Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Doi:10.1016/j.transproceed.2004.06.039
Primary Immunosuppression Regimen of Rapid Steroid Withdrawal After Living Related Liver Transplantation: A Single-Center Experience
Y. Toyoki, K. Hakamada, S. Narumi, E. Totsuka, M. Nara, H. Ono, Y. Ishizawa, M. Sasaki
Corticosteroids have been considered the mainstay of immunosuppressive therapy
after liver transplantation. However, the side effects of long-term steroid use such asdiabetes, infections, and bone disease, including growth retardation in children, are seriousproblems. Our immunosuppression regimen includes FK506 and steroid withdrawal by 30days after transplantation. The aim of this study was to determine the outcomes of livertransplant, using this immunosuppressive regimen.
Fifteen primary liver transplant recipients were performed between January
1994 and May 2003 and data were reviewed retrospectively. Eight pediatric and four adultrecipients, who had survived more than 3 months after transplantation, were included inthis sample. The immunosuppressive regimen consisted of FK 506 (Prograf), initially atdoses of 0.03 mg/kg, with dose adjustments to achieve daily trough levels of approximately10 to 12 ng/mL, and predonisone, initially at 4 mg/kg/d, with a taper and cessation by 30days when the graft was stable.
All recipients were successfully withdrawn by 30 days. Acute rejection episodes
occurred in three patients, no patient was diagnosed with chronic rejection. The acuterejection-free rate at 5 year was 74.1%. No recipient had diabetes, serious infections orbone disease.
Our primary immunosuppressive regimen of rapid steroid withdrawal is
safe with regard to acute and chronic rejection with benefits upon steroid-related sideeffects.
ORTHOTOPIC LIVER TRANSPLANTATION is a nosuppression regimen is initiated with FK506 with steroid
commonly accepted therapy for patients with end-
withdrawal by 30 days after transplantation.
stage liver disease. Immunosuppressive drugs, includingcorticosteroids, have contributed to the success of liver
transplantation. Corticosteroids are still considered a main-
The records of eight pediatric and seven adult primary liver
stay of immunosuppressive therapy after liver transplanta-
recipients who received transplants between January 1,
tion. However, their side effects such as diabetes, suscepti-
1994, and August 31, 2003, were reviewed retrospectively.
bility to infections, hypercholesterolemia, and bone disease,
Three adult liver transplant recipients died within 3 months
including growth retardation in children, are serious prob-
after living related liver transplantation: two cases due to
lems. Therefore, adequate immunosuppressive therapy, in-
portal vein thrombosis, and one case due to infectious
cluding avoidance of these steroid-related side effects, is a
myocarditis. Finally, eight pediatric and four adult recipi-
goal in long-term management of organ transplant recipi-ents. Some reports indicate that maintenance immunosup-
From the Department of Surgery, Hirosaki University School of
pression without steroids has the advantage of no steroid-
related side effects without an increased incidence of
Address reprint requests to Yoshikazu Toyoki, Department of
rejection and graft The timing of steroid withdrawal
Surgery, Hirosaki University School of Medicine, 5 Zaifu-cho,
varies between liver transplant centers, but is generally
Hirosaki, Aomori 036-8216, Japan. E-mail: ytoyoki@cc.hirosaki-
performed after 3 months post transplantation. Our immu-
2004 by Elsevier Inc. All rights reserved.
360 Park Avenue South, New York, NY 10010-1710
Transplantation Proceedings, 36, 2279 –2281 (2004)
Table 1. Demographic Characterization of Our Recipients
PSC, primary sclerosing cirrhosis; LC, liver cirrhosis; SAFHF, subacute fulminant hepatic failure; NNH, neonatal hepatitis; LOHF, late-onset hepatic failure.
ents who had survived and were followed more than 3
Renal Function and Immunosuppression-Related
months after living related liver transplantation were in-
cluded in this study. Patient age, gender, and the primary
Fasting serum creatinine levels as well as renal function
diagnosis for liver transplantation are shown in
have remained within the normal range though the post-
Median follow-up is 52.652 months (6.441 to 114.477
transplantation periods. Nine liver transplant recipients had
months). Our immunosuppression regimen consisted of FK
no immunosuppression related complications; however,
506 (Prograf), initially at doses of 0.03 mg/kg with dose
one adolescent recipient experienced a CMV infection; one
adjustments to achieve daily trough levels of approximately
pediatric recipient a candida infection; and one other
10 to 12 ng/mL, and predonisone, initially at 4 mg/kg/d, with
patient, an episode of convulsions. All three patients recov-
a taper and cessation of steroid therapy by 30 days post-
transplantation if the graft was stable. We conducted thisretrospective review to determine whether our immunosup-pressive regimen with rapid steroid withdrawal was safe to
suppress acute and chronic rejection among both adult andchild recipients of living related liver transplantation and to
The acute rejection free rate at 5 years was 74.1%
Two recipients were diagnosed with acute rejection patientswithin the first month after liver transplantation, and one at
6 months after steroid withdrawal. All three recipientsexperienced only one acute rejection that reversed with a
All recipients underwent steroid withdrawal by 30 to 70
steroid pulse alone. No patients were diagnosed with
days after liver transplantation. Currently 10 recipients are
maintained on FK506 alone and one recipient on pre-donisolone alone. One recipient was completely withdrawnfrom immunosuppressive therapy and his graft function isstable. Three recipients were diagnosed with acute rejectionepisodes and no patients with chronic rejection. None of therecipients showed diabetes, serious infections, or bonedisease.
Serum alanine aminotransferase and total bilirubin of allrecipients remained within the normal range from 3 monthsoccurred after transplantation. During the first 6 monthsafter transplantation, FK506 trough levels were 10 to 12ng/mL and at 24 months after transplantation they rangefrom 4 to 6 ng/mL.
Fasting Serum Cholesterol and Blood Glucose
Fasting serum cholesterol and blood glucose levels haveremained within the normal range though the posttrans-plant periods.
Acute rejection, free rate at 5 years was 74.1%.
glucose levels remained normal after steroid withdrawal. FK506 trough levels ranged from 4 to 6 ng/mL since year 2
For more than 25 years, liver transplantation has been
after liver transplantation. We have not seen serious ste-
recognized as the accepted therapy for end-stage liver
roid-related side effects, such as hyperglycemia or bone
disease in both adults and children. With newer and more
efficient immunosuppressive therapies, the optimal regi-
The potential benefits of steroid withdrawal are directly
mens should be reconsidered for long-term liver transplant
related to their side effects, especially to produce growth
recipients. Avoidance of steroid-related side effects is a goal
retardation in pediatric recipients. Vo Thi Diem et al
in the long-term management of organ transplant recipi-
reported an improvement in growth after steroid withdraw-
ents. Some reports indicate that maintenance immunosup-
There was an improvement in height z-score among our
pression without steroids has the advantage of no steroid-
pediatric recipients, except one patient who has growth
related side effects without an increased incidence of
retardation due to nonalcoholic steatohepatitis after liver
rejection and graft The timing of steroid withdrawal
varies between liver transplant centers, but is generally
In summary, our primary immunosuppressive regimen
performed beyond 3 months after transplantation. Our
with rapid steroid withdrawal for both adult and child
immunosuppression regimen is initiated with FK506 and
recipients of living related liver transplantation suppresses
steroid withdrawal occurs about 30 days after transplanta-
acute and chronic rejection and avoids steroid-related side
tion. The purpose of this study was to review our experience
to determine the characteristics of these patients.
In this study, all liver transplant recipients had an attempt
at steroid withdrawal by 30 days. Two recipients experi-enced acute rejection within 30 days after liver transplan-
1. Fraser GM, Grammonstianos K, Reddy J, et al: Liver Transpl
tation and were weaned from steroids at 60 and 68 days
2. Stegall MD, Everson GT, Schorter G, et al: Hepatology
after transplantation. Only one patient experienced acute
rejection at 6 months after steroid withdrawal. The acute
3. Gomez R, Moreno E, Colina F, et al: J Hepatol 28:150, 1998
rejection free rate at 5 years was 74.1%. No recipients had
4. Tisone G, Angelico M, Palmieri G, et al: Transplantation
been diagnosed with chronic rejection. In our data, liver
5. Vo Thi Diem H, Sokal EM, Janssen M, et al: Transplantation
and renal function, fasting serum cholesterol, and blood
WELCOME TO FULLMOONWATER CHINESE MEDICINE CONTACT INFORMATION _______________________________________________________________________________________________ Preferred Phone: (circle: Home Cell Work) ________________________________________________________________Do we have your permission to send appointment reminders, health newsletters, and occasional promotions to your email address
Patient information The information in this leaflet is to guide your use of nortriptyline this medicine safely. Further information is available inside the What is nortriptyline for? Notriptyline is a medicine which may help improve your pain control. It is different from other pain relief drugs. It can help nerve PHARMACY DIRECTORATE pain, for example shooting or burning
 Primary Immunosuppression Regimen of Rapid Steroid Withdrawal
Primary Immunosuppression Regimen of Rapid Steroid Withdrawal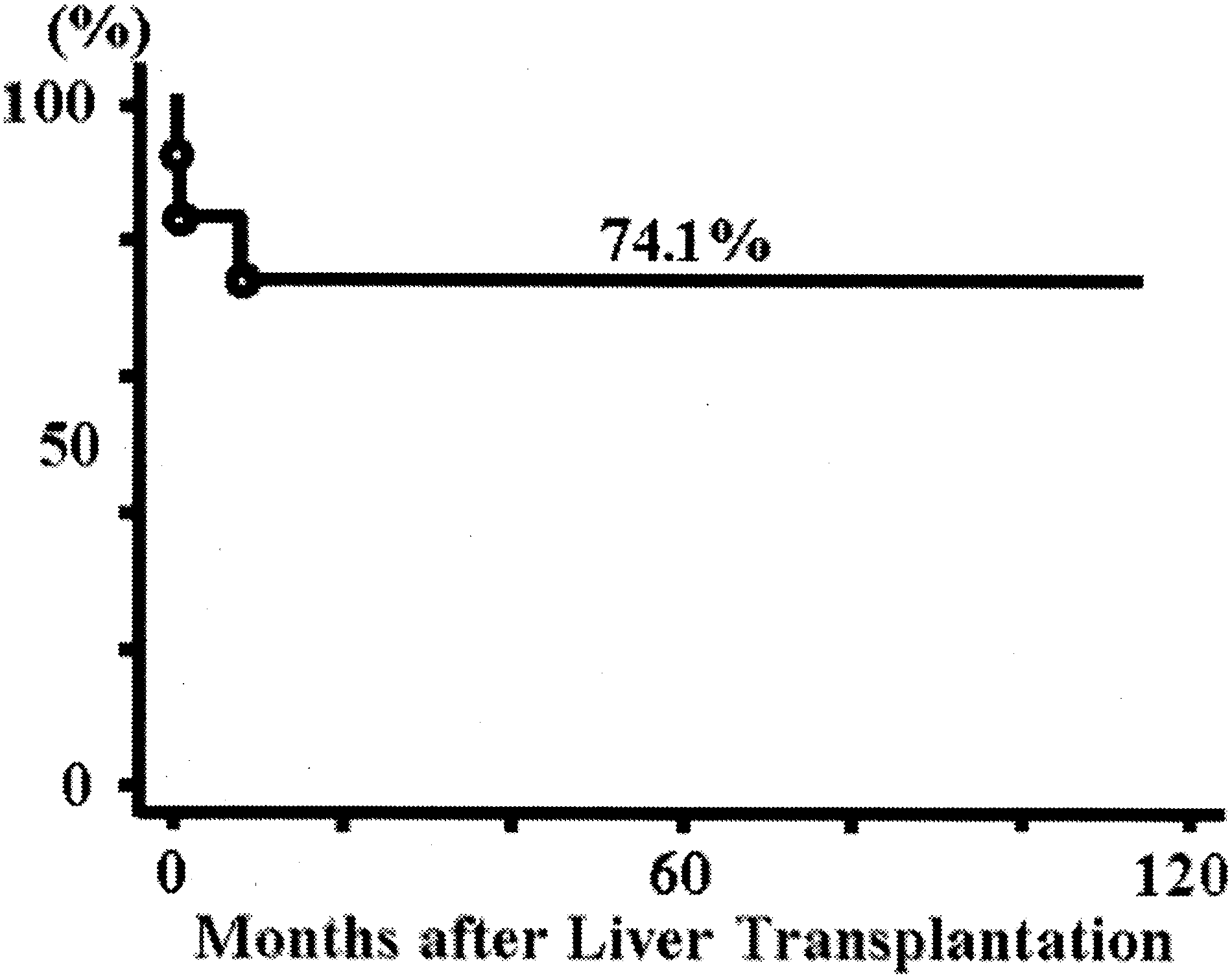 Table 1. Demographic Characterization of Our Recipients
Table 1. Demographic Characterization of Our Recipients