Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Microsoft word - fmw_intake_master.docx
WELCOME TO FULLMOONWATER CHINESE MEDICINE CONTACT INFORMATION
_____________________________________________________________________
__________________________ Preferred Phone: (circle: Home Cell Work)
________________________________________________________________
Do we have your permission to send appointment reminders, health newsletters, and occasional promotions to your email address? Yes _____ No _____ Your email will not be sold or given to any other agency.
Emergency Contact:
If you have health insurance, we will be happy to verify your benefits. If you have a discount plan through your insurance, please let us know.
How did you hear about us? (Please circle) MISSION STATEMENT
FullMoonWater provides information, education, and access to complementary health services for people seeking wellness, FullMoonWater connects practitioners and neighbors to achieve optimum health. Healthy and happy people are the basis of a healthy and happy community.
DISCLAIMER
Merely an office location, through which independent practitioners conduct their business, FullMoonWater does not render any services or provide any care or treatment. The individual practitioner that performs the services is independent from FullMoonWater and is responsible for the services rendered. Additionally, not all of the practitioners at FullMoonWater are licensed medical doctors; some services available at FullMoonWater are complementary to and not a substitution for treatment by a licensed medical doctor. As such, by signing below, you indicate that you understand this disclaimer and agree to hold FullMoonWater harmless from any and all claims related to services obtained at FullMoonWater.
Signature:
____________________________________ Date: _______________ COLORADO MANDATORY DISCLOSURE STATEMENT Troy Krebs, L.Ac.
Troy Krebs received her degree at the Colorado School for Traditional Chinese Medicine (a credentialed 36-month program). She was trained in the recommendation and application of adjunctive therapies and herbs as defined by traditional Oriental medicine concepts. She also studied 5-element acupuncture. She studied Chinese medicine in China to earn additional experience. Troy is certified by the National Certification Commission for Acupuncture and Oriental Medicine (NCCAOM). She is licensed to practice acupuncture in the state of Colorado and has been practicing acupuncture since 2002. She has privileges at Craig Hospital. Troy has not had any license, registration, or certification revoked or suspended.
This office complies with all rules and regulations promulgated by the Colorado Department of Health, including the proper cleaning and sterilization of needles and the sanitation of acupuncture offices. Only single-use, disposable, factory-sterilized needles are utilized; and they are disposed of in a manner consistent with OSHA and Colorado State regulations.
Cash at Time of Service Fee Schedule
Initial Acupuncture Evaluation and Treatment
Coupons or other special discounts may apply
Insurance is billed by code; payment varies by plan
Patient's Rights
Each patient who visits this office is entitled to receive information about the methods of therapy, the techniques used, and an estimated duration of therapy, if known. The patient may seek a second opinion from another healthcare professional or may terminate therapy at any time. In a professional relationship, sexual intimacy is never appropriate and should be reported to the Director of the Division of Registrations in the Department of Regulatory Agencies. The Colorado Department of Regulatory Agencies regulates the practice of acupuncture. If you have comments, questions, or complaints, contact the Acupuncturists Registration Office, 1560 Broadway, Suite 1350, Denver, Colorado 80202. Telephone: 303 894-7800. I have read and understand the above disclosure statement. I understand my rights and responsibilities as a patient.
Patient's Name (Please print): ________________________________________________
_____________________________________________ _____________________ Signature of patient or legal guardian FINANCIAL POLICY FOR PATIENT CARE SERVICES
FullMoonWater wants to provide the most efficient and affordable health care services, so it is necessary for us to have a financial policy stating our requirements for timely payment of services and products provided by our office. We welcome the opportunity to discuss any aspect of our financial policy.
1) Provide us with accurate and updated information on yourself and your insurance company. 2) Pay at the time of service for your entire balance. 3) Discuss your account balance only with the front office staff. It is important for practitioners
to be allowed to provide patient care. If the front office staff cannot help you, do not hesitate to contact the office manager.
Insurance Patients: We are happy to file for insurance as a courtesy to you. As stated by your insurance company: "Verification of benefits is no guarantee of payment." If you have insurance and we file with your carrier for you, you will be responsible for all charges not paid by the insurance company. The balance due is your responsibility if we have not received payment from your insurance company within 60 days.
FullMoonWater sends claims with procedure codes to the insurance companies. Your insurance company then chooses the "reasonable and customary" amount to apply to your visit. Your insurance plan is a contract between you and your insurance company, therefore any amount applied toward your deductible must be paid in full.
1) You are authorizing FullMoonWater, its providers, and its employees to release any
necessary information related to this visit and all future visits to your insurance company for the purpose of claim(s) payment.
2) You are authorizing your insurance company and your medical provider to release your
medical records to FullMoonWater for the purpose of claim(s) payment.
3) You are authorizing your insurance company to pay any medical benefits and all future
claims for services provided by our office directly to FullMoonWater.
4) You are giving FullMoonWater the right to speak with your insurance company, any third
party insurance company, and your attorney regarding your claims and bills.
5) You agree that a photocopy of any document is as valid and effective as the original.
FullMoonWater and its providers accept worker's compensation and auto accident insurance. We require that a lien signed by the patient and any attorneys is on file when applicable. FullMoonWater and its providers are willing to extend the expectation of payment within 60 days for worker's compensation and auto accident insurance when Med-Pay is not available.
If you prefer that we do not file insurance claims for you, you may pay the cash at time of service discounted rate and send the claim to your insurance carrier. If you choose to submit your own claims, we will provide you with a superbill, but cannot assist you in filing your claims.
FINANCIAL POLICY FOR PATIENT CARE SERVICES (CONT) Self-Pay Patients: If you do not have insurance or our services are not covered by your insurance company, you will be considered a "self-pay" patient. Family plans and discounts must be applied at the time of service and cannot be back-dated. If you have a financial hardship, an application for financing or a financial hardship discount must be completed before or at the time of service. It is important to FullMoonWater that you become well now, even if we need to work with your financial budget. Cancellation Policy: In order to provide you with the best care, please arrive 10 minutes prior to your appointment-late arrival may result in cancellation. We require 24 hours' notice of cancellation or you may be charged a fee. Please remember that failure to appear for your appointment prevents others from receiving care. Finance Charges: Failure to pay for services and products provided by our office will result in a finance charge. If we need to forward your account over to a collections agency for further legal action, you will be responsible for the entire balance on your account plus any collection fees. Payment Options: For your convenience, we are happy to keep your credit card on file and secured for payment of all services and products. Cash at Time of Service Rates: Service Healthy People are Happy People
___________________________________________________ Patient's Name (please print)
___________________________________________________ ________________________ Responsible Party or Authorized Person Signature
___________________________________________________ ________________________ FullMoonWater Signature ACUPUNCTURE INFORMED CONSENT
Acupuncture has been explained to me as a treatment consisting of the insertion of needles through the skin at specific points on the surface of the body (small amounts of electrical current may be applied to the needles). The purpose of acupuncture has been explained as the alleviation or cure of symptoms or disorders. Acupuncture, acupressure, Moxa, cupping therapy, allergy elimination technique, nutritional or herbal counseling are considered experimental procedures and are not considered a substitute for Western Medicine. Therapies and advice offered shall not be construed by the client to be a diagnosis of treatment of any disease or injury. We recommend that you CONSULT YOUR PHYSICIAN for any serious conditions and receive at least two medical opinions. It is your right and responsibility for your own body. I understand that complications may result from acupuncture treatment. Among these possible complications are: areas of anesthesia, fainting, weakness, nausea, hematoma, infection, pain and discomfort, Pneumothorax, and aggravation of present symptoms. Being hungry, tired, or stressed can infrequently make the body more sensitive to the acupuncture treatment. Please tell your provider if you have any conditions that may inhibit blood clotting, such as hemophilia or Coumadin use. Please use caution when walking with bare feet in the treatment room. I further understand and agree to hold harmless, to indemnify and to protect against court action the individual therapist as well as the management and owners of this clinic, in the event of accidental injury on these premises.
Payment Practices
FullMoonWater gladly accepts health insurance, automobile insurance, and worker's compensation as payment. Insurance coverage depends upon your individual plan. Please call your insurance company to verify your acupuncture benefits. In the event your insurance does not cover acupuncture, discounted charges will be collected at the time of service.
Payment Agreement
I authorize FullMoonWater to release any information required to process this claim to any insurance company or attorney in this case. I also authorize my insurance company or medical provider to release my medical records to FullMoonWater. This information is to be used for the purpose of processing my claims for benefits due. I hereby agree that a photocopy of the document is as valid and effective as the original. I hereby authorize my insurance benefits to be paid directly to FullMoonWater. I assume full responsibility for and agree to pay all costs, charges, and expenses of every kind and description for services furnished by FullMoonWater. I agree to pay charges and services not covered by any insurance or other third-party payer and/or not paid to FullMoonWater for any reason within a reasonable time (as determined by FullMoonWater). The amount of the bill shall be due and payable upon presentation to the patient, his/her agent, guardian, conservator, or third party responsible for payment of the charges.
Cancellation Notice
Please be considerate of your appointment time. We make every effort to respect your time and see you promptly when you are scheduled. Please call if you cannot make your appointment or you are running late. Patients who consistently miss their appointments or fail to cancel 24 hours in advance may be charged for their missed appointments. I have read and understand the above Informed Consent statement. I agree to the conditions set forth in this statement.
___________________________________________________ Patient's Name (please print)
___________________________________________________ ________________________ Responsible Party or Authorized Person Signature ACUPUNCTURE PRIVACY PRACTICES
As your health care provider, we use your health information for evaluation and treatment; as well as to
obtain payment for treatment. If you are referred to another health care provider, or at your request, your medical records may be shared with those providers. We may use your health care information without your authorization for the following reasons:
4. At the request of your insurance carrier
In all other circumstances, we will ask your written permission to release your medical information in
the form of a "Release of Medical Records" form. If you choose to sign such a form, you have the right to revoke that authorization at any time. If you would like to review our "Notice of Privacy Practices," please request a copy at the front desk. If, at any time, we change our policies regarding your medical information, you will be informed with a new "Privacy Practices" form to sign, as well as a new copy of "Notice of Privacy Practices."
You have the right to view and obtain a copy of your medical record. You also have the right to know
to whom we have disclosed your medical records. If you believe the information in your medical record is not correct or missing information, you have the right to request that such information is corrected or added to your medical record.
If you have any questions or concerns about your medical records, please contact FullMoonWater, or
you can file a written complaint with the U.S. Department of Health and Human Services. FullMoonWater is required by law to protect your medical information and provide this notice to you, along with your signature acknowledging your receipt of this information.
FullMoonWater reserves the right to change the privacy practices that are described in the "Notice of
Privacy Practices." You may obtain a revised "Notice of Privacy Practices" by notifying the office of FullMoonWater and requesting a revised copy. Our office sends thank you cards for referrals, periodic newsletters, and participates in other non-private contact. This may be via email or postal service. Reminders of your appointments may be via email or telephone.
I understand that I have a right to read the "Notice of Privacy Practices" prior to signing this form. The
"Notice of Privacy Practices" describes the types of uses and disclosures of my protected health information that will occur in my treatment, payment of my bills, or in the performance of health care operations at FullMoonWater. This "Notice of Privacy Practices" also describes my rights, as well as the duties of the practitioner with respect to my protected health information.
I consent to the use or disclosure of my protected health information by FullMoonWater for the purpose
of analyzing, diagnosing, or providing treatment; as well as obtaining payment for my health care bills or to conduct health care operations. I understand that analysis and treatment by Acupuncture Associates may be conditioned upon my consent as evidenced by my signature below.
I understand I have the right to request a restriction as to how my protected health information is used
or disclosed to carry out treatment, payment, or healthcare operations of the practice. FullMoonWater is not required to agree to the restrictions that I may request. However, if FullMoonWater agrees to a restriction that I request, the restriction is binding on FullMoonWater. I have the right to revoke this Consent, in writing, at any time, except to the extent that FullMoonWater has taken action in reliance on this Consent.
My "protected health information" means health information, including any demographic information
collected from me and created or received by my physician, another health care provider, a health plan, my employer, or a healthcare clearinghouse. This protected health information relates to my past, present, or future physical or mental health or condition that identifies me, or there is a reasonable basis to believe the information may identify me.
Patient's Name (please print): _____________________________________________________
___________________________________________________ ________________________ Responsible Party or Authorized Person Signature ACUPUNCTURE PATIENT INFORMATION
Please complete this form as thoroughly as possible. Some questions may seem unrelated to your condition, but the answers may affect your diagnosis and treatment. All information is confidential.
First Name ______________________ Last Name ______________________ Date
Date of Birth ________________________ Age __________________
Address ___________________________________________________________________________________
City _____________________________________ State _________ Zip ___________________________
Home Phone ________________ Work Phone _________________ Cell Phone ____________________
Place of Employment ________________________________ Occupation
How did you hear about us? (Please circle)
Friend or Family (name) ________________________________________
Major complaints, in order of importance to you: #1 ________________________________________
_____________________________________________________________________
____________________________________________________________
How does this condition impair your daily activities?
_______________________________________________
Treatments you have received for this condition?
__________________________________________________
Do you feel better since the onset of this condition? ________________________________________________
#2 ____________________________________________
_____________________________________________________________________
____________________________________________________________
How does this condition impair your daily activities?
_______________________________________________
Treatments you have received for this condition?
__________________________________________________
Do you feel better since the onset of this condition? ________________________________________________
#3 ________________________________________
_____________________________________________________________________
____________________________________________________________
How does this condition impair your daily activities?
_______________________________________________
Treatments you have received for this condition?
__________________________________________________
Do you feel better since the onset of this condition? ________________________________________________
Please rate your commitment to feeling better (On a scale of 1-10): What are your goals for your acupuncture visits?
_______________________________________________
Have you had acupuncture treatments before?
_________________________________________________
Do you have any concerns about having acupuncture? ACUPUNCTURE MEDICAL CONDITIONS
Please list conditions and surgeries you have had, along with the year diagnosed: Year
________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________
Please list all prescription medications you take, including those you use occasionally and Inhalers, nose sprays, and eye drops: Medication/Dose Purpose
________________________________ ______________________
________________________________ ______________________
________________________________ ______________________
________________________________ ______________________
________________________________ ______________________
Please list all supplements you take including vitamins:
________________________________ ______________________
________________________________ ______________________
________________________________ ______________________
________________________________ ______________________
________________________________ ______________________
Please list any allergies (seasonal, medications, environmental, food, etc.):
______________________________________________________________________________________________________________________________________________________________________________________
Please list any occupational concerns (stress, computer work, heavy lifting, etc):
___________________________________________________________________________________________
Please tell us about your exercise (regular, minimal, etc.):
___________________________________________________________________________________________
Musculoskeletal (Please list areas where you have problems, if any): Muscle Cramps? ____________________________
Muscle Pain? ______________________________
Joint Swelling? _____________________________ Tendonitis?
Arthritis? ____________________________________
Bursitis? __________________________________
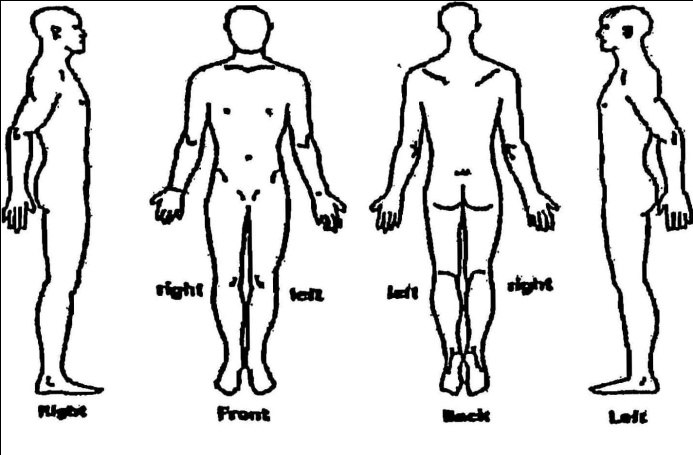
Please label (A,B,C,D) problem areas on diagram, then answer the questions about each area:
A: Sharp _____ Burning _____ Aching _____ Fixed _____ Other _____________________
B: Sharp _____ Burning _____ Aching _____ Fixed _____ Other _____________________
C: Sharp _____ Burning _____ Aching _____ Fixed _____ Other _____________________
D: Sharp _____ Burning _____ Aching _____ Fixed _____ Other _____________________
ACUPUNCTURE MEDICAL CONDITIONS (CONT) SYMPTOMS Note: For each symptom you currently have, rate its severity on scale from 1- 5 (1 being the least severity and 5 being the worst severity) Leave blank If Not Applicable LIVER / GALLBLADDER HEART / SMALL INTESTINES SPLEEN / STOMACH LUNG / LARGE INTESTINE
______ Clenching of Teeth at Night ______ Dry Cough
______ Sinus Infection / Congestion ______ Insulin Sensitivity
______ Itchy, Red or Painful Throat ______ Hemorrhoids
______ Dry Mouth / Throat / Nose ______ Constipation
KIDNEY / URINARY BLADDER BODY TEMPURATURE (Please check any that apply)
______ Hot Flush /Night Sweating ______ Normal
ENERGY LEVEL (Please circle) LOW 1 2 3 4 5 6 7 8 9 10 HIGH PERSONAL MEDICAL & FAMILY HEALTH HISTORY
Please indicate those that are current health problems for yourself and your family
members with a "C" under the appropriate person’s column. "P" should be used to indicate a past problem. Leave blank those that do not apply.
Other Emotional Problems: ______________________
If any of the above family members are deceased, please list their age at time of death and cause: _____________________________________________________________________________ _____________________________________________________________________________
ACUPUNCTURE PERSONAL INFORMATION For Women Only For Men Only
Have you had a hysterectomy? Yes No Impotence Testicular Pain/Lump
Could you be pregnant at this time? Yes No
Number of: Pregnancies _____ Births _______
For Women and Men Diet Information
Number of days in your monthly cycle? _____
Please describe your diet (low-fat, low-carb, vegetarian,
etc.): _______________________________________
Breakfast ____________________________________
Lunch ____________________________________
Dinner ____________________________________
Snacks ____________________________________
Before period During period After period
If you eat any of the following, please check
and list how much per week: Candy __________________________________
Chocolate _______________________________
Do you suffer from any of the following:
Soda - Regular/Diet ________________________
Milk ____________________________________
Pelvic Inflammatory Disease Ovarian cysts
Cheese __________________________________
Yogurt __________________________________
Breast Cysts Yeast Infections/Vaginitis
Eggs ___________________________________
Ice-cream _______________________________
Pasta ___________________________________
Coffee __________________________________
Alcohol _________________________________
Protein __________________________________ Dark
Fruit ____________________________________
Other ___________________________________
ACID-ALKALINE QUESTIONNAIRE SECTION A - HISTORY SECTION C – OTHER SYSTEMS
Circle the number score for each yes answer.
Enter the appropriate score for each symptom below. If a symptom is occasional or mild, score 1 points.
1. Have you taken tetracyclines (Sumycin, Panmycin
If a symptom is frequent or moderately severe, score 2 points.
Minocin, Vibramycin, etc.) or other antibiotics for one
If a symptom is severe or disabling, score 3 points.
2. Have you ever taken other "broad spectrum" antibiotics
for urinary, respiratory. or other infections for two
months or longer, or in shorter courses, four or more
3. Have you ever taken a "broad spectrum" antibiotic?
4. Have you ever been bothered by persistent prostatitis,
vaginitis, or other reproductive organ problems?
5. Have you been pregnant two or more times?
6. Have you taken birth control pills for more than two
7. Have you taken Prednisone, Decadron, or other
cortisone-type drugs for more than two weeks?
8. Does exposure to perfumes, insecticides, fabric shop
odors, and other chemicals provoke moderate to severe
9. Are symptoms worse on damp, muggy days, or in moldy
10. Have you had severe or persistent athlete's foot, ring
worm, jock itch, or chronic fungus infections of the skin
14. Does tobacco smoke really bother you?
SECTION A TOTAL
31. Recurrent infections or fluid in cars
SECTION B - MAJOR SYMPTOMS
Enter the appropriate score for each symptom below.
If a symptom is occasional or mild, score 3 points. SECTION C TOTAL
If a symptom is frequent or moderately severe, score 6 points.
If a symptom is severe or disabling, score 9 points. GRAND TOTAL SCORE _______________
4. Feeling "spacey" or "unreal"
Your Grand Total Score will help determine if your health
Yeast-connected health problems are:
Almost certainly present with scores over
15. Persistent vaginal burning or itching
Women with scores less than 60 and men with scores less than
40 are less apt to have yeast-connected health problems.
20. Cramps or other menstrual irregularities
SECTION B TOTAL ______
COMUNITÀ DELLA NATIVITÀ DELLA B.V. MARIA IN PRATOFONTANA DIACONIA DELL’OSPEDALE PSICHIATRICO GIUDIZIARIO Reggio Emilia Liturgia della Parola in lingua albanese “. ne nuk i dëgjojmë të flasin në gjuhët tona! veprat e pushtetshme e Perëndisë” 4 Mars 2012 Dytë e diela e Kreshmës Nga Libri i Zanafillës (22,1-2.9.10-13.15-18) 1Mbas këtyre gjërav
 ACUPUNCTURE
ACUPUNCTURE