Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Microsoft word - 2011 a meta-analysis of agomelatine versus placebo for the treatment of major depressive disorder
A meta-analysis of agomelatine versus placebo for the treatment of
1. School of Medicine, Faculty of Health Sciences, Queen’s University, Kingston, Ontario
Submitted on: March 31st, 2011 Word Count: 1884 Total pages: 11 Contact:
Derrick Tam B.Sc. (Hon) MD Candidate 2014 School of Medicine Queen’s University Kingston, Ontario Canada derrick.tam@queensu.ca 647-200-3639 Address 2-227B Earl St. Kingston, ON K7L2H6
Abstract Background: Major depressive disorder (MDD) is a significant cause of morbidity and mortality in
Canadians. Approximately 30% of patients with MDD do not respond to treatment. Agomelatine, a novel
drug targeting the melatonin pathway has been shown to be effective in treating MDD in a number of
randomized clinical trials. A meta-analysis was conducted on all available placebo-controlled randomized
trials to determine the efficacy of agomelatine in treating MDD.
Methods: A literature search was conducted using MEDLINE and EMBASE. Original research was
selected based on inclusion/exclusion criteria and the quality of the studies was evaluated. Five studies
were included in a random effects meta-analytic model developed by Cochrane.
Results: Agomelatine demonstrated statistically significant efficacy compared to placebo when evaluated
on the HAM-D. However, agomelatine failed to demonstrate clinical significance compared to placebo
Conclusion: Agomelatine demonstrates similar efficacy to currently available treatment for MDD.
However, given agomelatine’s unique mechanism of action, it may be useful for the treatment of patients
who are resistant to first line therapy.
Introduction Major depressive disorder (MDD) is a chronic disease that is estimated to affect about 8% to 11% of
Canadians1, 2. MDD is associated with significant morbidity and mortality and is characterized by
depressed mood, loss of interest in activities and decreased energy level3. One of the theories regarding
the neurobiology of depression is the monoamine hypothesis4. The monoamine hypothesis posits that
decreased levels of the monoamine neurotransmitters, such as serotonin (5-HT) and norepinephrine (NE),
in certain regions of the brain lead to mood dysregulation and the clinical manifestations of MDD. Thus,
many antidepressants have been developed in an attempt to increase central levels of these monoamines.
Antidepressants are categorized based on their mechanism of action. The tricyclic antidepressants (TCAs)
and serotonin-norepinephrine reuptake inhibitors (SNRIs) inhibit the reuptake of NE and 5-HT while
selective serotonin reuptake inhibitors (SSRIs) inhibit the reuptake of only 5-HT. SSRIs and SNRIs are
first line therapy for treating MDD because of their safer side effect profile and better tolerability relative
to TCAs5. Theoretically, each drug in the same class act by a similar mechanism to treat depression but in
practice, patients respond differently to these medications6. Approximately 30% of the MDD patients do
not respond to treatment and are classified as “treatment resistant” after failing two or more courses of
antidepressants7. The two most recently Health Canada approved antidepressants are Pristiq
(desvenlafaxine) and Cymbalta (duloxetine), both SNRIs8, 9. Nevertheless, the efficacy of these two drugs
are comparable to current available SNRIs or SSRIs but at a higher acquisition costs and therefore have
not been recommended for first line therapy8, 9. The paucity of effective treatment options for this large
population suffering from MDD demonstrates the need for novel therapies that target other aspects of the
Currently, there is a new drug that is in phase III clinical trials for the treatment of MDD, agomelatine, a
synthetic analog of melatonin10. Melatonin is a neurotransmitter produced by the suprachiasmatic nucleus
that regulates circadian rhythm, including the sleep-wake cycle11. Desynchronization of normal circadian
rhythm, resulting in sleep disturbance has been associated with MDD. In fact, the Diagnostic and
Statistical Manual of Mental Disorders (DSM-IV) states that disturbed sleep is one of the diagnostic
criteria for MDD12. Agomelatine is an agonist at the MT1 and MT2 receptors and an antagonist at the 5-
HT1C receptor13. Clinical trials have shown agomelatine to be efficacious in treating patients with MDD as
evidenced by improvement in the Hamilton Depression Rating Scale (HAM-D) and other measures of
MDD severity14-18. The sample sizes in these studies were small and may limit the detection of the
treatment effect. Previously, Montgomery and Kasper conducted a pooled analysis of three placebo-
controlled trials on agomelatine and grouped results based on disease severity but did not examine the
efficacy of each dose separately19. In addition, since the publication of the pooled analysis, two additional
clinical trials have been published. Thus an updated meta-analysis is necessary to evaluate this new
drug17, 18. The purpose of this review is to conduct a meta-analysis utilizing the results of the few available
Methods The population to be studied was patients suffering from MDD based on DSM-IV criteria, treated for at
least six weeks (minimum amount of time for medication to demonstrate an effect7) on placebo or
agomelatine (25 or 50mg). Only randomized double-blinded placebo-controlled trials utilizing the HAM-
A literature review was conducted using MEDLINE and EMBASE to search for clinical trials evaluating
agomelatine for clinical trials. The following keywords were used in the search: agomelatine and major
depression. The search was limited to original articles, human, English and clinical trials. The author
reviewed the methods to determine if studies met inclusion criteria. Appropriate trials were then assessed
for quality using the Jadad scoring tool. Only studies with Jadad score of three or greater were included in
A meta-analysis was conducted to estimate an overall mean effect based on the individual studies
obtained from the literature search. From each of the studies, the overall between group differences for
each dose of agomelatine and placebo were extracted along with the associated standard error of the mean
(SE). A random-effects meta-analytic model developed by Cochrane (Review Manager 5) was used in
this study examining the effects of agomelatine at 25 and 50mg compared to placebo. The effect size was
weighted based on standard error of the mean and model yielded a pooled mean point estimate and a 95%
confidence interval (CI). Funnel plots for both meta-analyses were generated examining the relationship
Results Twelve articles were extracted based on search criteria in the MEDLINE and EMBASE database. Seven
articles were excluded based on inclusion and exclusion criteria: inappropriate dose/diagnosis (n=2), lack
of placebo control (n=4), and open-label (n=1). The author assigned each of the five remaining articles a
Jadad score20. All trials examined were at least of good quality based on the Jadad scale and no studies
were removed (median score of 4). The five articles were randomized, double-blind, placebo-controlled,
multi-centred trials of short duration (6 or 8 weeks). The studies evaluated two doses of agomelatine (25
and 50 mg) in either a fixed or a flexible dose regimen in which patients were uptitrated from 25 to 50 mg
at a certain time point in the trial if they deemed the original dose not effective. Two studies included a
flexible dosing schedule and both studies were included in the 25mg and 50mg analysis. Inclusion and
exclusion criteria were similar in all the studies. Patients that met the DSM-IV criteria for depression
were included. Studies excluded patients with relevant psychiatric comorbidities, treatment resistant to
marketed antidepressants and other non-pharmacological treatments. Trial characteristics and results were
Two meta-analyses were conducted. The first meta-analysis examined the overall mean effect based on
studies that evaluated the 25mg dose (Figure 1) while the second meta-analysis evaluated the 50mg dose
(Figure 2). Since the final number of patients on either 25mg or 50mg could not be extracted from two of
the studies with a flexible dosing schedule14, 16, the aggregated data was used in both analyses. In the fixed
dose studies that examined both the 25 and 50mg, the results were disaggregated into the respective doses
and analyzed according17, 18. The 25mg analysis included all five studies and heterogeneity was found to
be not significant (2= 5.89, p=0.21). Pooled results demonstrated that 25mg agomelatine was
significantly different compared to placebo by 2.16 in HAM-D score changes from baseline to final visit
(95% CI 1.29-3.03, p<0.01). Similarly, in the 50mg analysis, 4 studies were included and heterogeneity
was not significant (2= 2.50 p=0.48). Pooled results demonstrated that 50mg agomelatine was also
significantly different than placebo by 2.18 in HAM-D score changes from baseline to final visit (95% CI
1.24-3.13). Funnel plot asymmetry was not tested due to low sample size.
Discussion Given that current treatment options for MDD are not effective for about 30% of the patients, the
introduction of a novel anti-depressant targeting a different aspect of the pathogenesis of depression is
promising. However, results from this meta-analysis demonstrate only modest benefits of agomelatine for
the treatment of MDD compared to placebo. Though results demonstrated significant differences
favouring agomelatine over placebo, the clinical significance of these results merit further discussion.
Specifically, a study has shown that a three-point difference in change between active medication and
placebo is indicative of clinical significance21. The results from the meta-analysis of both doses of
agomelatine fall short of this threshold definition of clinical significance. These results are similar to that
of a meta-analysis of published and unpublished studies conducted by the European Medicines Agency
that found a 1.5 difference in HAM-D change to be statistically significant but only marginally clinically
significant22. However, these results are different from the earlier study by Montgomery and Kasper that
found a 2.86 point difference overall and higher differences when patients were categorized based on
severity19. Furthermore, the results from this analysis suggested that there were no clinically significant
differences in efficacy between the 25mg and 50mg dose of medication. Due to the limitations in the data
presented in these articles, it was not possible to conduct a meta-analysis on other clinically significant
outcomes such as response or remission on the HAM-D scales. Visual inspection of the funnel plots
suggested minimal publication bias of trials, though a larger sample size is needed for statistical testing.
Generally, the studies were quite similar as demonstrated by the results from the meta-analysis that
showed heterogeneity to not be significant for both doses. This was expected as methods,
inclusion/exclusion criteria were similar for all studies, resulting in a well-defined population for this
meta-analysis. The study population can be described as patients suffering from moderate to severe
depression (based on initial HAM-D scores) that were not treatment resistant and did not suffer from
other psychiatric comorbidities. This patient population may not reflect true clinical settings as patients
often fail to respond to multiple treatments7 and present with multiple psychiatric comorbidities. This
highlights the paucity for additional studies that examine the use of agomelatine in treatment resistant
depression as this novel treatment may help those that are not responding to first line therapy that target
NE/5-HT neurotransmitter systems. In addition, most trials were 6 weeks in length with the longest trial
being 8 weeks. This is a short duration of treatment as MDD is an illness of much longer duration,
making it difficult to assess long-term tolerability and efficacy of the medication. In fact, the STAR*D
trial demonstrated that of those that do respond to medication, one third responded after six weeks7. Thus,
trials of greater lengths would be useful to determine the lasting benefits of agomelatine.
The measured effect sizes in this meta-analysis were similar to those observed in the duloxetine and
desvenlafaxine trials in the treatment of MDD23-27. Given the results of the meta-analysis, agomelatine
should not be recommended as first line treatment for MDD, given that current medications are more
cost-effective. However, it may have a role in treating patients that do not respond to medications that
target the serotonergic and noradrenergic systems. Additional research examining the efficacy of
agomelatine in this treatment-resistant population is warranted before further recommendations may be
Figure 1. Forest plot of trials evaluating agomelatine 25 mg versus placebo. Outcome reported as difference in mean change HAM-D scores with 95% confidence intervals.
Figure 2. Forest plot of trials evaluating agomelatine 50 mg versus placebo. Outcome reported as difference in mean change HAM-D scores with 95% confidence intervals.
Table 1. Characteristics and outcomes of agomelatine randomized placebo controlled trials included in the meta-analysis Study Baseline Estimate (SE) 95% Confidence Interval
Study duration: 6 weeks Dosing: Flexible Olie and Kasper (2006)
Dosing: Flexible Zajecka et al. (2010)
Study duration: 8 weeks Dosing: Fixed Stahl et al. (2010)
Study duration: 8 weeks Dosing: Fixed Estimate of the difference between groups in final change in HAM-D score from baseline to last visit. Ago 25- Agomelatine at 25 mg/d, Ago 50- Agomelatine at 50 mg/d, Ago 25-50- Agomelatine at 25 or 50 mg/d, SE- standard error of the mean, n- sample size
References 1.
Mood Disorders Society of Canada. Quick Facts: Mental Illness & Addiction in Canada. Second ed2007.
Patten SB, Kennedy SH, Lam RW, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) clinical guidelines for the management of major depressive disorder in adults. I. Classification, burden and principles of management. J Affect Disord. Oct 2009;117 Suppl 1:S5-14.
Bauer M, Bschor T, Pfennig A, et al. World Federation of Societies of Biological Psychiatry (WFSBP) Guidelines for Biological Treatment of Unipolar Depressive Disorders in Primary Care. World J Biol Psychiatry. 2007;8(2):67-104.
Maletic V, Robinson M, Oakes T, Iyengar S, Ball SG, Russell J. Neurobiology of depression: an integrated view of key findings. Int J Clin Pract. Dec 2007;61(12):2030-2040.
Lam RW, Kennedy SH, Grigoriadis S, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) clinical guidelines for the management of major depressive disorder in adults. III. Pharmacotherapy. J Affect Disord. Oct 2009;117 Suppl 1:S26-43.
Cipriani A, Furukawa TA, Salanti G, et al. Comparative efficacy and acceptability of 12 new-generation antidepressants: a multiple-treatments meta-analysis. Lancet. Feb 28 2009;373(9665):746-758.
Rush AJ. STAR*D: what have we learned? The American journal of psychiatry. Feb 2007;164(2):201-204.
Canadian Agency for Drugs and Technologies in Health (CADTH). CEDAC Final Recommendation and Reasons for Recommendation for Duloxetine (MDD). Common Drug Review. CADTH; 2008.
Canadian Agency for Drugs and Technologies in Health (CADTH). CEDAC Final Recommendation and Reasons for Recommendation for Desvenlafaxine. Common Drug Review. CADTH; 2009.
http://clinicaltrials.gov/ct2/results?term=agomelatine. Accessed March 1st, 2011.
Lam RW. Addressing circadian rhythm disturbances in depressed patients. J Psychopharmacol (Oxford). Sep 1 2008;22(7 Suppl):13-18.
Psychiatric Association A. DSM-IV-TR: Diagnostic and statistical manual of mental disorders, fourth . . Jan 1 2000:943.
Fuchs E, Simon M, Schmelting B. Pharmacology of a new antidepressant: benefit of the implication of the melatonergic system. Int Clin Psychopharmacol. Feb 1 2006;21 Suppl 1:S17-20.
Kennedy SH, Emsley R. Placebo-controlled trial of agomelatine in the treatment of major depressive disorder. Eur Neuropsychopharmacol. Feb 1 2006;16(2):93-100.
Lôo H, Hale A, D'haenen H. Determination of the dose of agomelatine, a melatoninergic agonist and selective 5-HT(2C) antagonist, in the treatment of major depressive disorder: a placebo-controlled dose range study. Int Clin Psychopharmacol. Sep 1 2002;17(5):239-247.
Olié JP, Kasper S. Efficacy of agomelatine, a MT1/MT2 receptor agonist with 5-HT2C antagonistic properties, in major depressive disorder. Int J Neuropsychopharmacol. Oct 1 2007;10(5):661-673.
Stahl SM, Fava M, Trivedi MH, Caputo A, Shah A, Post A. Agomelatine in the treatment of major depressive disorder: an 8-week, multicenter, randomized, placebo-controlled trial. J Clin Psychiatry. May 1 2010;71(5):616-626.
Zajecka J, Schatzberg A, Stahl S, Shah A, Caputo A, Post A. Efficacy and safety of agomelatine in the treatment of major depressive disorder: a multicenter, randomized, double-blind, placebo-controlled trial. J Clin Psychopharmacol. Apr 1 2010;30(2):135-144.
Montgomery SA, Kasper S. Severe depression and antidepressants: focus on a pooled analysis of placebo-controlled studies on agomelatine. Int Clin Psychopharmacol. Sep 1 2007;22(5):283-291.
Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. Feb 1 1996;17(1):1-12.
Falissard B, Lukasiewicz M, Corruble E. The MDP75: a new approach in the determination of the minimal clinically meaningful difference in a scale or a questionnaire. Journal of clinical epidemiology. Jul 2003;56(7):618-621.
Howland RH. Critical appraisal and update on the clinical utility of agomelatine, a melatonergic agonist, for the treatment of major depressive disease in adults. Neuropsychiatr Dis Treat. Jan 1 2009;5:563-576.
Detke MJ, Lu Y, Goldstein DJ, McNamara RK, Demitrack MA. Duloxetine 60 mg once daily dosing versus placebo in the acute treatment of major depression. Journal of psychiatric research. Nov-Dec 2002;36(6):383-390.
Brannan SK, Mallinckrodt CH, Brown EB, Wohlreich MM, Watkin JG, Schatzberg AF. Duloxetine 60 mg once-daily in the treatment of painful physical symptoms in patients with major depressive disorder. Journal of psychiatric research. Jan 2005;39(1):43-53.
Goldstein DJ, Lu Y, Detke MJ, Wiltse C, Mallinckrodt C, Demitrack MA. Duloxetine in the treatment of depression: a double-blind placebo-controlled comparison with paroxetine. J Clin Psychopharmacol. Aug 2004;24(4):389-399.
Goldstein DJ, Mallinckrodt C, Lu Y, Demitrack MA. Duloxetine in the treatment of major depressive disorder: a double-blind clinical trial. J Clin Psychiatry. Mar 2002;63(3):225-231.
Lieberman DZ, Montgomery SA, Tourian KA, et al. A pooled analysis of two placebo-controlled trials of desvenlafaxine in major depressive disorder. Int Clin Psychopharmacol. Jul 2008;23(4):188-197.
Patient Name______________________________________Date______________________________ Medical Physician’s Name & Phone___________________________________________________________ Please answer the following health questions as completely as possible (circle YES or NO) 1. Do you consider yourself to be in good health? 2. Are you now or have you been under a physicians care within the
Era um edifício de tijolo vermelho impecável na Rua Nove, perto da minha casa, pelo qual tinha passado muitas vezes sem reparar. Escadas de pedra e uma luz quente e confortável no interior. No passeio, uma senhora passeava o cão, um Boston terrier preto e de olhos esbugalhados. Sorriu-me. Interroguei -me se de alguma maneira ela sabia que eu era uma alma em difi culdades. O meu problema rece
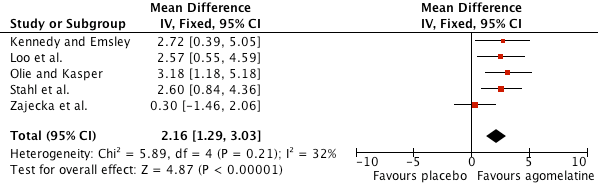
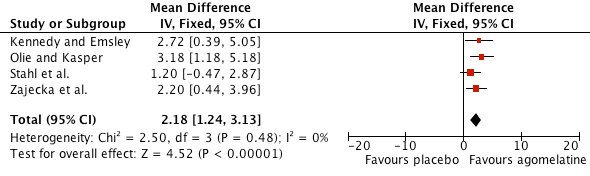 Figure 1. Forest plot of trials evaluating agomelatine 25 mg versus placebo. Outcome reported as difference in mean change HAM-D scores with 95% confidence intervals.
Figure 2. Forest plot of trials evaluating agomelatine 50 mg versus placebo. Outcome reported as difference in mean change HAM-D scores with 95% confidence intervals.
Figure 1. Forest plot of trials evaluating agomelatine 25 mg versus placebo. Outcome reported as difference in mean change HAM-D scores with 95% confidence intervals.
Figure 2. Forest plot of trials evaluating agomelatine 50 mg versus placebo. Outcome reported as difference in mean change HAM-D scores with 95% confidence intervals.