Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Parasitophil.comoj.com
Am. J. Trop. Med. Hyg., 70(6), 2004, pp. 635–637
Copyright 2004 by The American Society of Tropical Medicine and Hygiene
SHORT REPORT: HIGH PREVALENCE OF MULTIDRUG-RESISTANT PLASMODIUMFALCIPARUM MALARIA IN THE FRENCH TERRITORY OF MAYOTTE
FRANC¸OIS PETTINELLI, MARIE-EDITH PETTINELLI, PHILIPPE ELDIN DE PE´COULAS, JULIE MILLET,
DELPHINE MICHEL, PHILIPPE BRASSEUR, AND PIERRE DRUILHE
Centre Hospitalier de Mayotte, Mamoudzou, Mayotte; Faculté de Médecine, Rouen, France; Unité de Parasitologie Bio-Médicale,Abstract. A drug-resistance survey was conducted in the French territory of Mayotte in the Comorian Islands in the
Indian Ocean where malaria is endemic. A high prevalence of resistant Plasmodium falciparum parasites was observed,
not only to chloroquine (88%) and pyrimethamine (99%), but more surprisingly to quinine (17%), mefloquine (9%),
and amodiaquine (24%). This leaves few treatment alternatives other than artemisine-mefloquine combinations. How-
ever, despite notification to French Health authorities three years ago, inadequate treatment (chloroquine plus sulfa-
doxine-pyrimethamine) is still used in this locality. Thus, people still die of malaria in this remote territory of France.
The island of Mayotte in the Comorian Islands in the In-
double-site enzyme-linked LDH immunodetection (DELI)
dian Ocean is in an unusual situation because from an epide-
test.2 The correspondence between results obtained with
miologic and sociologic point of view, it is an African-like
the DELI assay and the classic isotopic microtest has been
setting, yet it benefits from the French health system with
previously established using laboratory-adapted strains2 and
diagnosis and treatment facilities that are of much higher
field isolates in Senegal,3 Burkina Faso,4 and Asia (Brasseur
standards than those in Africa. However, the population of
P, Druilhe P, unpublished data). Two strains of P. falciparum
Mayotte is of east African origin and lives in modest housing,
(3D7 and Palo Alto) were used as internal controls.
including huts along rare roads in a forested landscape. In
The in vitro drug sensitivities of 132 isolates that were suc-
contrast, since 1975 when Mayotte decided to remain a
cessfully cultured are shown in Figure 1. We observed an
French territory, a sophisticated health system has been
extremely high prevalence (88%) and an extremely high de-
implemented. This includes a modern, well-equipped central
gree of resistance to chloroquine, which is consistent with the
hospital, and numerous dispensaries run by doctors who de-
clinical failures reported by rural dispensaries and the in-
liver free medical care. This, along with other factors, has con-
crease in the number of cases referred to the hospital. The
tributed to massive immigration from other Comorian islands.
results also showed a substantial number (17%) of isolates
Malaria has always been prevalent in this region and has
resistant to quinine with high IC50 values (> 500 nM), which
not been decreased by vector control. Until 2001, treatment
may explain the fatality rate recently observed in the hospital
relied on classic schemes, i.e., chloroquine for acute uncom-
despite rapid infusions of quinine and adequate intensive
plicated cases and parenteral quinine together with adequate
care. Most likely as a consequence of quinine resistance, 9%
nursing for complicated cases. The increasing number of ma-
of the isolates were found resistant to mefloquine, despite
laria fatalities, particularly among cases properly handled in
the rare use of this drug. This finding is consistent with pre-
the central hospital, led us to initiate a drug sensitivity survey
vious observations of cross-resistance between quinine and
to determine why many could still die of malaria in France in
2001, even though this is a remote territory of France. The
Despite the absence of use of sulfadoxine-pyrimethamine,
results showed an unexpectedly high prevalence of resistance
all but one of the strains tested were resistant to pyrimeth-
to many available antimalarial drugs.
amine (IC50 > 2,000 nM). This is most likely due to numerous
The study was conducted from May 2000 to February 2001
treatments with other antifolates for microbial infections
among the patients from the different health centers of the
(e.g., cotrimoxazole). In contrast with many chloroquine-
island and those admitted to Mamoudzou Hospital. It was
resistant areas where amodiaquine is a suitable alternative to
reviewed and approved by the health regional authority, and
chloroquine as a first-line treatment,6 the prevalence of resis-
samples were obtained from patients after informed consent
tance to this drug is 24%. Therefore, amodiaquine cannot be
was provided. All patients had a Plasmodium falciparum
recommended as an alternative to chloroquine for treatment
−positive histidine-rich protein 2 (Cape Biotech Malaria
of a disease that can be fatal within 24−48 hours.
Rapid Test; Abbott Diagnostic, Rungis, France) or parasite
Finally, as in many other areas where artemisinin deriva-
lactate dehydrogenase (LDH) test (Optimal; Diamed, Paris,
tives have not yet been used, a number of isolates showed
France) result, which was verified by microscopic examina-
IC50 values greater than the threshold of 10 nM and 20%
tion of thin and thick blood smears. A venous blood sample
showed values of 5−10 nM. Although resistance to artemisi-
was taken either at the hospital or in dispensaries and kept
nin derivatives remains debatable, it is known that even
at 4°C for a maximum of four hours before performing an
seven-day treatments have failure rates of 5−7%. This is con-
in vitro culture. Drug sensitivity assays were determined for
sistent with in vitro findings. No significant difference in sus-
chloroquine sulfate, quinine hydrochloride, amodiaquine hy-
ceptibility was found between patients from rural areas, who
drochloride, mefloquine hydrochloride, pyrimethamine, and
constituted the majority (82%) of the study population, and
artemisinin. The conditions for in vitro culture of isolates in
those from urban areas. In addition, resistance to pyrimeth-
96-well plates are the same as those previously described.1
amine was investigated in 40 additional parasite isolates with
Antimalarial drugs solutions were prepared for each assay.
a nested polymerase chain reaction and restriction fragment
Drug sensitivity was determined using the colorimetric
length polymorphism as reported by Eldin de Pecoulas and
FIGURE 1. Distribution of the 50% inhibitory concentrations (IC50s) of the antimalarial drugs studied with 132 isolates of Plasmodiumfalciparum from Myotte in the Comorian Islands. Results for pyrimethamine are not shown because all isolates were resistant and only one
showed borderline resistance. CQ ס chloroquine; QN ס quinine; AQ ס amodiaquine; MF ס mefloquine; AT ס artemisinin. The shaded areas
correspond to the threshold values between susceptibility and resistance. The values at the bottom of the figure are the geometric (Geo) mean
ICSO concentration for each drug and the 95% confidence interval (CI).
DRUG-RESISTANT P. FALCIPARUM MALARIA IN MAYOTTE
others.7 This showed a point mutation in codon 108 (Ser
but would moreover constitute an outstanding opportunity to
(AGC) to Asn (AAC)) in the dihydrofolate reductase gene in
investigate its ability to control transmission and potentially
62% of the isolates (other mutations were not investigated).
eradicate malaria in a small, well-delineated territory, i.e.,
Our results are puzzling and in marked contrast with those
without borders with other endemic countries.
obtained in neighboring areas such as Madagascar, where re-sults over the past 10 years have showed a moderate but
Received September 4, 2003. Accepted for publication December 18,
stable prevalence of resistance to chloroquine, together with
a low prevalence of resistance to other drugs.8 Less numerous
Authors’ addresses: Franc¸ois Pettinelli, Marie-Edith Pettinelli, Julie
data are available from the neighboring islands of Anjouan
Millet, and Delphine Michel, Centre Hospitalier de Mayotte, 97600
and other Comorian islands. The last survey conducted in
Mamoudzou, Mayotte. Philippe Eldin de Pe´coulas and Philippe Bras-
seur, Faculte´ de Me´decine, 22, Boulevard Gambetta, 76183 Rouen,
1992 showed a chloroquine resistance level of 22.2% in seven-
France. Pierre Druilhe, Unite´ de Parasitologie Bio-Me´dicale, Institut
day in vivo assays.9 This situation suggests that the improved
availability in Mayotte, compared with Africa, of antimalari-
Reprint requests: Pierre Druilhe, Unité de Parasitologie Bio-
als and other drugs through a free and well-organized health
Médicale, Institut Pasteur, 25 Rue du Dr Roux, 75015 Paris, France,
system, has contributed to the emergence of multidrug-
Telephone: 33-1-45-68-85-78, Fax: 33-1-45-68-86-40, E-mail: druilhe@
resistant P. falciparum malaria.
Given this state of affairs, it is somewhat puzzling that it
took so many years of treatment failures to initiate a prelimi-
nary evaluation of the actual status of susceptibility. Our re-
1. Brasseur P, Druilhe P, Kouamouo J, Brandicourt O, Danis M,
sults should have at least triggered further in vitro and in vivo
Moyou SR, 1986. High level of sensitivity to chloroquine of 72
Plasmodium falciparum isolates from southern Cameroon in
investigations, which are known to be complementary. It is
January 1985. Am J Trop Med Hyg 35: 711–716.
shocking that given the degree of health care in Mayotte new
2. Druilhe P, Moreno A, Blanc C, Brasseur PH, Jacquier P, 2001.
and more adequate regimens have not yet been implemented.
A colorimetric in vitro drug sensitivity assay for Plasmodium
Indeed, the current recommendation for treatment is a com-
falciparum based on a highly sensitive double-site lactate de-
bination of chloroquine with sulfadoxine-pyrimethamine,
hydrogenase antigen-capture enzyme-linked immunosorbent
assay. Am J Trop Med Hyg 64: 233–241.
which in view of our observations, would constitute the worst
3. Moreno A, Brasseur P, Cuzin-Ouattara N, Blanc C, Druilhe P,
possible option. In addition, this combination therapy has not
2001. Evaluation under field conditions of the colourimetric
been the object of rigorous in vivo investigations to determine
DELI-microtest for the assessment of Plasmodium falciparum
its efficacy. It has unfortunately remained mandatory despite
drug resistance. Trans R Soc Trop Med Hyg 95: 100–103.
4. Moreno A, Cuzin-Ouattara N, Nebie I, Sanon S, Brasseur P,
reports of treatment failures and communication of the
Druilhe P, 2001. Use of the DELI-microtest to determine the
present data in January 2001 to the health authorities in May-
drug sensitivity of Plasmodium falciparum in Burkina Faso.
otte, as well as to the Direction Generale de la Sante in Paris,
Ann Trop Med Parasitol 95: 309–312.
and repeated recommendations to use artemisinin-based
5. Brasseur P, Kouamouo J, Moyou RS, Druilhe P, 1990. Emer-
gence of mefloquine-resistant malaria in Africa without drug
pressure (letter). Lancet 336: 59.
In view of the data in this report, therapeutic options are
6. Brasseur P, Guiguemde R, Diallo S, Guiyedi V, Kombila A,
scarce and few alternatives are currently available, other than
Ringwald P, Olliaro P, 1999. Amodiaquine remains effective
drug combinations such as quinine-tetracycline or artesunate-
for treating uncomplicated malaria in West and Central Africa.
mefloquine. However, the former combination has shown
Trans R Soc Trop Med Hyg 93: 645–650.
7. Eldin de Pecoulas P, Basco LK, Abdallah B, Dje MK, Le BJ,
insufficient compliance during ambulatory treatment in dis-
Mazabraud A, 1995. Plasmodium falciparum: detection of an-
pensaries. In our opinion, this suggests that the three-day
tifolate resistance by mutation-specific restriction enzyme di-
artesunate-mefloquine combination promoted by investiga-
gestion. Exp Parasitol 80: 483–487.
8. Randrianarivelojosia M, Raharimalala LA, Randrianasolo L,
One could argue that eradication through vector control
Ratsimbasoa A, Rason MA, Ariey F, Jambou R, 2001. Mada-
gascar isolates of Plasmodium falciparum showing low sensi-
might be achievable in Mayotte, as on other small islands such
tivity to artemether in vitro. Ann Trop Med Parasitol 95: 237–
as la Réunion, Martinique, and Guadeloupe. However, sev-
eral years of vector control in Mayotte has failed to prevent
9. Feillet N, Agnamey P, Brasseur P, Druilhe P, 1993. In vivo re-
the present increase in endemicity and many breeding sites
sistance of Plasmodium falciparum to chloroquine in Anjouan
(Comoros). Bull Soc Pathol Exot 86: 48–51.
are hardly accessible in the relatively large, wild, forested
10. Looareesuwan S, Viravan C, Vanijanonta S, Wilairatana P,
areas of Mayotte. In this regard, it is worth mentioning that
Pitisuttithum P, Andrial M, 1996. Comparative clinical trial of
the increased use of artemisinin derivatives in Southeast Asia
artesunate followed by mefloquine in the treatment of acute
indicates that they also exert a gametocytocidal effect,11 in
uncomplicated falciparum malaria: two- and three-day regi-
contrast to sulfadoxine-pyrimethamine, which tend to in-
mens. Am J Trop Med Hyg 54: 210–213.
11. Price RN, Nosten F, Luxemburger C, ter Kuile FO, Paiphun L,
crease transmission. Therefore, in the case of Mayotte, arte-
Chongsuphajaisiddhi T, White NJ, 1996. Effects of artemisinin
misinin may not only be the most efficient therapeutic option,
derivatives on malaria transmissibility. Lancet 347: 1654–1658.
ROYAUME DU MAROC MINISTERE DE LA SANTE CENTRE HOSPITALIER IBN ROCHD Dossier d’Appel d’Offres Ouvert N° 037-2013 OBJET : ACHAT DES MEDICAMENTS AVERTISSEMENT Pour pouvoir communiquer les modifications éventuelles que le maître d’ouvrage se réserve le droit d’apporter au dossier du présent appel d’offres conformément à l’article 21 du règlement fixa
Whom may we thank for referring your child to our office I understand the above information and guarantee this form was completed correctly to the best of my knowledge and understand it is my responsibility to inform Fairfax Corner Orthondontics and Pediatric Dentistry of any changes to the information I have provided. I agree to be responsible for all charges for dental services and materials
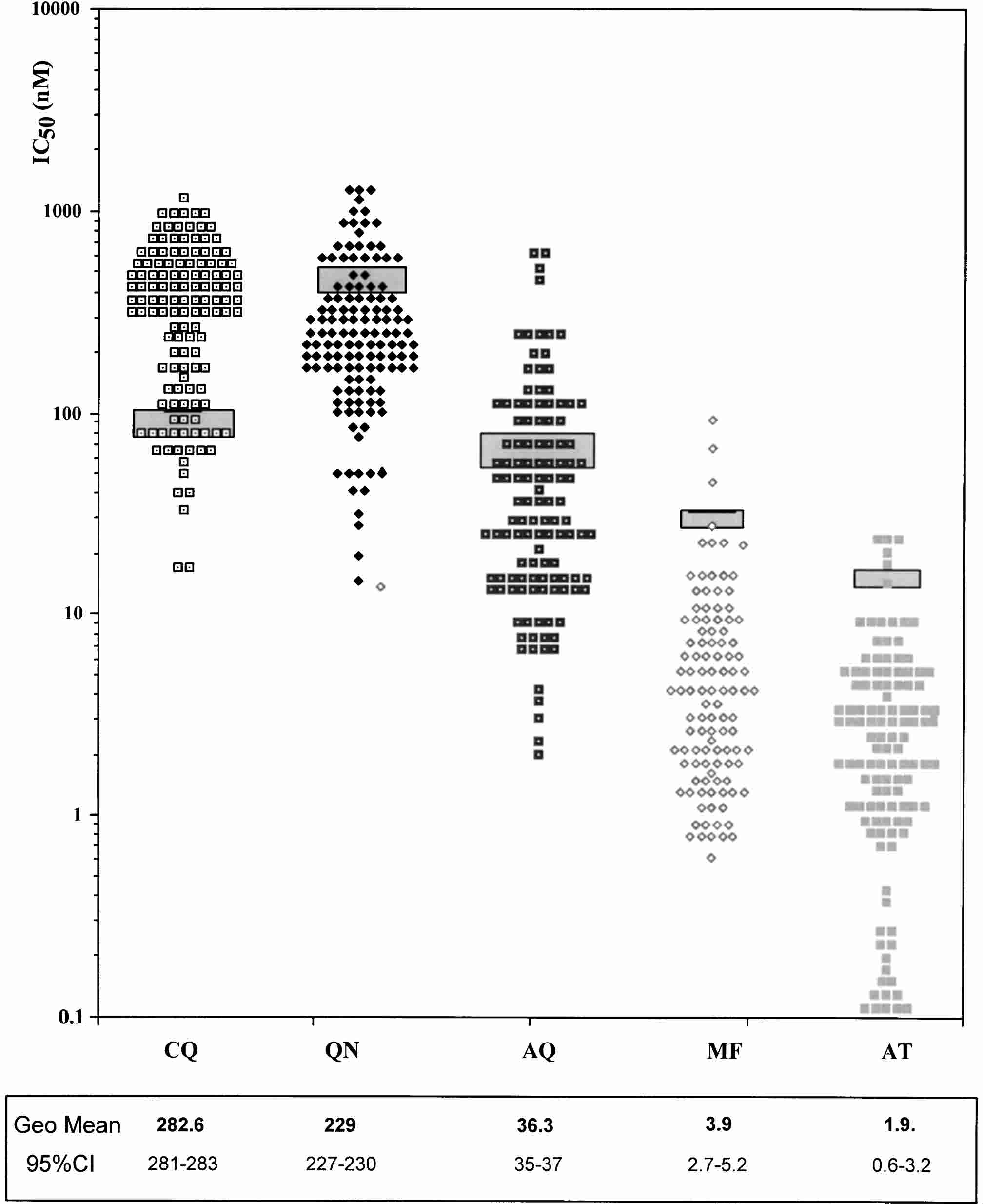 FIGURE 1. Distribution of the 50% inhibitory concentrations (IC50s) of the antimalarial drugs studied with 132 isolates of Plasmodium
falciparum from Myotte in the Comorian Islands. Results for pyrimethamine are not shown because all isolates were resistant and only one
showed borderline resistance. CQ ס chloroquine; QN ס quinine; AQ ס amodiaquine; MF ס mefloquine; AT ס artemisinin. The shaded areas
correspond to the threshold values between susceptibility and resistance. The values at the bottom of the figure are the geometric (Geo) mean
ICSO concentration for each drug and the 95% confidence interval (CI).
FIGURE 1. Distribution of the 50% inhibitory concentrations (IC50s) of the antimalarial drugs studied with 132 isolates of Plasmodium
falciparum from Myotte in the Comorian Islands. Results for pyrimethamine are not shown because all isolates were resistant and only one
showed borderline resistance. CQ ס chloroquine; QN ס quinine; AQ ס amodiaquine; MF ס mefloquine; AT ס artemisinin. The shaded areas
correspond to the threshold values between susceptibility and resistance. The values at the bottom of the figure are the geometric (Geo) mean
ICSO concentration for each drug and the 95% confidence interval (CI).