.C. Naczi, W.D. Longbottom, C.A. Davis, W.A. McAvoy, C.T. Frye, J.W. Harrison, and P. Stango, III. 2011. Floristic discoveries in Delaware, Maryland, and Virginia. Phytoneuron 2011-64: 1–26. Published 15 December 2011. ISSN 2153 733X FLORISTIC DISCOVERIES IN DELAWARE, MARYLAND, AND VIRGINIA ESLEY M. KNAPP Maryland Department of Natural Resources ROBERT F. C. NACZI
 to the list of temperatures. The day that the temperature rises above the mean and stays above until the next flow is the onset of the luteal phase.3 The luteal phase length includes all of the days from the temperature increase to the day before the next period starts.
HOW DO I TREAT OVULATION DISTURBANCES?
to the list of temperatures. The day that the temperature rises above the mean and stays above until the next flow is the onset of the luteal phase.3 The luteal phase length includes all of the days from the temperature increase to the day before the next period starts.
HOW DO I TREAT OVULATION DISTURBANCES?