Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Ijp_dec_04.pmd
Comparison of the clinical efficacy of three brands of warfarin
M. H. Namazi, Z. K. Yousefi, M. G. Shirazi, M. Shaykholeslami, H. Vakili, M. R. Moatamedi, M. Safi,
Objective: To compare the clinical efficacy of three brands of warfarin. Material and Methods: Thirty-six patients (mean age 51.8±12.7 years, 12 males, 24 females) withdifferent indications for anticoagulant therapy were randomly placed in 3 groups. Each groupstarted with one of the three brands of warfarin (Orion from Finland=Brand A, Cipla from India=Brand
B and Ferrer from Spain=Brand C) and crossed over to another after 4 weeks. Patients were fol-
lowed up at weekly visits, checking prothrombin time (PT), International Normalized Ratio (INR)
and any complications. The cardiologist and patients were unaware of the warfarin brand used.
Number of dose changes, mean dose changes (mg), target INR achievement in the last week and
the mean stable dose (mg) were compared between the three brands. Results: Mean number of dose changes throughout the 4-week course was 1.6±1.2 times for brand
A, 1.2±1.1 times for brand B and 1.3±0.9 times for brand C (P=0.24). The amount of total dose
changes was similar (0.70±0.6 mg for brand A, 0.63±0.9 mg for brand B and 0.72±0.8 mg for
brand C, P=0.89). The rate of target INR achievement in the last week was similar (46.9% for brand
A, 50% for brand B and 50% for brand C). Thirty-four per cent of patients treated with brand A,
28% with brand B, and 32% with brand C did not achieve target INR. The required dose for the
stable target INR was 4.6±2.2 mg, 5.3±2.2 mg and 5.3±2.4 mg in patients treated with brands A, Band C respectively (P=0.61). There were no complications except 2 cases of drug discontinuationby the physician for extreme overdose, (i.e. INR>4.5 that needed drug discontinuation). Conclusion: Orion, Cipla and Ferrer warfarin products were similar regarding target INR achieve-ment, the required dose and number of dose changes.
KEY WORDS: INR, oral anticoagulant, prothrombin time
Introduction
comparable to the brand Coumadin in its effectiveness,ability to maintain stable anticoagulation, and safety.5-7 When
Warfarin is a common anticoagulant which is used in a
initiating anticoagulant therapy or when converting patients
variety of clinical settings. The drug is vital to many patients
from the brand Coumadin to generic warfarin, additional
at increased risk of thromboembolic complications, and is of-
monitoring of the International Normalized Ratio (INR) may
ten prescribed for patients with artificial heart valves,
be needed. In 1980, conversion from DuPont crystalline
arrhythmias or other conditions that increase the risk of co-
warfarin to an amorphous warfarin caused an increase in
agulation. Studies have shown the beneficial effects of warfa-
the number of patients whose anticoagulation was poorly
rin administration in the prevention of stroke in patients with
In Iran, generic warfarin is mainly supplied by Orion Cor-
Different formulations and brands of warfarin are avail-
poration (Orion Pharmaceutica, Espoo, Finland). The process
able. Warfarin sodium has been added to the formulary as
of import and distribution of this product, for various reasons,
the generic alternative to the brand Coumadin, which is the
is not constant and reliable, imposing serious risks due to
eleventh most prescribed medication in the United States.3
unwanted drug discontinuation or dose change. Therefore, we
The Food and Drugs Administration of USA (FDA) has
designed this study to compare the efficacy and side-effects
granted some products of generic warfarin an “AB” rating,
of Orion warfarin with two other brands, in order to devise
indicating a therapeutic equivalence to the brand Coumadin.4
recommendations for the replacement of Orion warfarin with
Clinical trials have demonstrated that generic warfarin is
Indian J Pharmacol | December 2004 | Vol 36 | Issue 6 | 360-362
Material and Methods
P=0.89). Table 1 shows the amount of dose change in eachvisit and the total dose change for each brand.
This was a randomized double-blind crossover clinical trial.
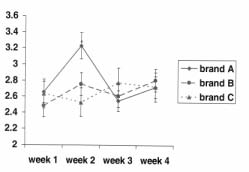
Figure 1 compares mean INR values in each week for the
The patients were those visiting Modarres Hospital heart clinic,
three brands. Except a sharp and statistically significant in-
or those hospitalized in Modarres Hospital, who had indica-
crease in INR at the second visit for brand A, the differences
tions for anticoagulation therapy. All patients had optimal In-
between mean INR for the brands in each visit were insignifi-
ternational Normalized Ratio (INR), i.e. 2-3 for atrial fibrilla-
cant. Target INR was defined for each patient according to
tion and 2.5-3.5 for valvular heart disease. Patients were ex-
his/her disease. Patients receiving the three brands achieved
cluded if they did not receive warfarin, could not come to the
the target INR at the same rate (46.9% for brand A, 50% for
hospital for weekly visits or did not cooperate, or had dis-
brand B and 50% for brand C). Thirty-four per cent of patients
eases interfering with warfarin metabolism. Also, patients on
treated with brand A, 28% of patients treated with brand B,
drugs interacting with warfarin such as phenytoin, phenobar-
and 32% of patients treated with brand C did not achieve tar-
bital, cimetidine and amiodarone were excluded. An appropri-
get INR. Over-treatment, i.e. INR>upper limit of target range,
ate review committee approved the study protocol.
was seen in 19%, 22% and 18% of patients treated with brand
Patients were briefed on the study protocol and objectives
A, brand B and brand C respectively (P=0.98). The required
and then, were asked to sign an informed consent if they were
dose for the stable target INR was 4.6±2.2 mg, 5.3±2.2 mg
willing to participate. The sample size was calculated based
and 5.3±2.4 mg in patients treated with brand A, B and C
on mean necessary dose change in groups assuming al-
respectively (P=0.61). There were no complications except 2
pha=0.05, beta=0.2, SD=0.7 and a difference of 0.5. So 36
cases of drug discontinuation by the physician for extreme
patients were randomly allocated into one of the three treat-
overdose. No major hemorrhagic or thromboembolic events
ment groups. Each group received one of the study drugs: A
(Orion warfarin 5 mg tablets, Orion Pharmaceutica, Espoo,Finland), B (Warf5, CIPLA, Mumbai, India) and C (Warfarin 5
Discussion
mg tablets, Ferrer, Spain). The formulations were identical inshape and size. The patients and the attending physicians were
The results of this study demonstrated similar effects of
the three brands of equal strength (5 mg) oral warfarin (Orion,
Each group received the prescribed drug for four weeks.
Cipla and Ferrer). This similarity was demonstrated through
During this period, they were visited weekly. In these weeklyvisits, prothrombin (PT) and INR were checked and the pa-tients were asked about the possible complications. The at-
tending cardiologist recorded the data and decided whether a
The total amount of dose change and dose change (mg) in each
dose adjustment was necessary. Target INR was defined ac-
visit for the three brands
cording to the indication: 2-3 for atrial fibrillation or 2.5-3.5for valvular heart disease and prosthetic valves. After four
weeks the patients were switched to the next drug (e.g. A to B)
and the same method was used. The patients were once more
switched to the next drug, till all completed the 12-week dura-
tion and had used all the three brands in the course. Blood
samples were centrifuged for 5 min and after plasma separa-
tion at 37° C, 0.2 ml thromboplastin and 0.1 ml plasma were
added to measure PT. Biomerieux table was used to deter-mine INR.
Data are presented as percentage and mean+SD. Repeated
measures ANOVA was used to assess the differences amongthe three brands used. A P value less than 0.05 was consid-ered significant.
The mean age of patients was 51.8±12.7 years. Their av-
erage weight was 64.4±14.0 kg. Twenty-four patients werefemale. Patients received warfarin for the following diagnoses:Valvular heart disease (44.4%), atrial fibrillation (50%), andother conditions (5.6%).
The mean number of dose changes throughout the 4-week
courses was 1.6±1.2 times for brand A, 1.2±1.1 times forbrand B and 1.3±0.9 times for brand C (P=0.24). The amount
*P<0.05 compared with other brands and other visits
of total dose changes was similar (0.70±0.6 mg for brand A,0.63±0.9 mg for brand B and 0.72±0.8 mg for brand C,
Figure 1: Mean INR for different brands of warfarin
Indian J Pharmacol | December 2004 | Vol 36 | Issue 6 | 360-362
the rate of achievement of target INR and number and amount
In another cohort study, Milligan and associates10 deter-
of dose changes. Other studies have examined the effect of
mined whether a Health Maintenance Organization (HMO) can
switching from one type of warfarin to another. Such studies
add generic warfarin to its formulary without adversely af-
focus mainly the switch from coumadin to generic warfarin.
fecting warfarin management or increasing adverse events.
Most of them have also shown that such a switch is usually
Data were collected 8 months prior to and 10 months after
harmless and does not have serious effects on anticoagula-
the introduction of generic warfarin (Barr Laboratories,
tion. In two randomized crossover clinical trials Neutel and
Pomona, NY) to an HMO’s formulary. In this study the change
Smith5 and Handler et al 6 compared coumadin and generic
did not significantly affect INR control, warfarin management,
warfarin. They treated patients for 21-28 days. In these trials,
or adverse events. Authors suggested that HMOs can safely
the change in the mean baseline INR to overall INR was – 0.10
substitute at least 1 generic formulation of warfarin without
and –0.20 for Barr and – 0.01 and – 0.02 for DuPont products
respectively. Both studies found no significant difference in
In two cases at a family medicine center anticoagulation
the average INR values. There was no difference in the ad-
clinic in Oklahoma city, Hope and Havrda11 reported sub-thera-
verse effects between the two drugs. Both concluded that the
peutic INR values after a switch from Coumadin to generic
two products were equivalent. Swenson7 studied a cohort of
warfarin, while all other variables were kept consistent dem-
patients at a managed-care organization and determined the
onstrating the need for close monitoring of the INR when pa-
safety and effectiveness of switching to generic warfarin. This
tients are switched between brands of warfarin.
study was not blinded and patients seen during routine visits
Although some findings such as Hope and Havrda’s re-
at two anticoagulation clinics were asked to volunteer to use
port11 underscore the importance of close monitoring if a switch
generic warfarin (Barr Laboratories) instead of coumadin for
in warfarin brand is done, most studies show safe switch from
eight weeks. Patients (n = 210) who had therapeutic INR val-
one warfarin brand to another. This is especially important for
ues at the baseline visit and had received anticoagulation with
our patients, since Orion warfarin is not always available. Since
coumadin for three months were enrolled in the study. The
it is very important to maintain a steady and acceptable level
control group (n = 105) consisted of patients who declined or
of anticoagulation over the time for all the patients, it is some-
were not asked to change the drug. Mean INR values were
times necessary to switch to a different brand when the cur-
compared before and after enrollment. The difference between
rent brand is not available. Our results demonstrate that such
the two groups was not significant and of negligible clinical
switching is harmless in patients taking warfarin as a prophy-
meaning. Among the patients who had a dosage change, there
was no significant difference in the variability of the INR be-fore versus after enrollment. Patients in either group did not
References
report any serious complications. The authors concluded thatthe two warfarin sodium products were equivalent in usual
Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrilla-tion. Analysis of pooled data from five randomized controlled trials. Arch Intern
Med 1994;154:1449-57. Erratum in: Arch Intern Med 1994;154:2254.
In one study, Weibert and associates9 compared the dos-
Kalra L, Yu G, Perez I, Lakhani A, Donaldson N. Prospective cohort study to
ing requirements and INRs associated with two bioequivalent
determine if trial efficacy of anticoagulation for stroke prevention in atrial fibril-
crystalline warfarin sodium products in patients with chronic
lation translates into clinical effectiveness. Brit Med J 2000;320:1236-9.
atrial fibrillation. This was a multicenteric, single-blind (pre-
National prescription audit: Physician specialty report, dispensed data. Ply-mouth Meeting, Pa.: America: IMS; 1998.
scriber), randomized, crossover trial of Apothecon warfarin
Electronic Orange Book: Approved drug products with therapeutic equivalence
and DuPont warfarin (coumadin) in adults with chronic or par-
evaluations. Rockville (MD): FDA/Center for Drug Evaluation and Research;
oxysmal atrial fibrillation who had been receiving DuPont war-
farin chronically for the prevention of thromboembolism. Pa-
Neutel JM, Smith DHG. A randomized crossover study to compare the efficacy
tients were randomly assigned to initially either continue
and tolerability of Barr warfarin sodium to the currently available Coumadin®. Cardiovasc Rev Rep 1998;19:49-59.
DuPont warfarin or receive Apothecon warfarin for four weeks,
Handler J, Nguyen TT. A blinded, randomized, crossover study comparing the
with weekly evaluation of dosage and INR changes, safety and
efficacy and safety of generic warfarin sodium to Coumadin®. Prev Cardiol
efficacy. Subsequently, patients crossed over and received the
other product for four weeks. Neither the propensity for a dos-
Swenson CN, Fundak G. Observational cohort study of switching warfarin so-
age change or an INR change nor the magnitude of a dosage
dium products in a managed care organization. Am J Health Syst Pharm
change or INR change appeared related to a particular warfa-
Richton-Hewett S, Foster E, Apstein CS. Medical and economic consequences
rin product (NS for each variable after each study period).
of a blinded oral anticoagulant brand change at a municipal hospital. Arch
After four weeks of treatment, the same number of patients
(n=7) experienced a 20% change in warfarin dosage from the
Weibert RT, Yeager BF, Wittkowsky AK, Bussey HI, Wilson DB, Godwin JE, et
respective baseline with each product. The number of patients
al. A randomized, crossover comparison of warfarin products in the treatment
with INRs outside the desired protocol range after four weeks
of chronic atrial fibrillation. Ann Pharmacother 2000;34:981-8.
10. Milligan PE, Banet GA, Waterman AD, Gatchel SK, Gage BF. Substitution of
of treatment was similar for both groups (<1.8, n = 9 for
generic warfarin for Coumadin in an HMO setting. Ann Pharmacother
both products, or >3.2, n = 9 for DuPont, n=10 for
Apothecon). No major hemorrhagic or thromboembolic events
11. Hope KA, Havrda DE. Subtherapeutic INR values associated with a switch to
generic warfarin. Ann Pharmacother 2001;35:183-7.
Indian J Pharmacol | December 2004 | Vol 36 | Issue 6 | 360-362
Pharmaceuticals – Permanent Pollutants in Environment Basic facts and proposed measures to protect the public health and the environment Prepared for the International Society of Doctors for the Environment by the Swedish Doctors for the Environment (LfM) in June, 2010 Authors Åke Wennmalm, MD, PhD. Former environmental director of Stockholm County Council Bo Gunna
 Material and Methods
Material and Methods