Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Use of tamoxifen in advanced-stage hepatocellular carcinoma
Use of Tamoxifen in Advanced-Stage Hepatocellular Carcinoma A Systematic Review Anna K. Nowak, M.B.B.S., Ph.D. BACKGROUND. Hepatocellular carcinoma (HCC) is the third most common cause of Martin R. Stockler, M.B.B.S., M.Sc.
cancer mortality worldwide. Survival is poor for patients with advanced-stage HCC,
Pierce K. H. Chow, M.B.B.S.
and small trials of tamoxifen for patients with this disease have shown conflicting
Michael Findlay,
results. The authors conducted a systematic review of randomized clinical trials to
compare the effect of a tamoxifen-containing arm with a nontamoxifen-containing
1 National Health and Medical Research Council
(NHMRC) Clinical Trials Centre, University of Syd-
METHODS. Eligible trials were identified from the Cochrane Hepato-Biliary Group
ney, Camperdown, New South Wales, Australia.
register and other databases. Studies were selected for inclusion and their meth-
2 Sydney Cancer Centre, Royal Prince Alfred and
odologic quality assessed by three independent reviewers. Hazard ratios (HR) were
Concord Repatriation General Hospitals, Camper-
derived for overall survival where possible. Metaanalysis was performed using a
3 Department of General Surgery, Singapore Gen-
RESULTS. The authors identified 10 randomized trials with a total of 1709 patients.
eral Hospital, Singapore, Republic of Singapore.
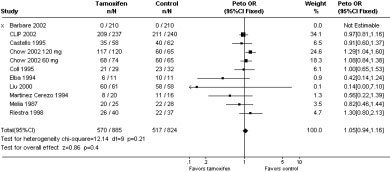
Use of tamoxifen had no effect on median survival (HR, 1.05; 95% confidence
4 Cancer Trials New Zealand, University of Auck-
interval, 0.94 –1.16; P ϭ 0.4) or tumor response rate. The findings were stable in
sensitivity analyses and were not affected by publication bias or inclusion of
low-quality studies or studies reported in abstract form only. Few adverse events or
withdrawals were noted. CONCLUSIONS. There was no support for the therapeutic use of tamoxifen in advanced HCC, nor for its use as a control arm in future clinical trials. Cancer 2005; 103:1408 –14. 2005 American Cancer Society. KEYWORDS: anti-estrogen, hepatocellular carcinoma, liver, neoplasm, systemic therapy, tamoxifen. Worldwide, hepatocellular carcinoma (HCC) is one of the most
common causes of death from malignant disease. Although less
common in Western populations, it is a significant cause of death ineastern Asia and sub-Saharan Africa.1 The etiology is believed to beassociated primarily with cirrhosis, due to chronic infection with
Dr. Anna Nowak is the recipient of the 2003Medical Oncology Group of Australasia/Novartis
hepatitis B or hepatitis C viruses, alcohol consumption, aflatoxin, or
hemachromatosis. People with HCC generally present with advanced-stage disease, although, more recently, some high-risk populations
The current study is based on a Cochrane review
have been targeted for screening, but the outlook is still poor in most
prepared for the Cochrane Hepato-biliary Group.37
Address for reprints: Martin R. Stockler, M.B.B.S.,
A variety of therapeutic modalities have been used in these pa-
NHMRC Clinical Trials Centre, University of Sydney,
tients.2 Surgery for early-stage disease results in some long-term
Locked Bag 77, Camperdown, New South Wales
survivors. However, the wide applicability of resection is often limited
1450, Australia; Fax: (011) 612-9562-5000; E-
by the poor synthetic function of the cirrhotic liver. The major prob-
lem after resection or local ablation is tumor recurrence, which often
Received August 26, 2004; revision received De-
occurs in the first 24 months after surgery.3,4 Long-term results similar
cember 7, 2004; accepted December 8, 2004.
to those for surgery have been reported with nonsurgical local abla-
2005 American Cancer SocietyDOI 10.1002/cncr.20963Published online 2 March 2005 in Wiley InterScience (www.interscience.wiley.com). Tamixofen for Advanced HCC/Nowak et al. TABLE 1 Search Strategy Register Search strategy Search date
Cochrane Hepato-Biliary Group Controlled Trials
(carcinoma OR neoplasm* OR cancer) AND (hepat* OR liver)
AND (tamoxifen OR antiestrogen* OR anti-estrogen)
Cochrane Central Register of Controlled Trials
(carcinoma OR neoplasm$ OR cancer) AND (hepat$ OR
liver) AND (tamoxifen OR antiestrogen* OR anti-estrogen)
(exp CARCINOMA/OR exp Neoplasms/) AND (exp Liver/OR
hepat$.mp) AND (exp Tamoxifen/OR exp EstrogenAntagonists/)
Abstracts from the Annual Scientific Meeting of
the American Society of Clinical Oncology
tive therapies such as percutaneous ethanol injec-
Eligibility Criteria for Inclusion in the Review
tion,5 radiofrequency ablation,6 and transarterial che-
Study type Unconfounded, truly randomized trials
moembolization.7 In addition, numerous cytotoxicagents have been investigated in trials comprising pa-
Treatment with any dose or duration of tamoxifen with
tients with HCC,8 and tumor response rates with sys-
or without other treatment modalities versus a
temically administered cytotoxic drugs are generally
control arm using placebo, no intervention, bestsupportive care, or the same other treatment
low, although they may be slightly higher when drugs
are administered regionally, with or without emboli-
zation.9 Any benefit from cytotoxic therapy must be
Diagnosis of HCC according to the definitions of
weighed against the associated toxicity.
individual trials (histology, cytology, or clinicalcriteria [e.g., typical imaging, raised AFP level, Ͼ 5
On the basis of the finding that some HCCs have
ϫ upper limit of normal, and a history of chronic
estrogen receptors (ER),10,11 several trials of the anti-
estrogen, tamoxifen, have been conducted. The earli-
Trials recruiting patients with apparently resected
est trials were small and had conflicting results. Al-
disease (testing tamoxifen as an adjuvant treatment)and trials recruiting patients with advanced or
though tamoxifen has been used in both women and
unresectable disease (testing tamoxifen as treatment
men with malignant disease, its putative mode of ac-
for advanced disease) were both eligible for
tion raises the question of whether its efficacy differs
inclusion; analyses were to be stratified according to
There have been 3 systematic reviews of ran-
domized controlled trials of treatments for
HCC: hepatocellular carcinoma; AFP: ␣-fetoprotein.
HCC.12–14 Whereas the 2 earlier reviews12,13 showeda marginal increase in survival with the use of ta-moxifen in advanced HCC, both noted that further
MATERIALS AND METHODS
large, well designed trials were needed to answer
A search by the secretariat of the Cochrane Hepato-
this question. The most recent review included fur-
Biliary Group used the search strategy described in
ther large trials and did not show any survival ben-
Table 1. References of review articles and identifiedtrials were also searched, and experts in the field con-
efit or antitumor effect for tamoxifen,14 and the
tacted, but no further trials were identified.
authors noted that only the trials assessed as lower
Titles of trials identified through this search strat-
egy were screened for possible eligibility, and the pro-
The current review extended the search beyond
spectively defined eligibility criteria (Table 2) were
Medline and added larger, more recent trials. The
applied to each trial by 3 independent reviewers, with
primary objective was to assess the effect of tamoxifen
disagreements resolved by discussion. Our search
on overall survival in patients with HCC. The second-
identified 42 reports, of which 19 were considered
ary objectives were to assess the effects of tamoxifen
potentially eligible. After further screening of the
on quality of life, tumor response, and treatment tox-
methods sections of the studies, 10 studies were in-
icity and, in addition, to assess whether there is an
cluded. Reasons for excluding trials included the fol-
interaction between gender and the effects of tamox-
lowing: no comparison group without tamoxifen,15–17
ifen on the overall survival or response rate.
confounded controls that added another drug to treat-
CANCER April 1, 2005 / Volume 103 / Number 7 TABLE 3 Study Characteristics evaluable patients Control arm Experimental arm Quality grade Reference
i.v.: intravenous. a Inadequate information available in abstract to classify quality.
ment in place of tamoxifen,18 studies that were not
the basis of actual (where available) or estimated max-
actually assessing the effect of tamoxifen,19 studies
imum and minimum follow-up times. To calculate an
that were assessing the affect of combination hor-
overall estimate of effect but avoid including the con-
monal therapy with tamoxifen and medroxyprogester-
trol group twice, the 3-arm study26 was analyzed using
one acetate,20 studies in which the outcome measures
one-half of the control group numbers as controls for
were unsuitable for analysis,21 studies with nonran-
each of the 2 experimental arms. A fixed-effect model
domized allocation to treatment and control arms,22,23
was used to calculate a pooled hazard ratio (HR) for
and publications that were found to be review articles.
overall survival, using the derived observed minus ex-
Methodologic quality was assessed independently
pected number of events and the variance obtained
by 3 reviewers using a modified subset of the MERGE
for each trial.25 The 95% confidence intervals (95% CI)
criteria,24 based on standard criteria to assess the de-
were calculated for individual and aggregate estimates
gree to which the study is susceptible to bias. The
criteria specifically take into account concealment oftreatment allocation, generation of the allocation se-
quence, blinding of treatment delivery, comparability
Of the 10 trials selected, 8 were fully reported, 2 were
between groups at baseline, inclusion of all random-
published in abstract form only, and 1709 patients
ized participants in the analysis, withdrawals from the
were included (Table 3). Nine studies examined the
trial, and valid assessment of end points. A global
effect of tamoxifen versus placebo or no treatment on
rating of quality and susceptibility to bias was then
outcomes that included overall survival. One study
assigned as follows: A) all or most criteria fulfilled:
randomized patients to 2 different doses of tamoxifen
where not fulfilled, it is believed very unlikely that the
in 2 arms in addition to the control arm.26 A single
conclusions of the study would be altered; B1)some
study examined the effect of adding tamoxifen to che-
criteria are fulfilled: where not fulfilled, it is believed
unlikely that the conclusions of the study would bealtered; B2) some criteria are fulfilled: where not ful-
Quality of the Studies
filled, it is believed likely that the conclusions of the
The methodologic quality of the studies was variable,
study would be altered; C) few or no criteria are ful-
with a low risk of bias in 3 trials (Grade A: 27%),26,28,29
filled: where not fulfilled, it is believed very likely that
a low to moderate risk in 3 trials (Grade B1:
the conclusions of the study would be altered.
27%),27,30,31 and moderate to high risk in 3 trials
Survival data were obtained indirectly using the
(Grade B2: 18%).32–34 Inadequate information was
methods described by Parmar et al.,25 by recording
available to classify 1 further study, published in ab-
actuarial survival proportions at predetermined time
stract form only.35 Six studies were placebo con-
points from Kaplan–Meier curves or tables. Censoring
trolled,26,28,30,31,33,34 although the study by Liu et al.
was accounted for by adjusting the numbers at risk on
was single-blinded only,33 and the adequacy of blind-
Tamixofen for Advanced HCC/Nowak et al.
treatment, and as high as 16 months in the studyallowing previous surgery.29
Funnel plots suggest the possibility of publication
bias, as there were several small trials with positiveresults, but no corresponding small trials with nega-tive results. The inclusion of unpublished and uniden-tified small trials with negative results could poten-tially show an overall detrimental effect of tamoxifen. None of the three trials showing a low potential forbias showed any survival benefits for tamoxifen. How-
FIGURE 1. Effect of tamoxifen on overall survival.
ever, this may be confounded by the use of higherdoses of tamoxifen in the studies showing the lowestpotential for bias.
ing in a further 2 studies was unclear.30,34 The remain-
The stratification of analyses according to stage of
der were either not placebo controlled27,29.32 or this
disease (i.e., postresection vs. advanced disease) was
planned, but could not be performed as no studiesincluded only postresection patients. Analysis using
Patient Characteristics
only studies with histologic or cytologic confirmation
The characteristics of patients in these 10 trials ap-
of the diagnosis was also planned originally. However,
peared similar. Their mean age ranged from 60 to 67
only 1 study, of 61 patients and overall poor quality,
years in the 9 studies testing tamoxifen alone, but was
fulfilled these criteria,30 and hence this analysis was
lower (52 years) in the study testing tamoxifen with
not done. In a further 5 trials, either histologic diag-
doxorubicin.27 Most patients were male in all studies
nosis or an elevated ␣-fetoprotein level together with
(range, 71– 89%). Underlying liver disease was re-
imaging suggestive of HCC was accepted.27,29,31–33 In
ported in 98 –100% of patients. Most studies excluded
these studies, a diagnosis was made without histology
patients with advanced concomitant liver disease,
or cytology examinations in 17%, 14%, 17%, 25%, and
with all studies including Ͻ 25% of patients with
24% of patients, respectively. A further 2 studies ac-
Child–Pugh Stage C liver disease, and Ͻ 25% of pa-
cepted similar criteria for diagnosis, but did not report
tients with Okuda Stage III disease. Only 1 study re-
the number of diagnoses made without histology or
ported including patients who had previously under-
cytology.26,28 Criteria for the diagnosis of HCC were
gone either surgery (5% of patients) or chemotherapy
Effect of Tamoxifen Treatment on Overall Survival Effect of Tamoxifen Dosage
In metaanalysis, overall survival was not affected by
It has been hypothesized previously that higher doses
the addition of tamoxifen (odds ratio, 1.05; 95% CI,
of tamoxifen could be more effective by invoking es-
0.94 –1.16; P ϭ 0.4) (Fig. 1). This comparison showed
trogen receptor-independent mechanisms of tumor
no significant statistical heterogeneity (P ϭ 0.2). One
inhibition.36 In the trials identified, the daily dose of
trial of 420 patients was necessarily excluded from the
tamoxifen varied, ranging from 20 mg in 5 tri-
metaanalysis because it reported insufficient data.35
als,27,28,30,32,35 30 mg in 1 trial,33 40 mg in 2 trials,29,31 to
However, it is unlikely that the availability of these
60 mg in 1 trial.34 A single 3-arm study randomized
data would change the overall review conclusions, as
patients to 2 high-dose levels of tamoxifen, 60 or 120
the trial showed no significant difference in median
mg daily, or placebo.26 In subgroup analysis, there was
survival between the tamoxifen and control arms.
an overall survival trend favoring the control arms
Exclusion of the single trial published in abstract
with higher doses of tamoxifen (Fig. 2). The HR for
form only for which results were available30 did not
overall survival was lowest for trials of tamoxifen 20
affect the results of the analysis (HR, 1.05; 95% CI,
mg daily (HR, 0.88; 95% CI, 0.69 –1.44; P ϭ 0.71),
0.94 –1.17; P ϭ 0.4). Median survival for both experi-
higher in trials of tamoxifen 40 mg daily (HR, 1.00; 95%
mental and control arms was available for all studies
CI, 0.85–1.19; P ϭ 1.0), higher still in trials of tamoxifen
reviewed, but was very variable, suggesting that the
60 mg daily (HR, 1.03; 95% CI, 0.81–1.31; P ϭ 0.8), and
patient groups were more heterogeneous than the
highest in the single trial of tamoxifen 120 mg daily
patient characteristics suggested. Median survival in
(HR, 1.29; 95% CI, 1.04 –1.6; P ϭ 0.02). There is unlikely
the control arm ranged from just over 1 month33 to 12
to be a place for further trials of tamoxifen dose esca-
months34 in groups without any previous surgical
CANCER April 1, 2005 / Volume 103 / Number 7
rubicin alone, and 16% in the group receiving doxo-rubicin plus tamoxifen, a difference that was not sta-tistically significant. There is no evidence thattamoxifen can produce objective tumor responses. Quality of Life Quality of life was examined in only 1 study using a validated tool (the European Organization for Re- search and Treatment of Cancer QLQ-C30 question- naire), but the data were not presented in detail.26 The authors commented that there were no appreciable differences in global quality of life between the treat- ment groups and that scores seemed somewhat lower with the highest dose of tamoxifen (120 mg). Thus, there is no evidence that tamoxifen can produce qual- ity-of-life benefits in these patients. Toxicity Treatment toxicity was not described as a predefined outcome in any study and was reported inconsis- FIGURE 2. Effect of tamoxifen dosage on overall survival.
tently. Reports of 2 trials made no mention of toxici-ty,27,30 whereas reports of 3 trials only included com-ments that treatment was “well tolerated” or had
Effect of Gender on Overall Survival
“negligible” or “minimal” toxicity.28,31,33 Reports of 3
The influence of gender on treatment effects was not
trials described minor side effects such as diarrhea,
an a priori objective in any of the trials. One trial
thrombophlebitis, vertigo, and hot flashes in a few
reported no difference in survival between men and
patients.32,34,35 The 2 largest trials reported toxicity in
women in post-hoc analysis.28 One trial reported a
more detail.26,29 Chow et al.26 graded toxicity as mild,
significant benefit of tamoxifen for men without major
moderate, or severe, with 3% of patients developing
hepatic insufficiency (P ϭ 0.02) but no benefit for
moderate or severe toxicity, with equal numbers receiv-
women (P ϭ 0.59).35 There were insufficient data for a
ing tamoxifen and placebo, and in this trial 1.5% of
metaanalysis on these subgroups. There was no com-
patients receiving tamoxifen withdrew from treatment
ment on gender differences in the only study to report
because of toxicity. The CLIP-1 investigators29 reported
estrogen receptor status in tumors.33 Furthermore, ER
that 10% of patients receiving tamoxifen developed tox-
status did not correlate with outcome in this trial.
icity, and 4% stopped tamoxifen because of toxicity. Asurprising absence was that none of the trial reports
Objective Tumor Responses and ␣-Fetoprotein
described thromboembolic events. This may reflect ei-
Responses
ther coagulopathy from underlying liver disease or lack
Assessment of tumor or serologic response was not an
of rigor in reporting adverse events.
a priori objective of any trial. Radiologic response wasreported in only 4 trials,27,28,30,33 and in these, tumor
DISCUSSION
response rates were not affected by the addition of
We identified 10 randomized trials testing tamoxifen
tamoxifen. Although the response criteria were not
in 1709 people with HCC and found no evidence of
defined, Coll et al.30 reported no partial responses (PR)
benefit. There were no apparent effects on survival,
and similar rates of progressive disease between
tumor response rate, or quality of life. Furthermore,
treated and untreated groups (78% vs. 79%). Castells et
the trials with the least risk of bias tended to show that
al.28 reported 1 PR (World Health Organization crite-
tamoxifen was associated with increased mortality,
ria) in the placebo group and the development of
whereas the trials with the largest risk of bias showed
progressive disease was not different between the 2
groups. Liu et al.33 reported no PRs and similar rates of
Funnel plots suggested publication bias, with sev-
progressive disease at 3 months (54% without tamox-
eral small positive trials and no corresponding small
ifen vs. 43% with tamoxifen). In the single trial com-
negative trials. It is possible that there are additional,
bining tamoxifen with chemotherapy, Melia et al.27
small, unpublished negative trials. Their inclusion
reported a PR rate of 11% in the group receiving doxo-
would improve the rigor of the current review, but
Tamixofen for Advanced HCC/Nowak et al.
would not affect its conclusion, namely, that the avail-
12. Mathurin P, Rixe O, Carbonell N, et al. Review article: over-
able evidence argues against use of tamoxifen in HCC.
view of medical treatments in unresectable hepatocellular
Many trials identified were of low methodologic
carcinoma—an impossible meta-analysis? Aliment Pharma-col Ther. 1998;12:111–126.
quality, with only two trials assessed as showing a low
13. Simonetti RG, Liberati A, Angiolini C, Pagliaro L. Treatment
potential for bias. Our findings that tamoxifen seemed
of hepatocellular carcinoma: a systematic review of ran-
to increase mortality in high-quality trials but have the
domized controlled trials. Ann Oncol. 1997;8:117–136.
opposite effect in low-quality trials support the con-
14. Llovet JM, Bruix J. Systematic review of randomized trials for
tention that low-quality trials are susceptible to bias.
unresectable hepatocellular carcinoma: chemoemboliza-tion improves survival. Hepatology. 2003;37:429 – 442.
However, we were not able to determine whether the
15. Group d’Etude et de Traitment de Carcinome Hepatocellu-
difference in treatment response was due to the meth-
laire. A multicenter randomized trial of anti-androgenic
odologic quality of the trials or the dose of tamoxifen,
(AA) treatment (leuproprelinϩ flutamideϩ tamoxifen vs ta-
as this finding is confounded by the use of higher
moxifen) in patients with unresectable hepatocellular carci-
doses of tamoxifen in the better-quality trials.
noma (HCC) [abstract]. Hepatology. 1998;28:249A.
16. Pelletier G, Ducreux M, Gay F, et al. Treatment of unresect-
These data argue against the use of tamoxifen in
able hepatocellular carcinoma with lipiodol chemoemboli-
advanced HCC. Further research on the effects of ta-
zation: a multicenter randomized trial. Groupe CHC.
moxifen in HCC is probably unwarranted. Tamoxifen
J Hepatol. 1998;29:129 –134.
should not be used as a control arm in trials in HCC.
17. Schachschal G, Lochs H, Plauth M. Controlled clinical trial
Future promising interventions should be tested in
of doxorubicin and tamoxifen versus tamoxifen mono-
large, well designed, randomized controlled clinical
therapy in hepatocellular carcinoma. Eur J GastroenterolHepatol. 2000;12:281–284.
18. Manesis EK, Giannoulis G, Zoumboulis P, et al. Treatment of
hepatocellular carcinoma with combined suppression and
REFERENCES
inhibition of sex hormones: a randomized, controlled trial. Hepatology. 1995;21:1535–1542.
Murray C, Lopez A. Mortality by causes for eight regions ofthe world: Global Burden of Disease Study. Lancet. 1997;349:
19. Raoul JL, Guyader D, Bretagne JF, et al. Randomized con-
trolled trial for hepatocellular carcinoma with portal vein
Fong Y, Kemeny N, Lawrence TS. Cancer of the liver and
thrombosis: intra-arterial iodine-131-iodized oil versus
biliary tree. In: DeVita V, Helmann S, Rosenberg S, editors.
medical support. J Nucl Med. 1994;35:1782–1787.
Cancer: principles and practice of oncology. 6th ed. Phila-
20. Uchino J, Une Y, Sato Y, et al. Chemohormonal therapy of
delphia: JP Lippincott, 2001:1162–1203.
unresectable hepatocellular carcinoma. Am J Clin Oncol.
Ikeda K, Saitoh S, Koida I, et al. Imaging diagnosis of small
hepatocellular carcinoma. Hepatology. 1994;20:82– 87.
21. Das J, Faiz M, Rahman M, et al. Effects of tamoxifen on the
Belghiti J, Panis Y, Farges O, et al. Intrahepatic recurrence
survival of patients with advanced hepatocellular carci-
after resection of hepatocellular carcinoma complicating
noma. J Inst Postgrad Med Res. 1999;14:1–5.
cirrhosis. Ann Surg. 1991;214:114 –117.
22. Farinati F, De Maria N, Fornasiero A, et al. Prospective
Livraghi T, Bolondi L, Buscarini L, et al. No treatment,
controlled trial with antiestrogen drug tamoxifen in patients
resection and ethanol injection in hepatocellular car-
with unresectable hepatocellular carcinoma. Dig Dis Sci.
cinoma: a retrospective analysis of survival in 391 patients
with cirrhosis. Italian Cooperative HCC Study Group.
23. Farinati F, Salvagnini M, de Maria N, et al. Unresectable
J Hepatol. 1995;22:522–526.
hepatocellular carcinoma: a prospective controlled trial
Livraghi T, Goldberg SN, Lazzaroni S, et al. Small hepato-
with tamoxifen. J Hepatol. 1990;11:297–301.
cellular carcinoma: treatment with radio-frequency ablation
24. Liddle JW, Irwig, L. Method for evaluating research and
versus ethanol injection. Radiology. 1999;210:655– 661.
guideline evidence. Sydney: New South Wales Department
Group d’Etude et de traitment de carcinoma hepatocellu-
of Health; 1996. Available from URL: http://www.health.
laire. A comparison of lipiodol chemoembolization and con-
nsw.gov.au/public-health/merge/merge.html [accessed July 6,
servative treatment for unresectable hepatocellular carci-
noma. N Engl J Med. 1995;332:1256 –1261.
25. Parmar MK, Torri V, Stewart L. Extracting summary statistics
Nowak AK, Chow PKH, Findlay M. Systemic therapy for
to perform meta-analyses of the published literature for
advanced hepatocellular carcinoma: a review. Eur J Cancer.
survival endpoints. Stat Med. 1998;17:2815–2834.
26. Chow PK, Tai BC, Tan CK, et al. High-dose tamoxifen in the
Llovet JM, Real MI, Montana X, et al. Arterial embolisation
treatment of inoperable hepatocellular carcinoma: a multi-
or chemoembolisation versus symptomatic treatment in pa-
center randomized controlled trial. Hepatology. 2002;36:
tients with unresectable hepatocellular carcinoma: a ran-
domised controlled trial. Lancet. 2002;359:1734 –1739.
27. Melia WM, Johnson PJ, Williams R. Controlled clinical trial
10. Nagasue N, Kohno H, Chang Y, et al. Specificity of androgen
of doxorubicin and tamoxifen versus doxorubicin alone in
receptors of hepatocellular carcinoma and liver in humans.
hepatocellular carcinoma. Cancer Treat Rep. 1987;71:1213–
Hepatogastroenterology. 1990;37:474 – 479.
11. Jonas S, Bechstein WO, Heinze T, et al. Female sex hormone
28. Castells A, Bruix J, Bru C, et al. Treatment of hepatocellular
receptor status in advanced hepatocellular carcinoma and
carcinoma with tamoxifen: a double-blind placebo-con-
outcome after surgical resection. Surgery. 1997;121:456 –
trolled trial in 120 patients. Gastroenterology. 1995;109:917–
CANCER April 1, 2005 / Volume 103 / Number 7
29. Perrone F, Gallo C, Daniele B, et al. Tamoxifen in the treat-
with expression of hormone receptors: a prospective ran-
ment of hepatocellular carcinoma: 5-year results of the
domized study. Am J Gastroenterol. 2000;95:218 –222.
CLIP-1 multicentre randomised controlled trial. Curr Pharm
34. Elba S, Giannuzzi V, Misciagna G, Manghisi OG. Random-
ized controlled trial of tamoxifen versus placebo in inoper-
30. Coll S, Sola R, Vila M, et al. Treatment with tamoxifen in
able hepatocellular carcinoma. Ital J Gastroenterol. 1994;26:
patients with advanced hepatocellular carcinoma. Results of
a randomized placebo controlled trial [abstract]. Hepatol-
35. Barbare J-C, Milan C, Bouche´ O, et al. Treatment of ad-
vanced hepatocellular carcinoma (HCC) with tamoxifen: a
31. Riestra S, Rodriguez M, Delgado M, et al. Tamoxifen does
phase III trial in 420 patients [abstract 551]. Proc Am Soc
not improve survival of patients with advanced hepatocel-
lular carcinoma. J Clin Gastroenterol. 1998;26:200 –203.
36. Tan CK, Chow PK, Findlay M, et al. Use of tamoxifen in
32. Martinez Cerezo FJ, Tomas A, Donoso L, et al. Controlled
hepatocellular carcinoma: a review and paradigm shift. J
trial of tamoxifen in patients with advanced hepatocellular
Gastroenterol Hepatol. 2000;15:725–729.
carcinoma. J Hepatol. 1994;20:702–706.
37. Nowak A, Findlay M, Culjak G, Stockler M. Tamoxifen for
33. Liu CL, Fan ST, Ng IO, et al. Treatment of advanced hepa-
hepatocellular carcinoma. Cochrane Database Syst Rev.
tocellular carcinoma with tamoxifen and the correlation
Vulnerable patients with a fractured neck of femur:nutritional status and support in hospitalM. Nematy,* M. Hickson,* A.E. Brynes,* C.H.S. Ruxton & G.S. Frost**Nutrition and Dietetic Research Group, Imperial College London, Hammersmith Hospitals Trust, London W12 0HS, UK; Schoolof Biosciences, University of Westminster, London W1W 6UW, UKMalnutrition has serious consequences forrecover
Medigene’s decision to expand its clinical programme for RhuDex in primary biliary cirrhosis (PBC) should result in a more meaningful outcome than would have been possible under previous plans. Although the revised Phase II study wil now not start until H114 (previously a Phase IIa was to start in Q113), we believe the delay should be worth it in the long run, making RhuDex a more valuable
 Tamixofen for Advanced HCC/Nowak et al.
Tamixofen for Advanced HCC/Nowak et al.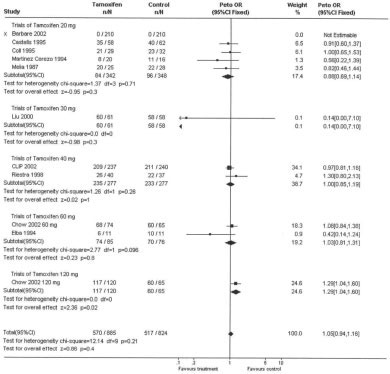 CANCER April 1, 2005 / Volume 103 / Number 7
CANCER April 1, 2005 / Volume 103 / Number 7