Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Doi:10.1016/s0140-6736(99)05036-9
Articles
Tamoxifen in treatment of intraductal breast cancer: NationalSurgical Adjuvant Breast and Bowel Project B-24 randomisedcontrolled trial
Bernard Fisher, James Dignam, Norman Wolmark, D Lawrence Wickerham, Edwin R Fisher, Eleftherios Mamounas, Roy Smith, Mirsada Begovic, Nikolay V Dimitrov, Richard G Margolese, Carl G Kardinal, Maureen T Kavanah,Louis Fehrenbacher, Robert H Oishi
IntroductionUntil the mid-1980s, mastectomy followed by axillary
Background We have shown previously that lumpectomy with
dissection was the preferred treatment for primary
radiation therapy was more effective than lumpectomy alone
invasive breast cancer and ductal carcinoma in situ
for the treatment of ductal carcinoma in situ (DCIS). We did a
(DCIS). That therapeutic approach was challenged,
double-blind randomised controlled trial to find out whether
however, as a result of more widespread use of better
lumpectomy, radiation therapy, and tamoxifen was of more
diagnostic equipment and an increased effort to educate
benefit than lumpectomy and radiation therapy alone for DCIS.
women about the value of early detection of breast
Methods 1804 women with DCIS, including those whose
tumours. Invasive and non-invasive tumours were foundmore frequently and at earlier stages, often before they
resected sample margins were involved with tumour, were
became clinically evident. Before the availability of
randomly assigned lumpectomy, radiation therapy (50 Gy), and
mammography, fewer than 3% of newly diagnosed breast
placebo (n=902), or lumpectomy, radiation therapy, and
cancers were DCIS, and most presented as large
tamoxifen (20 mg daily for 5 years, n=902). Median follow-up
palpable masses, many with areas of microinvasion.1,2
was 74 months (range 57–93). We compared annual event
Since the introduction of mammography, 20–30% of
rates and cumulative probability of invasive or non-invasive
mammographically detected cancers are DCIS.3
ipsilateral and contralateral tumours over 5 years.
The management of primary invasive breast cancer and
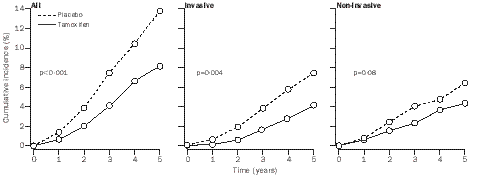
Findings Women in the tamoxifen group had fewer breast-
DCIS was influenced by a report which showed that the
cancer events at 5 years than did those on placebo (8·2 vs
outcome in women with invasive breast cancer treated by
13·4%, p=0·0009). The cumulative incidence of all invasive
lumpectomy and radiation therapy was similar to that of
breast-cancer events in the tamoxifen group was 4·1% at 5
women treated by radical or modified radical
years: 2·1% in the ipsilateral breast, 1·8% in the contralateral
mastectomy.4 Mastectomy for the treatment of invasivedisease therefore became more difficult to justify for
breast, and 0·2% at regional or distant sites. The risk of
invasive disease, but was frequently advocated for the
ipsilateral-breast cancer was lower in the tamoxifen group
management of DCIS, a non-invasive cancer. Thus,
even when sample margins contained tumour and when DCIS
surgery for removal of localised DCIS was commonly
more radical than that for removal of localised invasive
disease. Uncertainty therefore arose about the clinical
therapy, and tamoxifen was effective in the prevention of
management of women with small, localised DCIS
detected by mammography, and prompted the NationalSurgical Adjuvant Breast and Bowel Project (NSABP) to
do the B-17 study, a randomised controlled trial to
investigate whether excision of localised DCIS withtumour-free sample margins (referred to as lumpectomy,although most women had no palpable mass) followed by
National Surgical Adjuvant Breast and Bowel Project (NASBP),
radiation therapy was more effective than lumpectomy
Allegheny University of the Health Sciences 4 Allegheny
Suite 602, Pittsburgh, PA 15212–5234, USA (Prof B Fisher MD,
alone in prevention of an invasive tumour in the ipsilateral
R Smith MD); Department of Biostatistics (J Dignam PhD) and NSABP
Biostatistical Center (M Begovic MD), University of Pittsburgh,
The first findings of B-17 reported a significantly better
Pittsburgh; Allegheny General Hospital, Pittsburgh
overall 5-year event-free survival because of lower
D L Wickerham MD); Institute of Pathology, Shadyside Hospital,
incidence of invasive and non-invasive ipsilateral-breast
Pittsburgh (E R Fisher MD); Mount Sinai Center for Breast Health,
cancers among women who underwent lumpectomy and
Cleveland, OH (E Mamounas MD); Michigan State University, East
radiation therapy.5 At 8 years, findings were confirmed of
Lansing, MI (N V Dimitrov MD); Jewish General Hospital, Montreal,
lower cumulative incidence of both types of ipsilateral-
Quebec, Canada (R G Margolese MD); Alton Ochsner MedicalFoundation, New Orleans, LA (C G Kardinal
breast cancer because of lumpectomy and radiation
Center, Boston, MA (M T Kavanah MD); Kaiser Permanente, Northern
therapy for localised mammographically detected DCIS.6
California Region, CA (L Fehrenbacher MD); and University of Hawaii,
The study concluded that, because of the low recurrence
rate of invasive ipsilateral-breast cancer, mastectomy was
not warranted in women who had DCIS similar to that of
Many women were ineligible for participation in B-17
because mammography showed diffuse DCIS and
resected sample margins contained DCIS, or scattered
calcifications were thought to be benign or associated with
unremoved DCIS. Those women were mainly treated by
mastectomy. Tamoxifen had been shown in animal
studies to have anti-initiator and antipromoter
properties.7,8 We have also reported that tamoxifen
prevents tumour recurrences in the ipsilateral breasts and
second primary tumours in the contralateral breasts of
women who have undergone lumpectomy and radiation
therapy for primary invasive breast cancer,9,10 which
suggests that tamoxifen can interfere with development of
primary invasive breast cancer from the start or with
Table 1: Characteristics of patients and tumours
progression of DCIS to invasive cancer. As a result, wedesigned the NSABP B-24 randomised controlled trial.
scattered microcalcifications that had been classified on
The B-17 and B-24 studies were based on the idea that
radiological assessment as suspicious were eligible if biopsy
DCIS either progresses from non-invasive to invasive
cancer or is a marker of risk rather than a progenitor forthe subsequent occurrence of an invasive tumour, or that
a focus of invasive cancer existing in conjunction with
After women had undergone lumpectomy and given written
DCIS might remain after lumpectomy. In the B-24 study,
consent, they were randomly assigned radiation therapy to the
a double-blind randomised controlled trial, we tested the
ipsilateral breast and placebo (n=902) or radiation therapy
hypothesis that, in patients with non-invasive DCIS,
followed by tamoxifen (n=902). To avoid an imbalance in
treatment with lumpectomy, postoperative radiation
characteristics according to treatment assignment, we stratifiedwomen by age (р49 years or >49 years), tumour type (DCIS or
therapy, and tamoxifen would be more effective than
DCIS plus LCIS), and method of detection (mammography,
lumpectomy and radiation therapy alone in prevention of
invasive and non-invasive cancers in the ipsilateral and
Radiation therapy (50 Gy) was administered as stipulated in the
contralateral breast. We present results from B-24 and
protocol,4,5,12 and was started no later than 8 weeks after surgery.
relate them to those from B-17 and the NSABP P-1
Placebo or tamoxifen 10 mg twice daily were administered within
56 days of lumpectomy and were given continuously for 5 years. No dose modifications were made for either agent. Patientsunderwent physical examinations every 6
mammography once a year. Tumours detected at local or regional
sites were taken as events only if tissue biopsy of the lesion was
Women with DCIS were eligible for inclusion if their life
positive. Tumours detected at distant sites (ie, before local or
expectancy was at least 10 years. Women with tumours that
regional invasive cancer was noted) were taken as events if clinical,
consisted of DCIS and lobular carcinoma in situ (LCIS) were
radiographic, or pathological findings showed that a tumour was
also eligible. Although we did not require or recommend axillary
present. The presence of ipsilateral-breast or contralateral-breast
dissection in B-24, if it was done, all lymph nodes had to be
tumours, regional or distant metastases, second primary tumours
negative for tumour on histological assessment. Time between
other than a breast tumour that occurred as a first event, or death in
surgery and randomisation had to be 56 days or less. Women
the absence of evidence of recurrent breast cancer were used to
who had previously been diagnosed with cancer, except for
determine event-free survival. Our primary endpoints were the
those who had had in-situ carcinoma of the cervix or squamous-
occurrence of invasive or non-invasive tumours in the ipsilateral or
cell or basal-cell carcinoma of the skin, were not eligible. We
included women with one or more masses or clusters ofcalcifications that could be excised. Women whose DCIS or
LCIS showed microscopic margin-involvement were eligible, as
We calculated cause-specific hazards of failure and hazard rate
were women with scattered calcifications that were thought to be
ratios for the various endpoints, with exact binomial methods
benign or of indeterminate nature (ie, those for whom follow-up
used to test for differences in rates by treatment group. Cox’s
assessment was recommended). Women with scattered
proportional hazards model was used to calculate relative risks of
calcifications that were classified as suspicious and who had no
failure according to prognostic covariates and treatment
signs of invasive cancer were also eligible. Women with no
simultaneously, and to find out whether there was a differential
definite clusters of calcifications or masses but who had diffuse
response to therapy according to characteristics (eg, treatment-
Breast cancer at regional or distant sites
Second primary cancers other than endometrial cancer
*Rate per 1000 patients per year. †Rate in tamoxifen group divided by rate in placebo group. ‡Includes ipsilateral-breast cancer, contralateral-breast cancer, and local, regional, and distant disease. §Includes ipsilateral and contralateral non-invasive tumours.
Table 2: Site, cumulative incidence, rate, and rate ratios of first events
covariate interactions).13 We calculated cumulative probability of
A comprehensive analysis based on additional follow-up data was
events by means of cumulative incidence curves, which correctly
done later. Our results reflect information reported to the
account for competing risks.14 Event-free and total survival
NSABP data centre as of Dec 31, 1998.
curves were calculated by Kaplan-Meier analysis. Pointwiseasymptotic 95% CI are presented for cumulative incidence andsurvival curves.
We aimed to achieve 85% power to detect a 50% lower
1804 women were randomly assigned treatment between
occurrence of invasive cancer for women who received
May 9, 1991, and April 13, 1994 (figure 1). 29 (1·6%)
tamoxifen, with a one-sided 0·05 significance criterion. We
patients (11 on placebo, 18 on tamoxifen) became
anticipated that women who received tamoxifen would haveoutcomes at least as favourable as those of women who received
ineligible after randomisation because primary tumours
placebo, and, therefore, our original study design characterised
showed characteristics other than those of non-invasive
the tests as one-sided. However, all p values presented are two-
intraductal carcinoma (13) or because surgery after
sided. The design specifications required that a minimum of 72
diagnosis was delayed, surgical procedures were not done
events (invasive cancer in the ipsilateral or contralateral breast or
correctly, because of previous cancers, or because of other
metastases to other sites) occurred among all patients before
reasons (16). Of the 1804 randomised patients, 14 (0·8%)
analysis. Three interim analyses did not result in stopping the
did not begin the assigned therapy. 564 (31·3%)
study early. The adjusted significance criterion for the definitive
patients (269 in the placebo group and 295 in the
analysis, based on a log-rank test for the comparison of time toinvasive breast cancer, was 0·0483, according to the method of
tamoxifen group) who started therapy discontinued
Fleming and colleagues.15 After the requisite number of events
treatment because of side-effects (98 placebo,
had been seen, we did a preliminary analysis for the investigators.
tamoxifen), personal reasons (146 placebo,
Figure 2: Cumulative Incidence of all, invasive, and non-invasive events in ipsilateral and contralateral breastAll and invasive include cancers at regional and distant sites. p values based on comparisons of average annual rates of failure.
Figure 3: Cumulative Incidence of all and invasive events in ipsilateral and contralateral breastp values based on comparisons of average annual rates of failure.
124 tamoxifen), and unspecified reasons (25 placebo,
25 tamoxifen). We included all women in the analyses,
There were 295 breast-cancer and non-breast-cancer
however, for whom follow-up information was available,
events among the 1798 patients with follow-up (table 2).
including those who did not meet eligibility criteria. An
At 5 years of follow-up, 83·3% (95% CI 80·8–85·8) of
analysis of only eligible patients produced similar results
patients who received placebo were event-free compared
and conclusions. Median follow-up was 74 months (range
with 87·4% (85·1–89·6) of tamoxifen-treated patients
Patients’ characteristics were similar in the two groups
Among patients who received placebo, 130 invasive and
(table 1). 65% of women reported being postmenopausal.
non-invasive breast-cancer events occurred in the
16% of women had positive resected sample margins after
ipsilateral breast, contralateral breast, or presented as
definitive surgery. More than 80% of tumours had
metastases at regional or distant sites, compared with 84
maximum dimensions of 1 cm or less, were not palpable,
in the tamoxifen group (table 2, figure 2). The estimated
and were detected by mammography alone.
rate ratio for all breast cancer (0·63 [95% CI 0·47–0·83])
Covariate relative risk (95% CI) ‡
*Invasive and non-invasive. †Rate per 1000 patients per year. ‡Relative risk for patients in given covariate stratum, relative to reference (first) stratum, adjusted for treatment. §Includes unknown (79 and 94 in placebo and tamoxifen groups, respectively). These patients had failure rates similar to failure rate in women with positive margins.
Table 3: Relation between selected chcracteristics of patients and tumours and rates and relative risks of ipsilateral-breast tumours
represented 37% fewer events in the tamoxifen group.
among women who received tamoxifen (data not shown).
There were 43% fewer invasive breast-cancer events and
The relative risk of contralateral-breast cancer was 0·58
31% fewer non-invasive breast-cancer events in the
(0·35–0·97), which represents 42% fewer contralateral-breast
tumours among women who received tamoxifen.
150 (70%) of the 214 breast-cancer events were in the
Ten patients had tumours other than in the breast. In
ipsilateral breast (table 2, figure 3). A lower rate of
the placebo group, tumours occurred in the liver, lung,
ipsilateral-breast tumours in the tamoxifen group was
thorax, ipsilateral axilla (three patients), and ipsilateral-
apparent only for invasive tumours (44% reduction). The
chest wall. In the tamoxifen group, tumours occurred in
rate of non-invasive ipsilateral-breast tumours was not
the contralateral and ipsilateral axilla (two patients,
significantly lower in the tamoxifen group than in the
table 2). These ten patients were eligible for the trial since
placebo group (18% reduction, p=0·43). Of the 150
they had no invasive disease at the time of study entry. In
patients with ipsilateral-breast tumours, 64% were treated
nine women, the primary DCIS was 1·0 cm or less in size;
by mastectomy; the remainder had a second lumpectomy.
five tumours had comedonecrosis and seven had negative
The type of surgery after ipsilateral-breast tumour
was similar in the two groups; 68% of women who
The two groups did not differ in the rate of occurrence
received placebo and 59% of those who received
of second primary cancers other than those in the breast
tamoxifen underwent mastectomy. Women who had
or endometrium (table 2). 26 second cancers occurred in
invasive ipsilateral-breast tumours were, however, treated
women who received placebo and 25 in women treated
by mastectomy more frequently than those who had a
with tamoxifen. In each group, the tumours were widely
non-invasive ipsilateral-breast tumour (75 vs 56%,
distributed in various sites; there was no evidence of a
difference in the incidence of tumours in the placebo or
36 contralateral-breast tumours (23 invasive and 13
tamoxifen groups at any site. There was a non-significant
non-invasive) occurred as first events in the placebo group
excess of endometrial cancer in patients who received
and 18 (15 invasive and three non-invasive) occurred in
tamoxifen: seven in the tamoxifen group compared with
the tamoxifen group (table 2, figure 3). The estimated
two in the placebo group (relative risk 3·4 [0·6–33·4]).
relative risk of contralateral-breast cancer was 0·48
The incidence of deaths that occurred before a breast-
(0·26–0·87), which represents 52% fewer contralateral-
cancer recurrence or before a second primary cancer was
breast tumours for patients who received tamoxifen. The
also similar in the two groups. 11 deaths were seen in the
cumulative incidence of all contraleratal-breast tumours
placebo group and ten in the tamoxifen group.
occurring at 5 years as first events was 3·4% in theplacebo group and 2·0% in the tamoxifen group. The
Relation of characteristics to outcome
reduction in invasive contralateral-breast tumours (23 vs
Age at diagnosis was significantly associated with
15 events, 37%) was not significant (p=0·22). The
occurrence of ipsilateral-breast tumour. Younger patients
reduction in non-invasive contralateral-breast tumours
in the two groups were at higher risk than older patients
seemed larger, although the number of events was small
for such an event (table 3). The annual rate of ipsilateral-
(13 vs three, 78%, p=0·02). The cumulative incidence of
breast tumour per 1000 women aged 49 years or younger
invasive and non-invasive contralateral-breast tumours at
who received placebo was 33·3 and 13·03 for those aged
5 years was low. The 5-year cumulative incidence of
50 years or older. Tamoxifen administration resulted in a
invasive contralateral-breast tumours was 2·3% in the
38% reduction in ipsilateral-breast tumours in women
placebo group compared with 1·8% in the tamoxifen
younger than 50 years and a 22% reduction in women
group; for non-invasive contralateral-breast tumours, it
The presence of positive tumour-margins after surgery
When contralateral-breast tumours that occurred as first
was also associated with an increased rate and relative risk
events or subsequent to other events were taken into account,
of invasive or non-invasive ipsilateral-breast tumour.
39 were seen among women in the placebo group and 23
Similar findings occurred in patients whose DCIS were
Figure 4: Cumulative Incidence of all, invasive, and non-invasive events in ipsilateral and contralateral breast in B-17 and B-24studies
palpable compared with those whose disease was
or initial tumour characteristics were associated with a
diagnosed by mammography alone. The risk was lower for
significantly increased risk of contralateral-breast cancer.
ipsilateral-breast cancer among women who receivedtamoxifen, irrespective of margin status (22% lower in
women in the tamoxifen group whose sample margins
28 women in the placebo group and 26 in the tamoxifen
were negative, and 44% in those with positive or unknown
group died. At 5 years from study entry, survival was 97%
margins). For a few women whose DCIS was clinically
(96–98) for the two groups (p=0·74, data not shown). Six
apparent at the time of study entry, failure rates were
of the 28 women in the placebo group had invasive breast
substantially higher in the two groups than for those
cancer and two of these six had invasive ipsilateral-breast
without clinically apparent DCIS (table 3).
tumours. Four women on tamoxifen had invasive breast
Patients whose initial DCIS showed comedonecrosis, as
cancer, and three of these four had invasive ipsilateral-
reported by institutional pathologists, were about twice as
breast tumours. One developed a new primary cancer.
likely to develop an ipsilateral-breast tumour as womenwhose DCIS showed no comedonecrosis. This
observation was more strongly associated with the
Information about toxic events was available for 1781
occurrence of a non-invasive than with an invasive
(98·7%) randomised patients (table 4). No strokes were seen
ipsilateral-breast tumour (data not shown). The rate of
in the two groups. Grade 4 toxic effects not usually
ipsilateral-breast tumour was, however, lower by a similar
associated with tamoxifen occurred with similar rates in the
degree in the tamoxifen group in women who had no
two groups. There was an increase in the rate of endometrial
comedonecrosis (23%) and in those who showed evidence
cancer in tamoxifen-treated patients, (1·53 vs 0·45 per 1000
of comedonecrosis at entry (31%). None of the patients’
patients per year in the placebo group). No deaths fromendometrial cancer occurred in the tamoxifen group.
Women with DCIS treated by lumpectomy and radiation
therapy showed additional benefit from tamoxifen. The
advantage was due mainly to a decrease in the rate of
invasive cancer, especially in the ipsilateral breast. That
effect was also seen in the rate of invasive and non-
invasive tumours in the contralateral breast and at
regional or distant sites. When the events of those sites
were combined, there was a significantly lower rate and
cumulative incidence of all breast-cancer-related events
than in the placebo group. These observations suggest
that focusing on the frequency with which ipsilateral-
breast tumours occur after lumpectomy for DCIS is too
limited; the possible effect that treatment strategies for
DCIS have on all invasive or non-invasive breast-cancer
events at any site seems more important. Therefore, the
few metastases that were detected at regional and distant
sites in this study cannot be ignored, especially since
Almost two-thirds of the patients in the two groups who
developed non-invasive ipsilateral-breast tumours during
*Excludes alopecia, irregular menses, hot flashes, fluid retention, vaginal discharge,nadir grades, and weight gain or loss; septic episode classified as grade 4.
the first 5 years of follow-up underwent mastectomy, an
Table 4: Adverse events by treatment group
accepted treatment, although a second breast-conserving
procedure might have been possible. The large number of
tumours that were oestrogen-receptor positive. Tamoxifen
mastectomies performed lessened the opportunity for
also lowered rates of invasive tumours in P-1 participants
estimating the frequency of subsequent invasive cancers in
with a history of atypical hyperplasia or LCIS, which are
women with a history of DCIS. Studies to ascertain
frequently oestrogen-receptor positive.19,20 Since DCIS is
whether a second lumpectomy in conjunction with
commonly associated with tumour cells that are
tamoxifen is adequate therapy are appropriate.
oestrogen-receptor and progesterone-receptor positive,19–25
Our findings from this study can be considered in the
tamoxifen could have led to lower rates of oestrogen-
context of the B-17 findings because the studies were
receptor-positive invasive cancers in in this study after
similar except for inclusion in B-24 of women with more
extensive DCIS. The cumulative incidence of all breast-
In the P-1 study, the lower risk of invasive cancer in
cancer events at 5 years in the placebo group of B-24 was
women with a history of LCIS or atypical hyperplasia was
similar to that in women who were treated by lumpectomy
because of tamoxifen administration, whereas in
and radiation therapy in B-17. The spectrum of results
participants with DCIS in the B-17 study and this study
from the two studies clearly depicts the advantage from
the lower risk was because of postoperative breast
radiation therapy, as well as the added benefit of
irradiation and the difference was greater when tamoxifen
tamoxifen (figure 4). In the B-17 study, the cumulative
was administered with radiation therapy. Therefore, the
incidence of all breast-cancer-related events in women
effectiveness of tamoxifen in treating DCIS without
with DCIS treated by lumpectomy alone was about 25%
radiation therapy is speculative. A study currently in
at 5 years. The cumulative incidence was 13% after
radiation therapy in the two trials, and 8% when
The nature and magnitude of tamoxifen’s side-effects
tamoxifen was given in B-24. This benefit was due partly
were similar to those seen in other NSABP trials of
to the lower rate of contralateral-breast cancer and of
tamoxifen. The increase in the rate of endometrial cancer
invasive cancer at regional and distant sites in tamoxifen-
after tamoxifen administration and the rate of deep-vein
treated women. Thus, tamoxifen and radiation therapy
thrombosis and pulmonary emobolism were minimal
led to a 68% lower cumulative incidence of all breast-
(<1%) and there were no strokes. Despite the small
cancer events at 5 years of follow-up than in women
increases in rate of certain adverse events, adverse effects
treated with lumpectomy alone in B-17. Compared with
from surgery, radiation therapy, and chemotherapy in
women who underwent lumpectomy alone, the tamoxifen
unprevented breast cancers would probably have
group showed a 77% reduction in all invasive breast-
exceeded those associated with tamoxifen. Nevertheless,
cancer events and about 64% reduction for all non-
before women receive the drug, they should be carefully
screened so that only those who are free of comorbid
In this study, as in B-17,16,17 positive sample margins
disorders that would predispose them to such events are
and comedonecrosis were associated with an increased
risk of ipsilateral-breast tumours. Tamoxifen reduced the
Our findings could contribute to the decision-making
incidence of such tumours, irrespective of the presence or
absence of comedonecrosis or of margin involvement. An
mammographically detected DCIS when radiological or
8-year update of the B-17 findings has, however, shown
pathological evidence suggests that all of the cancer was
that, although comedonecrosis continues to be a predictor
not removed after lumpectomy. Currently, mastectomy is
of ipsilateral-breast tumour, margin status had less of an
commonly deemed appropriate when scattered
influence18 than in earlier reports.
calcifications are seen radiographically or more than one
Our findings from this trial and those of the B-17 study
focus of clustered calcifications persist after surgery, when
are related to those of the NSABP P-1 trial,11 which
radiologists are uncertain about whether findings are
showed that tamoxifen administered to women at
indicative of invasive cancer, when sample margins
increased risk for breast cancer led to 50% fewer non-
contain DCIS after lumpectomy, or when a tumour is at
invasive tumours (DCIS and LCIS) and 49% fewer
or close to a margin. Our findings for ipsilateral-breast
invasive breast cancers than placebo. B-17 showed that
tumours are encouraging because they suggest that
lumpectomy-treated women with a history of DCIS were
mastectomy could be avoided more frequently than at
at greater risk for invasive breast cancer than were women
present. Moreover, the value of tamoxifen used in
in P-1 who had a history of LCIS or atypical hyperplasia.
combination with radiation therapy to lower the
In B-17, the annual rate of an invasive-breast-cancer event
occurrence of invasive cancer justifies the suggestion that
during the first 5 years after the occurrence of DCIS was a
combined therapy replaces mastectomy for the treatment
little more than twice that which occurred after LCIS and
of DCIS patients in whom radiological findings are
nearly three times that after atypical hyperplasia. The
unlikely to be related to an invasive tumour.
B-17 study and the present study showed that invasive-
cancer rates in DCIS patients who received radiation
Bernard Fisher, Norman Wolmark, and D Lawrence Wickerham were
therapy alone were higher than those in patients with a
involved in the design and implementation of the study. James Dignamwas responsible for statistical analysis. Edwin Fisher was the senior
history of LCIS or atypical hyperplasia who had received
pathologist. Eleftherios Mamounas was the protocol officer from 1991–97.
tamoxifen alone. Since women with a history of LCIS or
Roy Smith was protocol officer and, with Mirsada Begovic, extensively
atypical hyperplasia have been thought to be at sufficiently
reviewed patients’ records. Nikolay Dimitrov, Richard Margolese,Carl Kordinal, Maureen Kavanah, Louis Fehrenbacher, and Robert Oishi
high risk of invasive cancer to warrant receiving
contributed to the implementation and conduct of the study at major
tamoxifen, women with DCIS, who are at even higher
recruitment sites. Bernard Fisher and James Dignam prepared the first
risk, should also be considered as candidates for
draft of the paper, to which all investigators contributed.
tamoxifen, even if they have been treated with radiation
Clinical Centres that contributed ten or more patients (shows
therapy. The P-1 findings provide a biological basis for
principal investigator and program coordinator)Baptist Regional Cancer Institute, Jacksonville, FL, USA N Abramson,
such a theory since they showed that tamoxifen lowered
P Stokes; Baylor-Sammons Cancer Center, Dallas, TX, M D Grant,
the rate of invasive tumours overall because of an effect on
B Quast; Baystate Medical Center, Springfield, MA, W P Reed,
T Barron; Boston Medical Center, Boston, MA, M T Kavanah,
Fisher B, Bauer M, Margolese R, et al. Five-year results of a
D McDonald; British Columbia Cancer Agency, Vancouver, Canada,
randomized clinical trial comparing total mastectomy and segmental
I A Olivotto, C Trevisan; Community Clinical Oncology Program,
mastectomy with or without radiation in the treatment of breast
Allegheny, Pittsburgh, PA, R P Pugh; Community Clinical Oncology
cancer. N Engl J Med 1985; 312: 665–73.
Program, Alton Ochsner Medical Foundation, New Orleans, LA,
Fisher B, Costantino J, Redmond C, et al. Lumpectomy compared
C G Kardinal, M Bateman; Community Clinical Oncology Program,
with lumpectomy and radiation therapy for the treatment of
Columbia River Oncology Program, Portland, OR, K S Lanier,
intraductal breast cancer. N Engl J Med 1993; 328: 1581–86.
L Birenbaum; Community Clinical Oncology Program, Evanston
Fisher B, Dignam J, Wolmark N, et al. Lumpectomy and radiation
Hospital/Kellogg Cancer Center, Evanston, IL, J D Khandekar, B Marks;
therapy for the treatment of intraductal breast cancer: findings from
Community Clinical Oncology Program, Grand Rapids, MI, S L Smiley;
National Surgical Adjuvant Breast and Bowel Project B-17. J Clin
Community Clinical Oncology Program, Marshfield Clinic, Marshfield,
Oncol 1998; 16: 441–52.
WI, J L Hoehn, L Weigel; Community Clinical Oncology Progam, Mount
Jordan VC. Effect of tamoxifen (ICI 46,474) on initiation and growth
Sinai Medical Center, Miami Beach, FL, E Davila, J W Grimes;
of DMBA-induced rat mammary carcinomata. Eur J Cancer 1976; 12:
Community Clinical Oncology Program, Northwest, Tacoma, WA,
H I Pierce, K Hart; Community Clinical Oncology Program, South East Cancer Control Consort, Winston-Salem, NC, J N Atkins,
Jordan VC, Allen KE. Evaluation of the antitumour activity of the
R R Burgess; Community Clinical Oncology Program, St Louis, MO,
nonsteroidal antioestrogen monohydroxytamoxifen in the DMBA-
R J Baglan; CHA-Pavillon Saint-Sacrement, Quebec City, Quebec,
induced rat mammary carcinoma model. Eur J Cancer 1980; 16:
Canada, J Robert, E P Marcoux; City of Hope Medical Center, Duarte,
CA, L D Wagman, D Hooks; Colorado Cancer Research Program,
Fisher B, Costantino J, Redmond C, et al. A randomized clinical trial
Denver, CO, S Sedlacek, N J Morton; Cross Cancer Institute, Edmonton,
evaluating tamoxifen in the treatment of patients with node-negative
Alberta, Canada, A W Lees, C Danbrook; Fallon Clinic, Worcester, MA,
breast cancer who have estrogen-receptor-positive tumors. N Engl J
J P Wei; Glens Falls Hospital, Glens Falls, NY, R W Sponzo,
Med 1989; 320: 479–84.
B A Sponzo; Hartford Hospital, Hartford, CT, P A DeFusco, J M Kulko;
10 Fisher B, Redmond C. New perspective on cancer of the contralateral
Henry Ford Hospital, Detroit, MI, R A Chapman, T J Doyle; Jewish
breast: a marker for assessing tamoxifen as a preventive agent. J Natl
General Hospital, Montreal, Quebec, Canada, R G Margolese, D Poulin;
Cancer Inst 1991; 83: 1278–80.
Kaiser Permanente, Northern California Region, CA, L Fehrenbacher,
11 Fisher B, Costantino JP, Wickerham DL, et al. Tamoxifen for
A Rodoni; Kaiser Permanente, Portland, OR (Cooperative Group
prevention of breast cancer: report of the National Surgical Adjuvant
Outreach Programme), M U Rarick; Kaiser Permanente, San Diego, CA,
Breast and Bowel Project P-1 study. J Natl Cancer Inst 1998; 90:
J Polikoff, S Cory; Lahey Clinic Medical Center, Burlington, MA,
K S Hughes; Lehigh Valley Hospital, Allentown, PA, H C Hoover Jr,
12 Fisher B, Wolmark N, Fisher ER, Deutsch M. Lumpectomy and
A Geshan; London Regional Cancer Center, Ontario, Canada,
axillary dissection for breast cancer: surgical, pathological, and
F E Perera; Lutheran Healthcare Network, Mesa, AZ, M M Long;
radiation considerations. World J Surg 1985; 9: 692–98.
M D Anderson Cancer Center, Houston, TX, F C Ames; Minority-Based
13 Prentice RL, Kalbfleisch JD, Peterson AV, Flournoy N, Farewell VT,
Community Clinical Oncology Program, Virginia Commonwealth
Breslow NE. The analysis of failure times in the presence of
University, Richmond, VA, H D Bear, L Keener; Michigan State
competing risks. Biometrics 1978; 34: 541–54.
University, East Lansing, MI, N V Dimitrov, C Robins; Montreal General
14 Gaynor JJ, Feuer EJ, Tan CC, et al. On the use of cause-specific
Hospital, Montreal, Quebec, Canada, M P Thirlwell; Mount Sinai
failure and conditional failure probabilities: examples from clinical
Medical Center, Cleveland, OH, L Levy, S Reynolds; New England
oncology data. J Am Stat Assoc 1993; 88: 400–09.
Medical Center Hospitals, Boston, MA, R A Graham, M J Scannell; OhioState University, Columbus, OH, W B Farrar; Ontario Cancer
15 Fleming TR, Harrington DP, O’Brien PC. Designs for group
Foundation-Hamilton Clinic, Ontario, Canada, H Lukka; Puget Sound
sequential tests. Controlled Clin Trials 1984; 5: 348–61.
Oncology Consortium, Seattle, WA, R B Clarfeld, N L Knudsen;
16 Fisher ER, Costantino J, Fisher B, Palekar AS, Redmond C,
Radiological Associates of Sacramento, CA, M H Leibenhaut, C Brooks;
Mamounas E. Pathologic findings from the National Surgical
Rockford Clinic, Rockford, IL, W R Edwards, S M Richter; Royal
Adjuvant Breast and Bowel Project (NSABP) Protocol B-17:
Victoria Hospital, Montreal, Quebec, Canada, H R Shibata,
intraductal carcinoma (duct carcinoma in situ). Cancer 1995; 115:
J Pepe-Aylward; Rush Presbyterian-St Luke’s Medical Center, Chicago,
IL, J M Wolter, D B Madrid; St Vincent Hospital, Indianapolis, IN,
17 Fisher ER. Pathobiological considerations relating to the treatment of
J A Cavins; Sutter West Cancer Research Group, Greenbrae, CA,
intraductal carcinoma (ductal carcinoma in situ) of the breast. CA
P D Eisenberg, L Friedman; Tom Baker Cancer Centre, Calgary, Alberta,
Cancer J Clin 1997; 47: 52–64.
Canada, A H G Paterson, L Dobni; University of Cincinnati, OH,
18 Fisher ER, Dignam J, Tan Chiu E, et al. Pathologic findings from the
B Aron, MA Schilds; University of Hawaii, Honolulu, HI, R H Oishi,
National Surgical Adjuvant Breast Project (NSABP) eight-year update
D Coleman; University of Iowa, Iowa City, IA (Cooperative Group
of protocol B-17. Cancer 1999 (in press).
Outreach Programme), P Jochimsen, M Spaight; University of Kentucky,
19 Giri DD, Dundas SA, Nottingham JF, Underwood JC. Oestrogen
Lexington, KY, E H Romond, M Ashki; University of Massachusetts,
receptors in benign epithelial lesions and intraductal carcinomas of
Worcester, MA, M E Costanza; University of Medicine/Dentistry, New
the breast: an immunohistological study. Histopathology 1989; 15:
Brunswick, NJ, I L Wapnir, A G Owens; University of Michigan, Ann
Arbor, MI, L H Baker, B Golden; University of North Carolina, Chapel
20 Barnes R, Masood S. Potential value of hormone receptor assay in
Hill, NC (Cooperative Group Outreach Program), S A Bernard,
carcinoma in situ of breast. Am J Clin Pathol 1990; 94: 533–37.
G C Huitt; University of Pittsburgh Cancer Institute, PA, V G Vogel,
21 Zafrani B, Leroyer A, Fourquet A, et al. Mammographically detected
L Robertson; University of Texas, San Antonio, TX, A B Cruz Jr,
ductal in situ carcinoma of the breast analyzed with a new
I Presas; University of Vermont, Burlington, VT (Cooperative
classification: a study of 127 cases: correlation with estrogen and
progesterone receptors, P53 and c-erb B-2 proteins, and proliferative
activity. Semin Diagn Pathol 1994; 11: 208–14.
We thank Tanya Spewock for editorial assistance, Mary Hof for
22 Allred DC, Berardo MD, Prosser J, O’Connell P. Biologic and genetic
preparation of the paper, and Linda Gilarski for data management. The
features of in-situ breast cancer. In: Silverstein M, ed. Ductal
study was supported by Public Health Service grants U10-CA-12027,
carcinoma in situ of the breast. Baltimore: Williams and Wilkins,
U10-CA-69651, U10-CA-37377, and U10-CA-69974 from the National
Cancer Institute, National Institutes of Health, and Department of Health
23 Pallis L, Wilking N, Cedermark B, Rutqvist LE, Skoog L. Receptors
for estrogen and progesterone in breast carcinoma in situ. Anticancer Res 1992; 12: 2113–15.
24 Berardo M, Hilsenbeck SG, Allred DC. Histological grading of
noninvasive breast cancer and its relationship to biological features.
Rosner D, Bedwani RN, Vana J, Baker HW, Murphy GP. Lab Invest 1996; 74: 15A (abstr 68).
Noninvasive breast carcinoma: results of a national survey by the
25 Leal CB, Schmitt FC, Bento MJ, Maia NC, Lopes CS. Ductal
American College of Surgeons. Ann Surg 1980; 192:139–47.
carcinoma in situ of the breast: histologic categorization and its
Lagios MD, Westdahl PR, Margolin FR, Rose MR. Duct carcinoma
relationship to ploidy and immunohistochemical expression of
in situ: relationship of extent of noninvasive disease to the frequency of
hormone receptors, p53, and c-erb B-2 protein. Cancer 1995; 75:
occult invasion, multicentricity, lymph node metastases, and short-
term treatment failures. Cancer 1982; 50:1309–14.
26 Recht A, Rutgers EJ Th, Fentiman IS, Kurtz JM, Mansel RE, Sloane
Ernster VL, Barclay J, Kerlikowske K, et al. Incidence of and
JP. The Fourth EORTC DCIS Consensus Meeting (Château
treatment for ductal carcinoma in situ of the breast. JAMA 1996; 275:
Marquette, Heemskerk, The Netherlands, 23–24 January 1998)
Conference Report. Eur J Cancer 1998; 34: 1664–69.
Vatikanoko II. Kontzilioaz haratago gaurko kulturatik bi arotara, bi eoitara. are bizkorrago eta kementsuago jarrai -tzen du aurrera. 1. Mundu modernoarekin adiski- detu raino bakarrik iritsi zela. Eta erdibide-listaren artean, mundua tragikoki bana-tua zegoela, herrialde kolonizatuenzuen, eta erdizka bakarrik lortu; bitar-tean, ordea –Kontzilioko eta ondoren-go urteetan– kultu
Casos Prácticos ASPECTOS GENERALES Moralidad de los actos humanos Exposición del caso: El viernes por la tarde, Lorenzo se reúne con sus amigos para ver una cinta de vídeo. La película resulta ser "El Doctor Zhivago". La acción se sitúa en la Revolución rusa. La joven protagonista es una chica guapa, buena, con gran corazón, a la que los acontecimientos maltratan
 Articles
Articles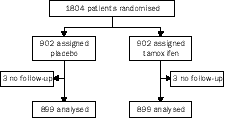
 Many women were ineligible for participation in B-17
because mammography showed diffuse DCIS and
resected sample margins contained DCIS, or scattered
calcifications were thought to be benign or associated with
unremoved DCIS. Those women were mainly treated by
mastectomy. Tamoxifen had been shown in animal
studies to have anti-initiator and antipromoter
properties.7,8 We have also reported that tamoxifen
prevents tumour recurrences in the ipsilateral breasts and
second primary tumours in the contralateral breasts of
women who have undergone lumpectomy and radiation
therapy for primary invasive breast cancer,9,10 which
suggests that tamoxifen can interfere with development of
primary invasive breast cancer from the start or with
Table 1: Characteristics of patients and tumours
progression of DCIS to invasive cancer. As a result, wedesigned the NSABP B-24 randomised controlled trial.
Many women were ineligible for participation in B-17
because mammography showed diffuse DCIS and
resected sample margins contained DCIS, or scattered
calcifications were thought to be benign or associated with
unremoved DCIS. Those women were mainly treated by
mastectomy. Tamoxifen had been shown in animal
studies to have anti-initiator and antipromoter
properties.7,8 We have also reported that tamoxifen
prevents tumour recurrences in the ipsilateral breasts and
second primary tumours in the contralateral breasts of
women who have undergone lumpectomy and radiation
therapy for primary invasive breast cancer,9,10 which
suggests that tamoxifen can interfere with development of
primary invasive breast cancer from the start or with
Table 1: Characteristics of patients and tumours
progression of DCIS to invasive cancer. As a result, wedesigned the NSABP B-24 randomised controlled trial.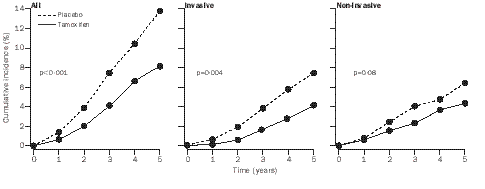
 Breast cancer at regional or distant sites
Second primary cancers other than endometrial cancer
*Rate per 1000 patients per year.
Breast cancer at regional or distant sites
Second primary cancers other than endometrial cancer
*Rate per 1000 patients per year.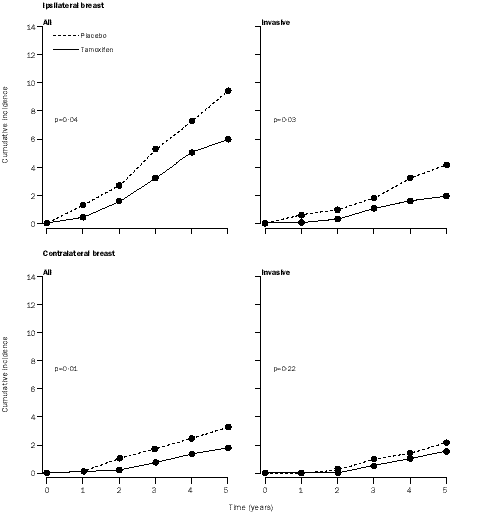
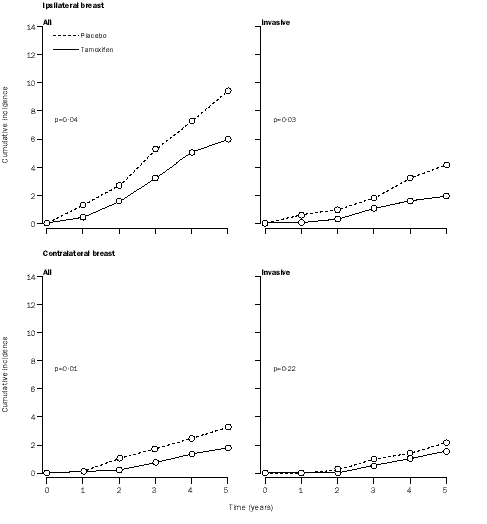 Figure 3: Cumulative Incidence of all and invasive events in ipsilateral and contralateral breastp values based on comparisons of average annual rates of failure.
Figure 3: Cumulative Incidence of all and invasive events in ipsilateral and contralateral breastp values based on comparisons of average annual rates of failure.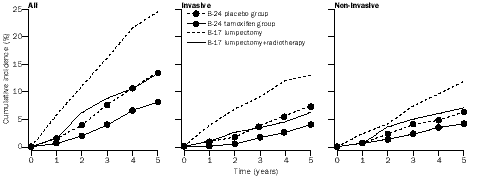
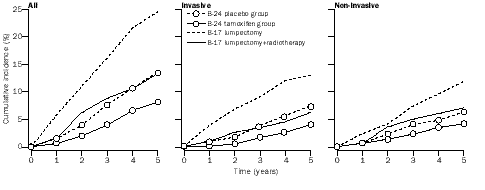 Figure 4: Cumulative Incidence of all, invasive, and non-invasive events in ipsilateral and contralateral breast in B-17 and B-24studies
palpable compared with those whose disease was
or initial tumour characteristics were associated with a
diagnosed by mammography alone. The risk was lower for
significantly increased risk of contralateral-breast cancer.
Figure 4: Cumulative Incidence of all, invasive, and non-invasive events in ipsilateral and contralateral breast in B-17 and B-24studies
palpable compared with those whose disease was
or initial tumour characteristics were associated with a
diagnosed by mammography alone. The risk was lower for
significantly increased risk of contralateral-breast cancer.