Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Successful bicom treatment of central nervous system disorders in children
Going beyond the Herpes Viruses in BICOM treatment of Chronic Fatigue and Fibromyalgia Andrew Barrie PhD, and Mrs D. Anna Barrie, non-medical practitioners. Energy Waves Clinic, Adelaide, Australia. INTRODUCTION
The purpose of this paper is to share the experiences and successes of our clinic in Australia where we have been using the bioresonance method since 1998 after training in England. Initially we were seeing 60 – 70 patients per week but currently we see only half this number to make time for training and support of other therapists in the region as we are also the Regumed representatives. We pass on enquiries for simple treatments to other therapists and mainly see ‘difficult’ cases, often as referrals from other BICOM therapists or medical practitioners with a positive attitude towards bioresonance. Our findings from Australia are not only relevant to practitioners in Australasia and Asia but also to practitioners anywhere because people now travel so widely for business or holiday. There is also evidence that global warming is causing diseases carried by insects to be moving into colder parts of Europe. The general principles we are describing may be adapted to any location. It just requires a little research on your behalf. With about half the patients we see, their main complaint is constant fatigue and general pain. Often, they have not been officially diagnosed by a medical specialist with Chronic Fatigue Syndrome ,CFS, (also known as Myalgic Encephalomyelitis, ME). Patients may tell us this is because they have lost faith in orthodox medicine, or that they fear a diagnosis of CFS will lead to problems with employers or insurance companies. It has been estimated that fewer than 16% of sufferers are diagnosed and treated [1]. There is now general acceptance by orthodox researchers [1] that CFS is not a psychiatric illness but a physical illness triggered by a virus, usually Herpes viruses, such as EBV (Epstein-Barr virus), CMV (Cytomegalo virus) and HHV-6. These viruses compete with serotonin for receptors [2], which explains why serotonin re-uptake inhibitors (SSRI’s) are prescribed as medication. BICOM practitioners generally agree with this viral explanation but also believe that multiple allergies play a major role by overloading the immune system. We must remember that orthodox scientists often hope to find a single cause of a disease, whereas BICOM practitioners treat each patient as an individual and expect a multiplicity of factors contributing to his/her conditionin addition to the triggering Herpes virus – the ‘overflowing barrel’ you are all familiar with. Some factors will be specific to an individual patient but some will also be specific to their geographical location. The purpose of this paper is to suggest both individual and geographical factors that therapists might look for to increase the success of their therapy. Our success rates with difficult cases have improved recently after incorporating into our practice the biochemical principles described in the publications [3, 4] of Dr Igor Tabrizian, a general practitioner from Perth, Western Australia. He began developing his approach after finding patients improved with supplements of minerals that were deficient in local soil. He explains why blood analysis is useless as an indicator of mineral deficiency and explains the need for tissue analysis, advocating hair analysis by mass spectrometry as a painless method. In
his words, “Patient’s problems are in their tissues, not their blood”. In this paper, we are only using the part of his approach that relates to CFS/Fibromyalgia but we feel BICOM therapists would find his books useful. His alternative, nutritional medicine model for CFS, which we combine with BICOM therapy, proposes three contributors to the illness:
• Nutritional disturbance • Digestion
A summary of the proposed mechanism is that the illness begins with the infection, but there is a lack of immune nutrients to fight the infection, and it moves in to an unresolved, chronic phase. Nutrients may not only be deficient in the diet but also their uptake may be blocked and so the illness is prolonged. Key nutrients linked to the symptoms of fatigue and muscle pain are iron and magnesium. Poor digestion means these key nutrients are poorly absorbed. We find BICOM therapy is useful in all three areas. We use the B13 model BICOM 2000 device with spin tester and impulse generator. ME/CFS RESEARCH SUMMARY
ME/CFS has been formally classified as a neurological disorder by the World Health Organisation. Its diagnosis [1] includes clinical syndromes linked to infectious agents such as Herpes viruses, Ross River virus, Q fever, Lyme disease and exposure to toxic chemicals such as pesticides. At a CFS conference in Adelaide, the research position was summarised by the keynote speaker, Prof. Kenny De Meirleir of the Free University of Brussels. His clinic sees 800 CFS patients every three months, from many countries in Europe. He has developed a set of six laboratory tests, which allows him to classify CFS patients into three groups. These are too complicated to detail here but using these tests, he was able to predict their symptoms before they were seen clinically in about 95% of the cases. Group 1, about 20% of cases, tends to have a multiple sclerosis type picture. Pain is not a strong feature. They are associated with viruses, pesticides and heavy metals. Group 2, about 60% of cases, has pain as a predominant feature. The pain is generalised and does not follow nerve root distribution and is often triggered by exercise. It includes headaches, and generalised myalgia and arthralgia. Group 3, about 15% of cases, are severely ill. They usually have severe bowel problems and are living in survival mode. In 58% of cases, they responded to treatment with antibiotics followed by probiotics. INFECTIONS
A major ‘local factor’, for us equally as important as the Herpes viruses, is infectious disease from insect bites. Mosquito-borne Diseases Examples are Ross River Fever and Dengue Fever, viruses spread by mosquitoes, which are well known to doctors in Australia. However, these are only the tip of the iceberg. We test for 13 mosquito-borne viruses which have migrating birds and both wild and farm animals as intermediate hosts. These are also spread by air travel. They are common in Asia and Africa as well as Australia and belong to the families Alphavirus, Flavivirus and Bunyavirus. The West Nile Virus (a Flavivirus) is also a problem in North America. A Bunyavirus (Toscana virus)
causes sandfly fever in the Mediterranean region (Italy, Portugal, Spain, and Cyprus). At campsites near lakes, official warning notices state that there is no cure for these diseases and advise prevention by spraying the skin with chemical insect repellents. Symptoms are fatigue, polymyalgia and polyarthralgia. On our first holiday after coming to Australia, we took a tourist trip advertised as “see koalas going to bed in their trees”. This was in a swamp, at dusk. Five to ten days later, we had these symptoms. Fortunately, we quickly recovered after BICOM treatment. _____________________________________________________________________________
Alphavirus Flavivirus (related to Yellow Fever, Dengue and Hepatitis C)
• Japanese Encephalitis (Northern Australia, Asia, Oceania)
Bunyavirus
• Trubanaman (South Eastern Australia)
_____________________________________________________________________________ In our clinic, we always test anyone presenting with these symptoms for mosquito-borne viruses as well as the Herpes viruses. Some patients are surprisingly symptom-free after only three or four treatments at weekly intervals. This includes people who have been unable to work for 3 - 15 months before treatment. These are physically active, outdoor workers whom we generally find respond much faster to all BICOM treatment than office workers. Perhaps there is a lesson here for all of us to take more exercise?
Rickettsial and Other Intracellular Pathogens If there is still general pain as well as fatigue, we next look for Rickettsial infection, as this is common in our region. Rickettsial fevers have afflicted armies since the Middle Ages. Epidemic typhus fever (transmitted by lice) contributed significantly to the loss of life during Napoleon’s retreat from Moscow in 1812. The following quotation from an Australian Defence Force publication shows that this is as much a problem today. “Although it has been claimed that “the jungle is neutral”, the Australian bush is a potentially hostile environment and visitors can contract a range of serious illnesses. In March and April 2005, 22 soldiers contracted typhus while training in a coastal area of North Queensland.”
Infection is believed to be caused by a bite from a tick, mite, louse, sand fly or flea. Wild birds carry infected fleas to areas hundreds or thousands of kilometres from the infected mammal, rodent or lizard. Humans cannot pass the Rickettsia to each other. Cecile Jadin from South
Africa was the first to document the link between chronic Rickettsial infections and CFS/Fibromyalgia. In 3,600 patients she found the commonest symptoms were fatigue, myalgia and arthralgia, the same as for mosquito-borne viral infections. She believes Rickettsial disease may also be transmitted by inhalation, ingestion or contamination of abrasions or cuts.
A study by John Graham of Flinders University, Adelaide, found Rickettsia in 337 out of 611 CFS cases. Rickettsias are bacteria – not viruses and so can be killed by antibiotics. However, because they can go dormant, the normal medical treatment is to give antibiotics for 18 months, which many patients wish to avoid. The body does not seem to be able to recognize them accurately enough to make specific antibodies. They live in the cells that make up blood vessel walls (the endothelium & the smooth muscle cells) and have developed special mechanisms to steal energy from the host cell. Rickettsias can be dormant for years and each colony can have a different life cycle – so different symptoms, different parts of the body can be affected each time, making it very difficult to associate the outbreaks with a common causative agent.
___________________________________________________________________________
Rickettsial Antibodies tested in Australian Laboratories
Spotted Fever Group
• R. australis - Queensland tick typhus (Eastern Australia)
• R. honei - Flinders Island spotted fever (Southern Australia)
• R. conorii - Mediterranean spotted fever (Southern Europe, Africa, Asia)
• R. sibirica - North Asian tick typhus (Asia)
• R. rickettsii - Rocky Mountain spotted fever (Americas)
• R. akari – Rickettsial pox ( USA, Ukraine, Slovenia)
Typhus Group
• R. typhi – Murine typhus (worldwide)
• R. prowazekii – Epidemic typhus (worldwide)
Scrub Typhus Group
• R. (orientia) tsutsugamushi (Asia, Australia, Pacific)
o Gilliam scrub o Karp scrub o Kato scrub o Litchfield scrub
__________________________________________________________
The other intracellular pathogens we test for are Mycoplasma, Q fever (Coxiella burnetii) and Lyme disease (Borrelia burgdorferi), alone and in combination with the Herpes viruses. Although not infections, toxins from spider bites will also lower the immune system. Although we are unaware of statistics, at a conference for victims of spider bites, many reported a spider bite as being the trigger for their chronic fatigue. Venomous species in Australia are the White-
tail, the Redback and the Sydney Funnel Web. Local patients will generally know if they have been bitten by a venomous spider and will be able to identify it. This will not be the case with tourists. A spider bite shows as two small red dots from the pair of fangs. Therapists in Australia catch spiders and keep the dried specimens in vials for treatment. BICOM treatment using the dead spider is effective. An Adelaide BICOM therapist was bitten by a White Tail the day before her wedding, refused to cancel her honeymoon and took the BICOM with her for daily treatments. Another source of infection is vaccinations. In our experience, this is rare but we have had a few teenage girls having to stay off school for weeks with fatigue following Hepatitis B vaccinations which are given routinely at age 15. NUTRITIONAL DISTURBANCE There are two factors to consider with nutritional disturbance: either the nutrient is not there or it is ineffective because something is blocking its use. Deficiency The CFS patient must have sufficient immune nutrients to fight infections. One obvious nutritional factor is mineral deficiency. If the soil in your area is deficient in particular minerals, then so will be the food your patients are eating and this may be contributing to their symptoms. It is estimated [6] that 740 million people worldwide are iodine deficient so many people have an under-active thyroid, a well-known cause of fatigue. A German study [7] has also linked under- active thyroid to fibromyalgia. The Alps, Himalayas and the Ganges valley are severely deficient. Within Australasia, Tasmania and New Zealand are highly deficient because of their mountainous terrain and high rainfall. Other areas are the Adelaide Hills, the Atherton Tablelands, the Great Dividing Range, Eastern Victoria and the plains around Canberra. This is reflected in the high proportion of our patients taking thyroxine supplements. Australian research [8] showed that the diets of 67% of men and 85% of women were below the RDA for zinc and 50% of men and 39% of women were below the RDA for magnesium. Zinc and selenium are important nutrients for the thyroid. Without adequate selenium, the inactive T4 hormone, thyroxine (the one prescribed by doctors), cannot be converted into the active T3 form. Many parts of the world have selenium deficient soils, and, according to Cabot and Jasinska[6], in Australia, “it is almost impossible to obtain an adequate amount of selenium from diet alone”. Some viruses, including Herpes viruses, deplete selenium, as selenoproteins are needed for viral replication. We have also found parasites testing with selenium. Yet up until a few years ago, selenium supplements were banned from sale in this country. Deficiency of magnesium will contribute to muscle pain and also fatigue as magnesium is required for ATP production. Deficiency is tested using an A program such as 192, but often we find a mineral that is deficient also tests as a strain with an Ai program. We interpret this as meaning that the body sees the mineral as an ‘enemy’, and so we must treat it first as a strain using an Ai (998) or H+Di (977) program before the patient can absorb it. Common examples are magnesium and zinc. Anti-nutrients These are metals that, in excess, will block metabolic pathways and prevent proper use of nutrients. This will happen at levels below what is conventionally regarded as ‘toxic’. Nutritional supplements will be less effective, if their uptake and metabolism is being blocked by these anti- nutrients. Major anti-nutrients are copper, aluminium, lead, mercury and cadmium. These will test as strains with an Ai program on the BICOM but often need the impulse generator and/or a Kurzbak test [10]. Anti-nutrient – Nutrient Combinations Anti-nutrient Nutrients
blocks Magnesium, Iron, Zinc, Molybdenum, Manganese,
Aluminium blocks
blocks Calcium, Iron, Zinc, Chromium, Molybdenum
Cadmium blocks
Two minerals related to the symptoms of CFS are iron and magnesium. Both iron and magnesium are blocked by excess copper, which does not show in a blood test. Only a hair analysis, or a bioenergetic test will show this. Tabrizian proposes that copper excess is a major cause of fatigue and the commonest cause of iron deficiency [4]. By blocking zinc, it causes low stomach acid and blocks the transfer of iron across the intestinal wall. Once inside the cells, copper blocks the action of iron in the mitochondria to produce energy and blocks carnitine production which leads to poor muscle function with pain and fatigue. This is highly significant for us because South Australia is a copper mining area but also, copper fungicides are widely used in the wine industry and to suppress algae in water reservoirs. Vineyards are often located close to residential areas. Specific Blocking of Nutrients Needed for Energy
It is important to note that often the main problem is not excess copper in the diet but retention of copper in the body. Sufficient zinc and molybdenum will prevent too much copper being absorbed but xenoestrogens, such as pesticides, PCBs, plastics and medications such as oral contraceptives and oestrogen-HRT will block the body’s ability to excrete copper. In our
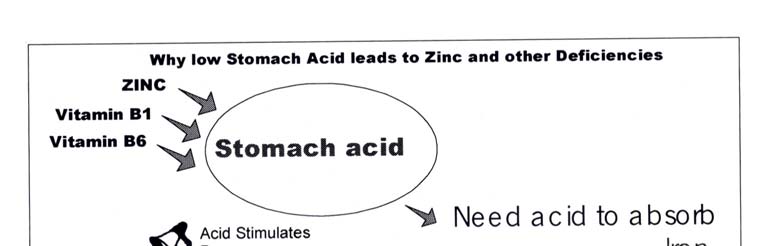
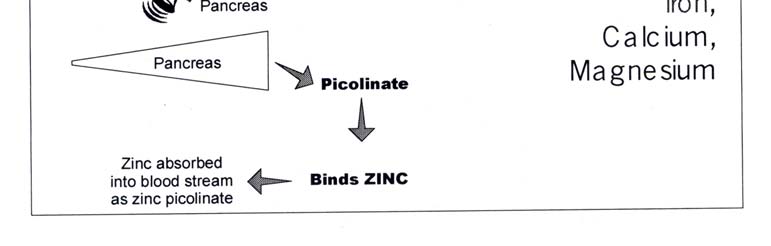
experience, a normal EAP test rarely shows copper excess as a strain. More often, to detect the copper it is necessary to use a Kurzbak test, often on the liver, head or thyroid, after using the impulse generator. Once it has been found, copper can be eliminated as normal with the BICOM, using Ai programs such as 998, 971, 197 and 979. Supplements such as chlorella, MSM and cysteine as well as zinc, molybdenum and vitamin C will help to speed up this process. A proprietary product called Molyzinc is sold to overcome copper retention, and contains 5mg zinc, 100µg molybdenum, and 100mg vitamin C. Where xenoestrogens are found, these should be eliminated also. Both xenoestrogens and metals may be associated with parasites and it may be necessary to test these symbiotically, in other words with all vials in the input beaker together[9] or with the parasite vial in the input beaker and the xenoestrogens and metals in the spin tester on left spin [5]. Note that parasites do not only absorb toxic metals, they also absorb beneficial minerals. We often think of parasites ‘stealing our food’ but we have found cases where they are stealing minerals that are already deficient in the diet, such as selenium, molybdenum, magnesium, zinc and chromium – the ones we can least afford to lose. Throughout Australia, the soil is deficient in phosphorous and large quantities of ‘superphosphate’ fertiliser are used. This contains 20mg per kg of cadmium as an unavoidable impurity so food is contaminated with cadmium, which then blocks zinc, magnesium and selenium metabolism. Cadmium and mercury are members of the “zinc series” of the periodic table of elements. Because of this similarity in atomic structure, plant and animal biological systems will readily substitute these toxic metals for zinc in biochemical processes. DIGESTION Imbalance of intestinal flora, gastrointestinal infections, and malabsorption are all factors which weaken the CFS patient. Richard Schloeffel, a Sydney physician who has specialised in CFS for 24 years, reports that his worst cases have major gastrointestinal problems. This is an area where BICOM therapy excels, by treating food allergies, mycoses and parasites. As this audience is familiar with these treatments, we do not need to discuss them. Zinc is the mineral of major importance for digestion. It is needed to make stomach acid to help absorb iron, magnesium, calcium and amino acids. When the stomach makes acid, it sends a message to the pancreas to release digestive enzymes to digest proteins. Stomach acid protects us against pathogens such as Candida and creates an environment favourable to beneficial bacteria such as Acidophilus – its name means “acid loving”. So treatment for Candida should include not only a low-sugar diet, anti-fungal remedies and BICOM therapy with an Ai program but also supplements of zinc, with vitamins B1 and B6, to increase stomach acid. Zinc has anti-viral, anti- bacterial and anti-fungal properties and is contained in the mucus layer that protects the stomach lining from being digested by the acid. Zinc is also needed for repair of damage to the intestinal wall. As discussed earlier, lack of zinc may be due to deficiency in the diet or blockage by the toxic metals, mercury, cadmium and copper. Zinc often tests as a strain, and we treat this early to enable it to be absorbed when the patient takes supplements, which is essential in Australia. Of course we must first treat the toxic metals blocking the zinc. Vitamin B12 ‘intrinsic factor’ is produced in the stomach and is necessary for absorption of the vitamin. Malabsorption causes anaemia and hence fatigue. We have found a small number of patients with an allergy to the intrinsic factor and also to the cobalt contained in the B12. PROCEDURES When new patients make a booking, we send them two questionnaires. One asks for information on lifestyle, health history and environmental factors. The other is a list of symptoms. They are asked to put a tick next to the symptoms they have before coming for BICOM treatment. This is valuable for monitoring progress with chronically ill patients who may have many symptoms. If, after several visits, they tell you “I don’t feel any different”, you can go through the list of symptoms and find how many have gone away, or at least improved. Often they will have forgotten that they had these symptoms in the first place. This then increases confidence for both the patient, and, you, the therapist. Our first visit protocol is essentially the same for all patients. This is detailed in our 2005 BICOM Congress paper [12]. In a standard 90-minute appointment, we do a full EAP reading and test and treat energetic blockages such as chakras, geopathy/radiation, scars and run the 133 program with input from both feet to balance the meridian system. We then test as many strains as time will allow, starting with the ones we expect from the information on the patient questionnaire as well as central foods. If we have the luxury of a 2-hour appointment, we follow the treatment of blockages with a diagnosis using the Regumed KTT Five-element test kit. We also use this when the information on the questionnaire suggests we are dealing with a difficult case or when it is a referral from another practitioner, because then it must be a difficult case! We are really impressed with the ability of the Five Element testing to pinpoint the priority strain(s) as chemical, viral, bacterial, heavy metal or intercellular strain. This lets us identify the major strains and start treatment in the priority area. We then wait until later sessions for testing of other strains which we assume to be less important. Simple Cases In many cases, we find the patient will obtain quick relief within three or four visits after treating Herpes viruses, mosquito viruses, central allergens and any metals that test with a simple EAP meridian test. If we find there is only limited improvement in the symptoms of energy and pain after these treatments, we know we are dealing with a more complex case and we look for other strains. If pain has gone from the upper body but remains in the lower legs, we suspect carbohydrate intolerance. This is also indicated by a quadrant measurement with a low reading on the left foot. We use a vial of glucose as an indicator of carbohydrate intolerance as glucose is the end product of carbohydrate metabolism. We test for glucose and insulin as strains (Ai program). This may need unmasking with a low glycemic index diet for four days followed by eating something sweet, like a doughnut or cake, 60-90 minutes before the appointment [10].
Allergy treatment, with program 998 initially and 977 during follow up sessions, for glucose and insulin appears to boost the immune system and we often find that minor allergens no longer test after this treatment. Because of this we now test glucose as a central allergen. We advise the patient that 25% of the Australian population is estimated to have hyperinsulinia and that it would be wise to keep on a low to medium glycemic index diet permanently because BICOM treatment of glucose is not a long-lasting treatment like that for wheat or cow’s milk. It does remove the craving for carbohydrates and helps the patient to control their diet. We recommend repeating the treatment every six months. Since learning about the symbiotic relationships between foods and molds [5], we now re-test and treat central foods with the appropriate molds. The pairs we most often find in our area are:
It should be noted that Zearelenone is a highly oestrogenic mold and will contribute to oestrogen dominance symptoms. Salicylate is a common allergy in Australia due to a Mediterranean type diet combined with low zinc / low stomach acid which impairs digestion of salicylates. Difficult Cases Here we expect to find nutritional and digestive problems with strains such as metals/minerals, fungi/molds, parasites, Rickettsia, Mycoplasma, Lyme disease, or Q Fever. Chemical overload may also be a factor. The toxic metals acting as ‘anti-nutrients’ are often hidden, because they are localised in a particular organ or inside a parasite. We used to test for these after using a provocation with an ‘A’ program (196 or 972) but we now use the Regumed Impulse Generator at 3.6Hz for two minutes as this is much quicker. We also use the Kurzbak test with the ‘hammer’ electrode held on a likely organ such as the liver, head, pancreas or thyroid to find which area gives the highest Ai value. Both toxic metals and nutrient minerals may test symbiotically with a parasite. Chemicals may also be a factor, depending on where the patient lives now, or has lived in the past and on what jobs they have held. These also have to be tested symbiotically with parasites. If copper tests positive, it is essential to test for xenoestrogens because these promote copper retention. If patients work with chemicals, for example farmers, building workers and beauty technicians, then we ask them to bring samples of these chemicals. Rickettsial infections are the most common after Herpes and mosquito viruses. These tend to be long lasting and progress can be slow. The main symptom is constant pain. Rickettsias can be anywhere there is a blood vessel and there are usually multiple colonies throughout the body. They prefer muscle, thyroid, bowel, lung, heart, throat, skin and pancreas blood vessels, so these are potential places to test using the Kurzbak method [10]. If Rickettsias do not test on a meridian with EAP, we ask the patient where the pain is greatest and test on that area with the Kurzbak method. In our current practice, we actually use the Impulse Generator first and then test using the Spin Tester [5] with one vial in the input beaker and the other in the spin tester. After Rickettsias no longer test at any amplification, it is necessary to provoke them to continue treatment. Since we began using the Spin Tester and Impulse Generator combination [5], we have made better progress. When the pain is in the neck and shoulder areas, we often find a symbiotic relationship between the Rickettsia and a Herpes virus (EBV or CMV). By this, we mean there is only a positive test using an Ai program when vials of both pathogens are in the input beaker at the same time. To find the focus we use a Kurzbak test and move the hammer electrode until we
find the place that gives the highest Ai value. Often the patient can pinpoint the most painful spot to test on. We must admit that we have a few CFS patients with Rickettsias who have been coming for several years. We get disappointed that we are not able to help them more and ask if they feel it is worth continuing. They always say they feel the treatment is helping even if the improvement is short–lived. When we use the symptoms sheet, we find that many of the symptoms have gone away. Unfortunately, the one that keeps coming back is pain. A recent finding has been Kurzbak testing for central foods on the thyroid. Many patients whom we believed to be completely treated for food allergies still tested for foods on the thyroid. Gluten is a common one. Summary of Factors Herpes viruses, mosquito viruses Central foods, carbohydrate intolerance Toxic metals – copper, mercury, cadmium, aluminium, lead Deficiencies – iron, magnesium, zinc, selenium, molybdenum, iodine Fungi and molds Chemicals – especially xenoestrogens Parasites Rickettsia, Mycoplasma, Q-fever, Lyme disease Allergy to B12 intrinsic factor Vaccinations CASES FROM OUR RECORDS Fifty patient records were taken at random for patients with CFS/Fibromyalgia symptoms who had been seen sometime during the past three years. As our procedures have changed over this time in the light of new information, this cannot be taken as a scientific study. However, it does give an indication of the most common strains found and their frequency of occurrence. This selection included 14 males and 36 females born between 1940 and 1992. _______________________________________________________________________ Strain Percentage positive Mosquito
------------------------------------------------------------------------------------------- Mosquito + Herpes
________________________________________________________________________ The following are some case histories to illustrate some of the points made in this paper.
Case 1 Male born 1959 (Simple Case) Outdoor construction worker who has a weekend holiday shack at the River Murray, the largest river in Australia. Complained of pain in joints and muscles plus lethargy. Self-employed and unable to work for 4 months. He was sceptical but desperate to get back to work and a neighbour had recommended BICOM. First visit April 2002. This was a short ‘first aid’ visit and limited testing showed Barmah Forrest virus, EBV, Aspergillus Flavus mold and cow’s milk allergy. Barmah Forest was the priority and was treated in the first appointment and he was told to abstain from cow’s milk. One week later he came back and reported “a dramatic improvement in joint pain”. He had been able to work for two days that week. The Barmah Forrest treatment was repeated and the other strains were treated for the first time. The following visit he told us he was now working full time. We tested all four strains and gave a final treatment. We explained about total body load and how there might be more treatments needed to achieve optimum health. However, he felt the treatment had been fantastic and that was all he needed. He was now a convert. Two year’s later (June 2004) he came back. He had been well but was starting to get pain in his ankles. His GP could not find anything. This time we found Kunjin and Edge Hill (both flaviviruses) and the EBV had re-activated. We found gluten allergy because we were now using Kurzbak testing. These strains were treated and he was well for another 15 months. This time (September 2005) his doctor thought it was “post Q Fever syndrome”. By now we were using symbiotic testing with the spin tester and we found a positive test with Q Fever on right spin and the EBV vial in the input beaker. We treated this successfully and the pain went away. As he works outdoors and holidays by the river, he cannot avoid being bitten by insects. We explained that he needed to boost his immune system. In recent treatments we have been using thymus activation program 428. We also treated carbohydrate intolerance using the glucose vial. Case 2Male born 1970 (Simple Case) Former footballer, had to retire after several knee injuries and operations. Now a football recruiting manager. Still exercises regularly. Came with joint and muscle pain and fatigue which he felt had developed over many years. He felt he had a problem with cow’s milk. First visit August 2006. Normal first visit procedure. Blockages treated were solar plexus chakra and scars to both knees. Testing revealed cow’s milk, wheat, Murray Valley Encephalitis (MVE) and Trubanaman viruses but no obvious Herpes viruses. No metals with normal testing. Very few strains were testing so we treated viruses in the first visit to give relief. At the second visit, one week later, he reported feeling good on the day of treatment and that he had slept well. However, 24 hours later he had a nervous reaction from his scalp to jaw line and broke out in cold sores on his lips. We tested herpes viruses again and found that a herpes simplex virus had reactivated. This was treated along with the mosquito viruses, cow’s milk and wheat and the session finished with an individualised toxin release program 970. The third week he reported that the cold sores (Herpes simplex) on the lip had dried up 24 hours after the treatment but he had felt tired that day. He had noticed some reduction in the pain. This session we tested foods with molds and found milk testing symbiotically at a higher
amplification with Geotrichum Candidum. All strains were tested and programs run with the new Ai or Di values. This time a liver activation program 430 tested as being needed. At the fourth and final session he said he felt “great and absolutely fantastic”. Because he was thinking clearly and had no pain anywhere he had considered cancelling this visit. The Impulse Generator was used followed by Kurzbak testing. No metals were found, wheat was no longer a strain, milk was at Ai = 2 with Geotrichum Candidum, MVE was at Ai = 1 and Trubanaman was at Ai = 4. He was impressed and wondered how he could persuade the football team to have BICOM as about half the players handed their asthma ‘puffers’ to the coach before a match. Case 3Female, born 1972 (Moderate Difficulty) First visit April 2006. Moved to Adelaide from a tropical area of Australia where she had been introduced to BICOM treatment. Extreme fatigue, dizziness even when lying down, migraine, irregular heart beat, pale complexion. Illness began “years ago” after contracting a virus on an island in Queensland. Doctor had diagnosed a mosquito virus but was unable to say which one. Previous history of glandular fever in her early twenties and recalled being bitten by a redback spider when young also. First visit was a short, ‘first aid’ one. EAP showed high liver and spleen readings. The only treatment this session was stabilisation using a modified version of our ‘self- regulation’ protocol [11] with 507 (yin-yang balance) in place of the dry injection of flower essences. So this meant the series of individualised programs 535, 133 and 507. Electrode placement for 535 and 133 was as for “laterality” in the BICOM manual. One week later, Five Element testing showed Wood as the primary cause, drawing energy from all other elements. Water was the ‘middleman’ drawing energy only from Fire. Further testing showed the Wood problem to be located on the LIV and FD meridians, with viral and heavy metal strains. The metals were found to be copper and nickel; the viruses were Kunjin and Trubanaman. The strain on Water was allergy. After two treatment sessions for the metals and viruses she felt “better in the head, not dizzy”, the fatigue was less and the heart palpitations had gone. Heavy metal treatment continued for two more sessions and allergies were found and treated for gluten, cow’s milk, yeast and tyramine over five sessions. When food allergies were testing at lower amplifications, foods were then tested symbiotically with molds. Milk was found with Geotrichum candidum. Two foods which had not tested alone were now found to test with molds: salicylate with Zearelenone and cashew nuts with Aspergillus Flavus and Aflatoxin. The food/mold combinations tested stronger with a Kurzbak test on the ear. Milk was also testing at low amplification with Penicillin Roqufortii. In November, 2006 after 11 visits, she had colour in her face and friends had commented how well she looked. She had organised a dinner party, had not felt tired or dizzy and was able to eat everything. By January 2007 she has had 13 treatments and wants to continue with maintenance treatments but clearly is over the worst of her problems. Case 4Female Born 1964 (Difficult Case) Manager/Owner of an airfreight business. Extreme tiredness, sore muscles, dizziness and mental confusion but has to keep going all day because she is the boss. Collapses in a chair when she gets home. Tries to exercise but this makes symptoms worse. Became ill during a world trip in May 2005 when she was given antibiotics and has never been well since. She did see a medical CFS specialist but was “not impressed”. He believed the problem was “slow blood flow to the brain”. Also saw an ENT specialist, Gastroenterologist and Sports Medicine specialist and the Professor at the Balance and Dizziness Disorders Centre who diagnosed vestibular neuritis and gave balance exercises for 5 weeks. First visit was in May 2006, one year after the problem started. We used the Impulse Generator, Spin Tester and Kurzbak testing throughout treatment of this patient along with symbiotic
testing. Without these new approaches, we would probably not have been able to help this patient regain a normal life. The following has taken 16 visits. We found major problems with molds and fungi – nine of these tested, probably the link to the problem starting with the antibiotics. Copper metal tested as a strain, the worst possible metal according to the Tabrizian model. Central foods were wheat, milk, salicylate and sugars. Herpes viruses, CMV and EBV, were found and three mosquito viruses, MVE, Sindbis and Trubanaman, also Streptococcus. The parasite Ascaris was found testing with milk and Eurytrema Pancreaticum tested with wheat, glucose, Candida Albicans, Candida Glabrata, Candida Parapsilosis, and Mucor Mucedo. Outdoor molds, Helminthosporium, Alternaria and Cladosporium tested symbiotically with glucose. She did have some bad reactions following early treatment sessions, but she had a positive attitude and gave us accurate feedback on how she felt which helped. After the fourth visit she felt she “had the best day in ages”. Then the dizziness got worse after the fifth visit but was better again after the sixth visit when she also noticed more energy. After the seventh visit she had enough energy to clean the whole house. She also kept giving us feedback such as “tingling in the right ear, pain located in the upper spine”, which helped us to test with the Kurzbak method. After the tenth visit, the sugar craving had gone and she felt we were 80% there on energy. After 15 treatments she cut the lawn grass without any hayfever, the dizziness had gone and the fatigue was 90% gone. There is still a little pain in the back of the neck but the EBV treatment is not yet completely finished. We expect a complete recovery in two more treatments. This is at January 2007. Case 5 Male born 1988 (Moderate Difficulty) First visit November 2003, when he was 15 years old. Constant tiredness, aches and pains. He has been diagnosed with Rickettsia by a doctor who wanted him to have long-term antibiotics. He wanted to avoid this and so came for BICOM treatment. He tested positive to Rickettsial Pox and Flinders Island Spotted Fever as well as EBV, CMV and Influenza viruses. Other strains were magnesium, gluten, lactose, yeast, Candida Crusei, glucose, fructose and insulin. After nine treatments, none of these strains were testing and on March 22nd 2004 he reported feeling lots better with only one day off school that year. From late March to October 2004, he visited us for treatment with the ‘self-regulation’ series of programs to help him study for his exams at school. He continued to do well apart from occasional ENT infections which were quickly treated. In February, 2005 he came with an ear infection and a sore throat and said things were going well but he was starting to get tired again. In addition to the Staphylococcus infection on the ear we found Rickettsia testing positively but only in a symbiotic relationship with Candida Crusei using a Kurzbak test on the liver. This was resolved with three treatment sessions and he had been fine since. Case 6 Female, born 1940 (Difficult Long-term Case) February 2000 – November 2001 First came to see us in February 2000. Fatigue, muscle pain and irritable bowel. Diagnosed by a rheumatologist with CFS/Fibromyalgia. Medication prescribed is Zoloft and Methatrexate. Symptoms started after a difficult labour with her son 32 years ago. Numerous operations and injuries. Had glandular fever many years ago. Initially treated for scars, electrosmog (702) and standard BICOM treatment of numerous strains aimed at reducing total body load. Treatment helped the bowel problem and reduced the muscle pain. After three months, her naturopath reported that live blood microscopy showed less clumping and that oxygen levels were improved. Treatment continued at greater intervals, helping to manage symptoms but not getting a big breakthrough. Gap in treatment from November 2001 to February 2003. February 2003 – January 2005 During this period we began to provoke hidden strains, use Kurzbak testing and look for parasites in symbiotic relationship with metals and chemicals. We found a strain from the metals amalgam, chromium and zinc, using provocation with an ‘A’ program, and a Kokobera mosquito virus. We treated carbohydrate intolerance. Five Element testing (old set, not KTT) showed hormonal allergy and we found thyroid hormones testing as strains. We found the pancreatic fluke (Eurytrema), Trichinella and Toxoplasma testing with mercury , copper and gold. We treated these by BICOM and also the Hulda Clark herbal treatment. We first tested the Clark herbs to make sure she was not allergic to them. She had a short-lived negative reaction of nausea, losing hair, and pimples. After seven treatments, the parasites and metals were no longer testing and she reported that her muscles felt good and she no longer had to take magnesium supplements. We now know that this is probably because the copper had been blocking magnesium uptake, but at this time we were not aware of the importance of copper. Gap in treatment from January 2005 to November 2006. November 2006 – January 2007 Having learned about the spin tester, impulse generator and symbiotic testing at the 2005 Fulda Congress, we were now able to take treatment further. We found one relationship between Fasciola Hepatica, Toxoplasma, copper and lactic acid testing both on the liver and thyroid and another between glucose, Candida Albicans and Candida Glabrata testing on the colon. We recommended supplements of zinc, selenium, magnesium and vitamin C to help overcome the copper overload and support the thyroid. After the first treatment she had a negative reaction in the colon, but after three more treatments, she was thinking more clearly, the pain was much reduced and she reported having “much more energy, getting lots of things done”. She was about to help her son paint his apartment. If only we had known at the beginning of treatment in February 2000, what we know now, we would have made faster progress and saved this patient having to have so many treatments. Clearly we have now made significant progress but we will have to support the immune system in future sessions. CONCLUSION BICOM therapy can be a powerful tool in the treatment of CFS/Fibromyalgia. Treatment of allergies and viruses is straightforward and usually brings quick relief of symptoms. Many factors can be involved in this condition, some individual to the patient and some common to the locality in which you have your practice. Identifying these common factors can save you time when testing for strains and can result in patients getting better with fewer treatments. Some factors are, however, more difficult to overcome. The example given in Case 6 above, applies to many other cases and shows the benefit of continuing education and sharing of information to continually improve the standard of BICOM treatment available worldwide.
REFERENCES
1]
Prof. Kenny De Meirleir, keynote speaker at ME/CFS Research Forum, a two-day workshop of leading CFS researchers and clinicians at the University of Adelaide on June 3-4, 2005.
Candace B. Pert, Molecules of Emotion, Simon and Schuster, New York, 1999. ISBN 0-684-84634-9
Igor Tabrizian Nutritional Medicine – Fact and Fiction.Visual Textbook of Nutritional Medicine NRS Publications.
Alan E. Baklayan Workshop-Intracellular Strains. BICOM Congress Fulda, 2005
Sandra Cabot and Margaret Jasinska Your Thyroid Problems Solved WHYS, Camden, NSW, 2006. ISBN 0-9757436-4-3
W. Riedel, H Layka, G Neeck. Rheumatol.1998; 57 Suppl 2:81-87 Zinc and Magnesium Status of Australian Adults Nutrition Research,
1991, 11, 23-32
Martin Keymer and Alan E. Baklayan, BICOM Congress, Fulda 1998
Alan E. Baklayan, Kurzbak. BICOM Congress RTI 23 (1999), 101-103 and 28 (2004) 10.
For more details see BICOM Congress RTI 29 (2005), 25.
BICOM Congress RTI 29 (2005), 23-24
4x4 Voyager Kit List The Woodland Ways 4x4 Voyager course is designed to give you off road driving techniques and experience, as well as an outline understanding of what it takes to survive in the wild- using your vehicle as your survival resource. The course will give you the hands on experience, and the confidence, to utilise your knowledge around off road driving techniques and the
 PROCEDURES
PROCEDURES