Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
04-incremental prognostic value of (25-31):01- gender association.qxd.qxd
ORIGINAL ARTICLE INCREMENTAL PROGNOSTIC VALUE OF GATED SPECT MYOCARDIAL PERFUSION SCANS WITH DIPYRIDAMOLE STRESS IN PATIENTS WITH LEFT BUNDLE BRANCH BLOCK NOSHEEN FATIMA 1-2, MASEEH UZ ZAMAN 1,3, SYED ZAHED RASHEED 1, M ISHAQ 1, REHAN OMAR 1,SHOAIB Y ALI 1, DAD J BALCOH 1, JAVERIA BANO 1, ASIF WALI 1, KAWISH REHMAN 1,2Objective: Gated single photon emission computerized significantly lower in Group A (42 ±16) than Group B tomography (GSPECT) myocardial perfusion imaging (58 ±8) with significantly higher end diastolic and end (MPI) has well validated incremental prognostic value. systolic volumes (EDV, ESV) in Group A. At 18-24 The aim of this study was to find out the prognostic months follow up, 09 (4.3%) non-fatal events were value of abnormal dipyriodamole GSPECT MPI in reported in Group B while in Group A it was 04 (2.9%, patients with left bundle branch block (LBBB). non-significant p values). Total 8 (5.90%) fatal MIs were reported, all in Group A and none in Group B Methods: This was a prospective study conducted at (significant p values). Kaplan Meier survival plot for Nuclear Cardiology Department of Karachi Institute of non-fatal MI shows a similar event free survival in both Heart Diseases (KIHD), Karachi from August 2010 till groups with a Log Rank value 0.217 (non-significant February 2011. Total 345 patients (135 with LBBB p value) [Figure 2]. Kaplan Meier survival plot for fatal comprised Group A and 210 without LBBB comprised MI show significantly low event free survival for Group B) with adequate dipyridamole GSPECT MPI patients with LBBB (Group A) with a Log Rank value were included. These patients were followed-up for 18- 10.552 (significant p value). 24 months (mean 20 ±3 months) for fatal or non-fatal infarctions (MI). Conclusions: We conclude that dipyridamole GSPECT MPI provides important prognostic information in Results: GSPECT scans were positive for abnormal in patients with LBBB. LBBB group had lower LVEF 47/135 (35%) in Group A and in 90/210 (43%) in which was a strong predictor of cardiac deaths while Group B patients (non-significant p values). However, perfusion parameters were predictors of non-fatal MIs fixed perfusion defects were significantly higher in in patients with or without LBBB. Group A (27%) than Group B (15%) while reversible defects were significantly higher in Group B (28%) Key words: Gated SPECT, LBBB, Prognostic value, than Group A (08%). Similarly incidence of transient dipyridamole, fatal myocardial infarctions ischemic dilatation (TID) was significantly higher in Group B (16%) than Group A (02%). Mean sum stress score (SSS) was higher in Group A (6 ±5) while mean sum difference score (SDS) was higher in Group B (4 PJC 2012; 23: 25-31 ±2). Left ventricular ejection fraction (LVEF) was
1. Nuclear Cardiology Department of Karachi Institute of Heart
INTRODUCTION
2. Karachi Institute of Radiotherapy and Nuclear Medicine
The incidence of left bundle branch block
3. Department of Radiology, The Aga Khan University Hospital
(LBBB) in general population is low (0.6%) but
almost 1/3rd of patients with chronic heart failure
Address for Correspondence:
do have this abnormality.1 Presence of LBBB
Dr. Maseeh uz Zaman Associate Professor and Section Head Nuclear Medicine,
poses a challenge for diagnosis of ischemia due to
Department of Radiology, AKUH, Karachi.
presence of baseline ST-T changes which makes
electrocardiogram (ECG) non-diagnostic at rest
perfusion defects on stress images with or without
and even during treadmill test.2-3 Non-ischemic
transient ischemic dilatation (TID) visually,
abnormal left ventricular ejection fraction (EF <
cardiomyopathy, hypertensive heart disease, aortic
50%), abnormal wall motion, sum stress score
valve disease and fibrosis of conduction fibers.4
[SSS], sum rest score [SRS] and sum difference
Studies have shown that a higher incidence of
score [SD] all >2. All patients/families were
coronary artery disease (CAD) in patients with
interviewed on telephone (18-24 months follow
LBBB5 and 3-4 fold increased in mortality in
up, mean 20 ±3 months) regarding MACE like
patients with known CAD.6 Myocardial perfusion
fatal myocardial infarction (MI) and non-fatal
imaging (MPI) is a non-invasive imaging used for
diagnosis and follow up of patients with CAD with
good sensitivity but low specificity. This lowspecificity is caused by false positive septal
Study Population: Study included 345
defects7 and specificity can be improved by using
consecutive patients who were referred for
vasodilators and gating.8 Gated single photon
dipyridamole GSPECT MPI either for evaluation
emission computerized tomography (GSPECT)
of chest pain or risk factor assessment. Out of
allows assessment of myocardial perfusion and
these, 135 patients had LBBB on resting ECG
(Group A) and 210 patients without LBBB (Group
diagnostic and prognostic strength for patients
B). In Group A, mean age of the cohort was 58 ±
with CAD9. However, data is limited about the
9 years with a male: female ratio of 77: 58 (57%:
prognostic value of pharmacological (vasodilator)
43%). Risk factor assessment in Group A revealed
GSPECT in patients with LBBB with suspected
that 93 (69%) were hypertensive, 49 (36%) were
diabetic, 32 (24%) were dyslipidemic, 24 (18%)were smoker and positive family history for CAD
The aim of this study was to find out the
was found in 39 (29%) [Table1]. In Group B,
prognostic value of abnormal dipyridamole
mean age of the cohort was 56 ± 12 years with a
male: female ratio of 126: 84 (60%: 40%). Riskfactor assessment in Group B revealed that 137
(65%) were hypertensive, 85 (40%) were diabetic,55 (26%) were dyslipidemic, 24 (11%) were
Study Design, Site and Duration: This was
smoker and positive family history for CAD was
found in 80 (38%) [all with non-significant p
Cardiology Department of Karachi Institute of
Heart Diseases (KIHD), Karachi, Pakistan fromAugust 2010 till February 2011. It was duly
Acquisition Protocol: All patients underwent
approved by the ethical committee of the institute.
same day (rest-stress or stress-rest) myocardial
We recruited 135 consecutive patients with LBBB
Methoxy IsoButyl Isonitrile (MIBI). 10-15 mCi
dipyridamole GSPECT scan for evaluation of
of Tc-99m MIBI was administered intravenously
known or suspected CAD. We also selected a
for first study (rest in rest-stress or stress in stress-
control group of 210 patients without LBBB
rest protocol) and 25-30 mCi for second study
(stress in rest-stress or rest in stress-rest protocol).
dipyridamole GSPECT. A positive GSPECT (with
adequate dipyridamole intervention, i.e. increase
acquisitions were performed using dedicated dual
in pulse rate ≥10/min or drop of systolic BP ≥10
head cardiac (Cardio MD, Philips) gamma camera
mmHg from baseline) was defined as presence of
with low energy all purpose (LEAP) collimator,
32 projections around a 180 degree arc, a 64 x 64
study. A rise in ≥10 beats/minute (from baseline)
matrix and 16 frames per cardiac cycle. Image
or drop of ≥10 mmHg of systolic blood pressure
reconstruction and LV functional parameters (EF,
with or without symptoms or ST changes were
considered as adequate response to dipyridamole.
contemplated by using commercially available
Astonish® and Autoquan® software packages
dipyridamole infusion. Intravenous aminophylline
respectively. An EF ≥ 50%, ESV ≤ 70 ml and WM
(75-125 mg) was given to all patient 2-3 minutes
score of zero (in a 17 segment model) were
after radiotracer to antagonize the effect of
considered normal. Similarly, GMPI with SSS,
SRS and SDS <2 were considered as normal.
Statistical Analysis: Comparisons between Stress Protocol: Dipyridamole intervention
patient groups were performed using student-t test
was performed intravenously at a rate of 0.567
for continuous variables and the X2 test for
mg/kg for 4 minute in all patients. Tea, coffee and
categorical variables. Continuous variables were
xanthine derivatives were stopped 24 prior to
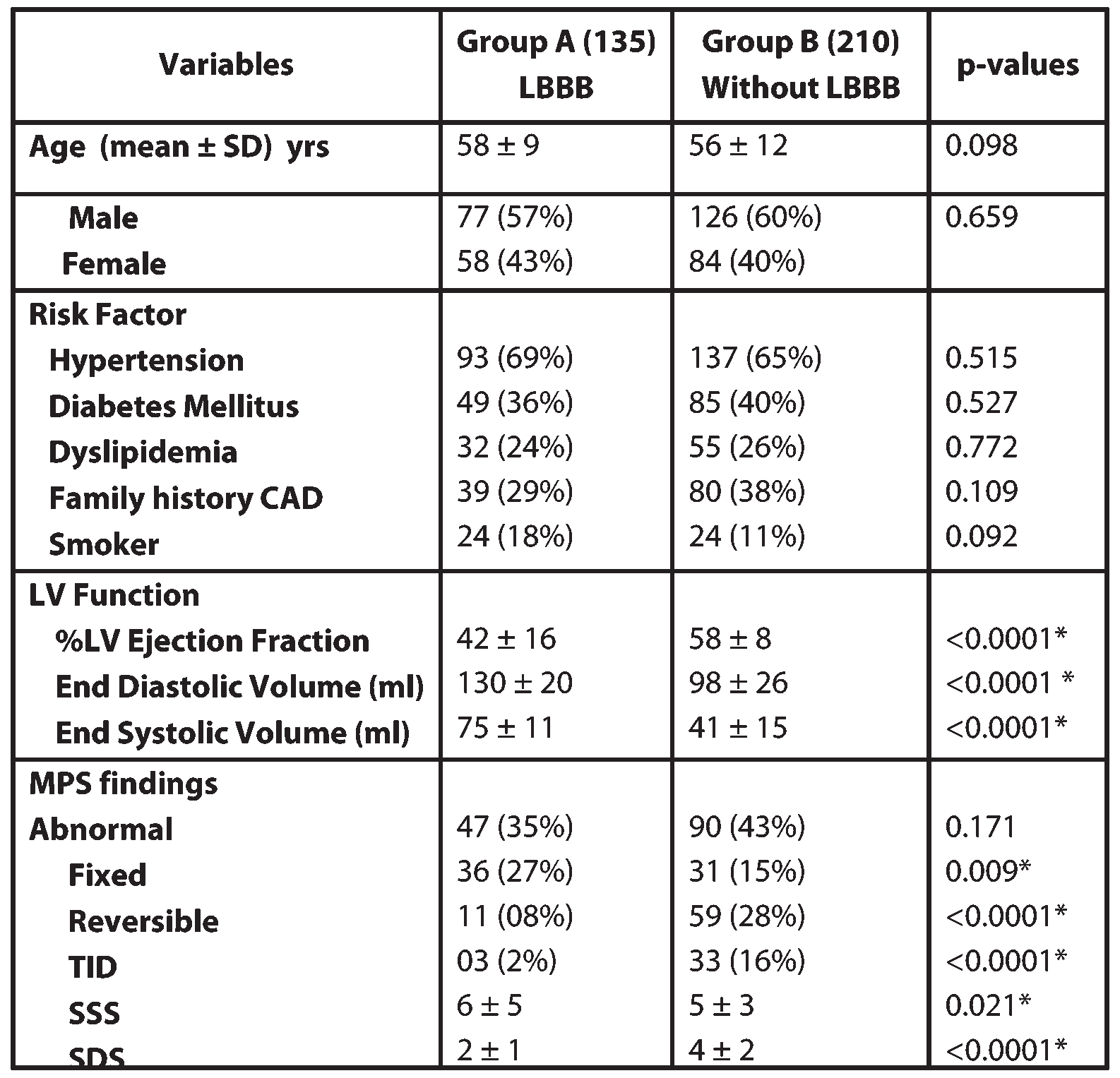
described by mean ± standard deviation (SD). Table-1: Demographic comparison of both groups (Group A=with LBBB, Group; B=without LBBB)
*p<0.05SD= Standard DeviationMPS=Myocardial Perfusion ImagingTID=Transient Ischemic DilatationSSS=Sum Stress ScoreSDS=Sum Difference Score
Figure-1: Comparative fatal and non-fatal events among both groups Figure-2: Kaplan Meier Survival Plot for Non-Fatal Myocardial Infraction among both groups (Group A=LBBB; Group
B=without LBBB) in 18-24 months follow up.
Kaplan-Meier cumulative survival analysis for
compared by the Logrank test. Statistical
major cardiac events like fatal and non-fatal MI
significance was defined as P<0.001.
Figure-3: Kaplan Meier Survival Plot for Fatal Myocardial Infraction among both groups (Group A=LBBB; Group
B=without LBBB) in 18-24 months follow up
significantly higher end diastolic and end systolicvolumes (EDV, ESV) in Group A (Table 1).
perfusion findings in 47/135 (35%) in Group A
At 18-24 months follow up, 09 (4.3%) non-
and in 90/210 (43%) in Group B patients (non-
fatal events were reported in Group B while in
significant p values). However, fixed perfusion
Group A it was 04 (2.9%). These non-fatal events
defects were significantly higher in Group A
included hospital admissions with chest pain
(27%) than Group B (15%) while reversible
culminated in revascularization 07 patients (05 in
defects were significantly higher in Group B
Group B and 02 in Group A). Total 8 (5.90%) fatal
(28%) than Group A (08%). Similarly incidence
MI were reported in the studied population (all in
of TID was significantly higher in Group B (16%)
Group A and none in Group B) [Figure 1). Kaplan
than Group A (02%). Mean SSS was higher in
Meier survival plot for non-fatal MI show a similar
Group A (6 ±5) indicting extent of CAD while
event free survival in both groups with a Log Rank
mean SDS was higher in Group B (4 ±2) which
value 0.217 (non-significant p value) [Figure 2].
shows higher ischemia burden in patients without
Kaplan Meier survival plot for fatal MI show
LBBB (Group B). Left ventricular function
significantly low event free survival for in patients
parameters like LVEF (%) was significantly lower
with LBBB (Group A) with a Log Rank value
in Group A (42 ±16) than Group B (58 ±8) with
10.552 (significant p value) [Figure 3]. DISCUSSION
statistically non-significant) non-fatal events inGroup B. These data are in accordance with a large
Gated SPECT with perfusion and functional
published trial by Cedar Senai investigators16
parameters has an established incremental
which revealed LVEF<45% as significant
diagnostic and prognostic value in general
predictor of mortality while LVEF>45% had lower
population; however, data is scarce about its role
mortality rate irrespective of severity perfusion
in LBBB group. In this study abnormal GSPECT
abnormalities on GSPECT. They also found that
scans were non-significantly higher in Group B
perfusion variables are powerful in predicting
than Group A and most likely due to biased
worsening of coronary disease. In our study mean
sampling. In Group A, incidence of fixed perfusion
SSS and SDS were in mild to moderate range in
defects was significantly higher and this could be
both groups and studies have shown differential
justified due to known anteroseptal defects
risk stratification of lower score for non-fatal
associated with LBBB. Various mechanism have
events and correlation of higher scores with fatal
been proposed for this false positive finding like
impaired diastolic flow to septum due to itsdelayed contraction,10 short diastolic filling at
higher rate11 and decrease baseline and systole
provides important prognostic information in
septal thickness with normal perfusion (partial
LVEF which was a strong predictor of cardiac
dipyridamole stress and gating to avoid it but
deaths while perfusion parameters were predictor
studies have shown that these measures can reduce
of non-fatal MIs in patients with or without LBBB.
but not eliminate the incidence of false positiveresults.13 In this study reversible perfusion
REFERENCES
abnormality was significantly higher in Group B(higher SDS) and also with higher incidence of
TID. These findings are consistent with significant
underlying CAD and this higher incidence could
branch block in ambulant patients withchronic heart failure. European Journal of
In Group A, the mean EF was low with raised
Mahmarian JJ, Verani MS. Detection of left
higher reversible ischemia burden. This is in
anterior descending coronary artery stenosis
accordance with various published studies,14,15 as
in patients with left bundle branch block:
LBBB is often accompanied by LV dilatation even
exercise, adenosine or dobutamine imaging?
in absence of CAD and plausible mechanism is
ventricular asynchrony which in long run leads to
3. Stark KS, Krucoff MW, Schryver B, Kent
remodeling and dilatation4. Another important
aspect of this study is significantly higher fatal MI
during coronary angioplasty in patients with
in Group A and non-significant incidence of non-
left-bundle-branch block. Am J Cardiol.
fatal events in both groups. If we closely observe
the data than we come to realize that LVEF wasthe predictor of higher mortality in LBBB group
while perfusion parameter like SDS was the
Saladini F, Razzolini R, Evangelist L. Risk
predictor of non-fatal events in both groups. The
stratification and prognostic assessment bymyocardial perfusion-gated SPECT in
SDS was significantly higher in Group B and that
patients with left bundle-branch block and
low-intermediate cardiac risk. Ann Nucl Med
12. Afzal MS, Imran MB, Aslam N, Khurshid
5. Schneider JF, Thomas HE Jr, Sorlie P, Kreger
identifying septal perfusion artifacts in left
Comparative features of newly acquired left
bundle branch block. J Coll Physicians Surg
and right bundle branch block in the general
population: the Framingham Study. Am JCardiol 1981; 47: 931–40
13. Matzer L, Kiat H, Friedman JD Van Train K,
6. Eriksson P, Wilhelmsen L, Rosengren A.
the assessment of tomographic thallium-201
scintigraphy in patients with left bundle
Goteborg. Sweden. Eur Heart J 2005;26:2300–6
14. Bavelaar-Croon CDL, Wahba F, Van Hecke
7. Fahy GJ, Pinski SL, Miller DP, McCabe N,
Pye C, Walsh MJ, et al. Natural history of
abnormalities outside the septal region in
isolated bundle branch block. Am J Cardiol
assessed with gated SPECT. Q J Nucl Med2001;45:108–14
8. Higgins JP, Williams G, Nagel JS, Higgins
Krawczynska E, Cooke CD, Faber TL, et al.
tomography with technetium Tc 99 M (Tc-99
assessment of left ventricular function from
decrease false-positive interpretations. Am
9. Evangelista L, Nai Fovino L, Saladini F,
16. Sharir T, Germano G, Kavanagh PB, Lai S,
Saladini G, Razzolini R, Mormino GP, et al.
Cohen I, Lewin HC. Incremental Prognostic
myocardial perfusion single-photon emission
17. Hachamovitch R, Berman DS, Shaw LJ, et
abnormalities in isolated left-bundle branch-
myocardial perfusion single photon emission
computed tomography for the prediction of
asynchrony. Circulation 1989; 79:845–53
cardiac death: differential stratification forrisk of cardiac death and myocardial
11. Ono SJ, Nohara R, Kambara H, Okuda K,
infarction. Circulation 1998;97:535–43.
Kawai C. Regional myocardial perfusion andglucose-metabolism in experimental left-bundle-branch block. Circulation 1992;85:1125–31
Chinese Kruidengeneeskunde Westers gezien bestond er in de middeleeuwen wel verband tussen de diverse toegediende kruiden. Erwas sprake van een traditioneel systeem wat echter door de inquisitie en de westerse wetenschap werduitgebannen.Nu bestaat de westerse kruidengeneeskunde uit een grote hoeveelheid kruiden zonderverband, dit pilletje hiervoor en dat pilletje daarvoor. Hetzelfde beeld ontwi
Price List Membership Fees Doctor Consultation Fees Joining Fees Telephone (15 mins, including out of hours) VIP12 Home Visit (during surgery hours)# 5th & subsequent members of a household Medical Procedures VIP 12 membership (excludes Nurse/Doctor fee unless stated) Non-Members Cervical Smear–Non-member (inc Nurse fee) £112.50 VIP 24 membership V
 32 projections around a 180 degree arc, a 64 x 64
study. A rise in ≥10 beats/minute (from baseline)
matrix and 16 frames per cardiac cycle. Image
or drop of ≥10 mmHg of systolic blood pressure
reconstruction and LV functional parameters (EF,
with or without symptoms or ST changes were
considered as adequate response to dipyridamole.
32 projections around a 180 degree arc, a 64 x 64
study. A rise in ≥10 beats/minute (from baseline)
matrix and 16 frames per cardiac cycle. Image
or drop of ≥10 mmHg of systolic blood pressure
reconstruction and LV functional parameters (EF,
with or without symptoms or ST changes were
considered as adequate response to dipyridamole.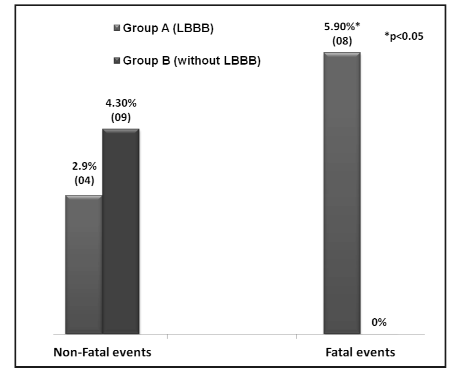
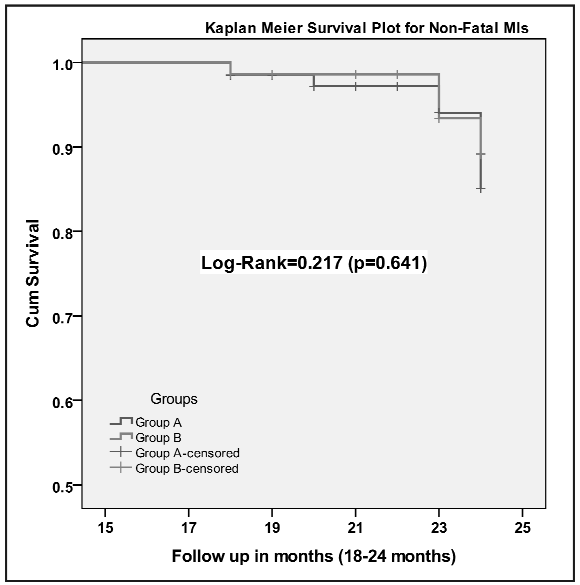 Figure-1: Comparative fatal and non-fatal events among both groups
Figure-1: Comparative fatal and non-fatal events among both groups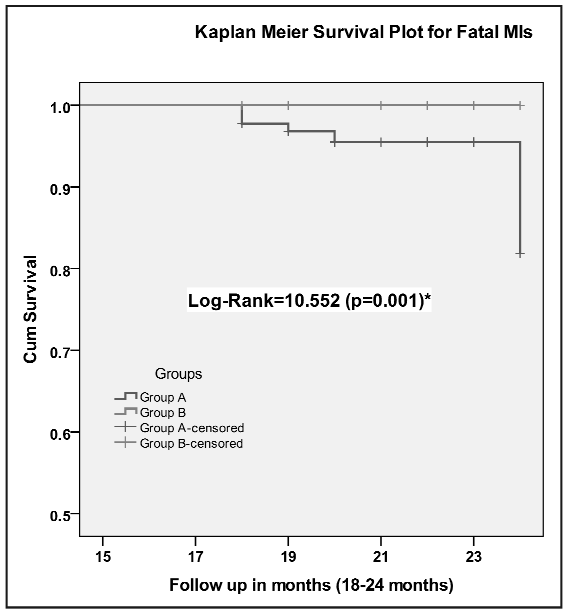 Figure-3: Kaplan Meier Survival Plot for Fatal Myocardial Infraction among both groups (Group A=LBBB; Group
B=without LBBB) in 18-24 months follow up
significantly higher end diastolic and end systolicvolumes (EDV, ESV) in Group A (Table 1).
perfusion findings in 47/135 (35%) in Group A
At 18-24 months follow up, 09 (4.3%) non-
and in 90/210 (43%) in Group B patients (non-
fatal events were reported in Group B while in
significant p values). However, fixed perfusion
Group A it was 04 (2.9%). These non-fatal events
defects were significantly higher in Group A
included hospital admissions with chest pain
(27%) than Group B (15%) while reversible
culminated in revascularization 07 patients (05 in
defects were significantly higher in Group B
Group B and 02 in Group A). Total 8 (5.90%) fatal
(28%) than Group A (08%). Similarly incidence
MI were reported in the studied population (all in
of TID was significantly higher in Group B (16%)
Group A and none in Group B) [Figure 1). Kaplan
than Group A (02%). Mean SSS was higher in
Meier survival plot for non-fatal MI show a similar
Group A (6 ±5) indicting extent of CAD while
event free survival in both groups with a Log Rank
mean SDS was higher in Group B (4 ±2) which
value 0.217 (non-significant p value) [Figure 2].
Figure-3: Kaplan Meier Survival Plot for Fatal Myocardial Infraction among both groups (Group A=LBBB; Group
B=without LBBB) in 18-24 months follow up
significantly higher end diastolic and end systolicvolumes (EDV, ESV) in Group A (Table 1).
perfusion findings in 47/135 (35%) in Group A
At 18-24 months follow up, 09 (4.3%) non-
and in 90/210 (43%) in Group B patients (non-
fatal events were reported in Group B while in
significant p values). However, fixed perfusion
Group A it was 04 (2.9%). These non-fatal events
defects were significantly higher in Group A
included hospital admissions with chest pain
(27%) than Group B (15%) while reversible
culminated in revascularization 07 patients (05 in
defects were significantly higher in Group B
Group B and 02 in Group A). Total 8 (5.90%) fatal
(28%) than Group A (08%). Similarly incidence
MI were reported in the studied population (all in
of TID was significantly higher in Group B (16%)
Group A and none in Group B) [Figure 1). Kaplan
than Group A (02%). Mean SSS was higher in
Meier survival plot for non-fatal MI show a similar
Group A (6 ±5) indicting extent of CAD while
event free survival in both groups with a Log Rank
mean SDS was higher in Group B (4 ±2) which
value 0.217 (non-significant p value) [Figure 2].