Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Quintessence journals
CASE REPOR t Publication Apexification and coronal restoration after traumatic tooth avulsion: a 10 year follow-up Dr Oliver Pontius, MSD Diplomate, American Board of Endodontics, Höhestr. 15, D-61348, Bad Homburg, Germany Key words adhesive restoration, apexification, avulsion, dental trauma, immature root, MTA
This case report looks at a case of traumatic avulsion and subsequent apexification of a maxillary permanent incisor of a 6-year-old boy and a 10-year follow-up is reported. Treatment included apex-ification of the tooth with incomplete root formation using mineral trioxide aggregate and restora-tion of the immature root with a zirconia post and a coronal composite restoration. At the 10-yearfollow-up the tooth was asymptomatic, functional and showed radiographically intact periapical tissues. Introduction
further trauma of the periapical tissues due to overex-tended root canal fillings and may also lead to three-
Dental injuries are very common in children and ado-
dimensionally underfilled root canals prone to leak-
lescents. According to Trope1 the maxillary central inci-
age2. An apexification treatment procedure is
sors are the most frequently avulsed teeth in both the
indicated in such cases. Long-term apexification with
permanent and primary dentition. When a tooth is
calcium hydroxide dressings has been performed with
avulsed, the attachment apparatus of the root (peri-
reasonable success3. The aim of this treatment mode
odontal ligament and the cemental layer) is damaged
is to induce the formation of a hard tissue barrier at the
and the blood vessels at the apex of the tooth are sev-
apex so that a root canal filling material can be prop-
ered, rendering the pulp necrotic2. Treatment is
erly introduced without the risk of over-extension4.
directed at minimising damage and inflammation of
The disadvantage of using calcium hydroxide for
the periodontal membrane. In the tooth with incom-
apexification is that it can take several months to
plete root development, the primary treatment goal
obtain a physiological hard tissue apical barrier. The
must be to promote revascularisation of the pulp
patient is required to present for treatment at multiple
tissue. In non-vital immature teeth with open apices,
times and, in addition, these teeth are susceptible to
a number of difficulties for adequate endodontic ther-
fracture during treatment2,4. It has been demonstrated
apy are present. The lack of an apical stop may lead to
that the long-term use of calcium hydroxide can
Apexification and coronal restoration Publication
had been performed. The patient saw his physician
The clinical examination 2.5 weeks after the trauma
(Fig 1) revealed that teeth 11 and 21 were partiallyerupted, slightly protruded and rotated. A sinus tractwas present about 4 mm below the buccal gingivalmargin of tooth 21 (Fig 2). Enamel craze lines in tooth11 were clearly visible using transillumination. All otherteeth were intact and free from caries. Periodontal tis-sues appeared healthy. The pocket depths of tooth 11
Fig 1 Intraoral view during clinical examination two and a half weeks after the trauma . A sinus tract was present
were 2 mm on the buccal, palatal, distal and mesial
about 4 mm below the buccal-gingival margin of tooth 21.
aspects. Sound periodontal probing was not performedfor tooth 21 as it had been replanted shortly. No mobil-
weaken dentine and make teeth even more suscepti-
ity of the adjacent teeth was present with exception of
ble to fracture5. Mineral trioxide aggregate or MTA
tooth 21, which showed grade 1 to 2 mobility.
(Pro Root, Dentsply, Konstanz, Germany) has proved
In the clinical tests tooth 21 was slightly tender to
to be a potential root-end filling material. In vitro and
palpation, percussion and biting pressure. Tooth 11
in vivo studies have demonstrated the good sealing
showed a delayed response to cold, heat, and electric
ability of this material, its excellent biocompatibility
pulp testing (Vitality tester, Analytic, Orange, CA, USA:
and low cytotoxicity, and also its effect on the induc-
threshold reading 67/80). Tooth 21 did not respond to
tion of odontoblast activity and on the formation of a
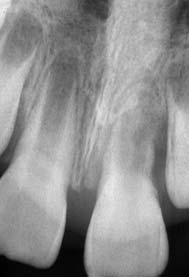
any of the sensibility tests used. Periapical radiographic
hard-tissue barrier6-10. Meanwhile, clinical studies have
examination (Fig 3) showed the immature open apices
confirmed the high regenerative potential of MTA,
of teeth 11 and 21, an intact periodontal ligament of
thus justifying its use for creating an apical barrier in
tooth 11, as well as evidence of an inflammatory root
resorption in the apical part of tooth 21.
The aim of this report is to describe the treatment
A diagnosis of pulp necrosis and asymptomatic
of an avulsed immature permanent incisor submitted
apical periodontitis was made for tooth 21. The fol-
to apexification with MTA, and the subsequent coro-
lowing treatment plan was presented to the parents:
apexification followed by non-surgical root canal ther-apy of tooth 21. As an alternative approach the extrac-tion of tooth 21 followed by orthodontic treatment
Case report
was discussed. The restorative treatment plan includeda bonded composite restoration and a custom-made
A 6-year-old boy with no general health problems was
mouthguard. The parents were informed about the
referred to the author’s endodontic office on July 6th
1999 for treatment of tooth 21. About 2.5 weeks pre-
On July 7th 1999 treatment was started. Local
viously, the boy had suffered an injury while rollerblad-
anaesthesia was administered (1.8 ml of 2% lidocaine
ing. He had hit the ground and avulsed his maxillary
HCL [36 mg] with 1:100,000 adrenaline [0.018 mg]).
left central incisor (June 19th 1999). His father had
Rubber dam was fixed with dental floss, isolating teeth
recovered the tooth from the ground, wrapped it in a
21 and 11. Using a surgical operating microscope an
napkin and the boy had immediately seen the family’s
access cavity was prepared. Ultrasonically activated irri-
clinician. Following a clinical examination, it was con-
gation was performed with 0.5% sodium hypochlorite.
firmed that there were no other injuries present and
Cleaning and shaping were performed using Gates
the socket and the tooth was rinsed with sterile saline,
Glidden drills #2 to #5 and K-type hand files. Root canal
and the tooth replanted. According to the patient’s
length was determined with an electrical apex locator
father, the extra-oral dry time was about 45 minutes.
(Root ZX, Morita, Tokyo, Japan) and the result was con-
No antibiotic coverage and no splinting of the tooth
firmed radiographically with a size 120 K-file (Fig 4).
Apexification and coronal restoration Publication Fig 2 Preoperative radiograph, sinus Fig 3 Preoperative radiograph, July 6th Fig 4 Working length radiograph, July
An aqueous calcium hydroxide suspension was packed
hydroxide dressing was carried out if necessary.
with Schilder hand pluggers (Dentsply) and the access
Ibuprofen (200 mg) was prescribed every 6 hours (if
cavity was sealed with glass-ionomer cement (Ketac
Molar, Espe, Seefeld, Germany). After removal of the
At the following visit (January 4th 2000) the tooth
rubber dam, the occlusion was checked and the patient
was asymptomatic and the sinus tract was closed.
was rescheduled for a 3 month radiographic check and
After local anaesthesia and isolation using rubber dam
replacement of the calcium hydroxide dressing if nec-
(as previously described) the access to the root canal
essary. Ibuprofen 200-mg was prescribed every 6 hours
was reopened under the microscope. The calcium
if post-operative pain meant an analgesic was required.
hydroxide dressing seemed washed out again and
At the second visit (September 10th 1999), the
ultrasonically activated irrigation with 0.5% sodium
patient reported that the sinus tract initially had
hypochlorite cleaning and shaping to working length
resolved, but had reappeared the previous week. After
using K-type hand files was repeated. There still was
local anaesthesia with 1.8 ml of 2% lidocaine HCL (36
no evidence of a hard-tissue barrier. The final irrigation
mg) with 1:100,000 adrenaline (0.018 mg), rubber
consisted of a 17% EDTA rinse followed by sodium
dam (clamp #9T, Hu Friedy, Leimen, Germany) was
hypochlorite. The root canal was dried with sterile
applied. Under the microscope the calcium hydroxide
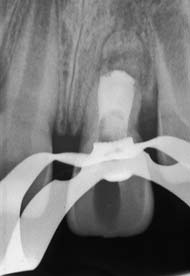
paper points. MTA was placed into the apical 5 mm of
intracanal dressing seemed to have been washed out.
the canal under control with the surgical microscope
Gentle irrigation with 0.5% sodium hypochlorite acti-
(Fig 6) using a MTA carrier (Dovgan Carrier, Quality
vated by ultrasonics was performed. Cleaning and
Aspirators, Duncanville, TX, USA) and condensed with
shaping to the working length was repeated, the fora-
Schilder hand pluggers and ultrasonics. A moistened
men was probed with a size 150 Kerr hand file. There
cotton pellet (2% chlorhexidine) was placed over the
was no evidence of an apical barrier. Calcium hydrox-
material. The access cavity was closed with glass-
ide was again packed with Schilder hand pluggers and
ionomer cement. A prescription for 200 mg of ibupro-
the access cavity sealed with glass-ionomer cement.
fen every 6 hours as needed for pain was given to the
The calcium hydroxide dressing was checked radi-
ographically (Fig 5). The patient was rescheduled for
On January 21st 2000, rubber dam was applied,
a 3 month check and replacement of the calcium
the temporary filling was removed, and the hardness
Apexification and coronal restoration Publication Fig 5 Contr
ol of the density and ex- o
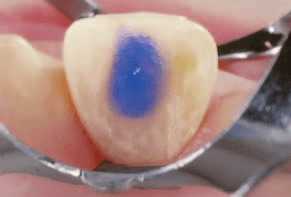
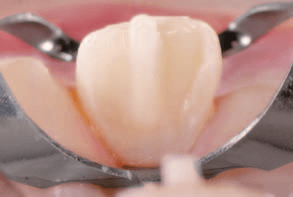
oxide, September 10 c Fig 6 Root canal filling with MTA (January 4th 2000) was placed into the apical 5 mm of the canal with Schilder pluggers under control with the surgi- cal microscope. Fig 7 Conditioning of the enamel with phosphoric acid, Fig 8 Adhesive fixation of the zirconia post with composite,
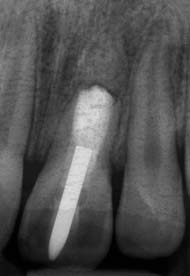
of the MTA was checked under the microscope with a
MI, USA), the occlusion was checked and a post-
sharp explorer. A zirconia post (Cerapost, ISO 110,
operative radiograph was taken (Fig 10).
Komet, Lemgo, Germany) was adhesively fixed into
Six months later (July 11th 2000), a recall check was
the wide root canal to strengthen the fragile root. The
done by the family clinician. The tooth was asympto-
largest available post was inserted in an upside-down
matic. The periapical radiograph showed an intact peri-
direction due to the very wide diameter of the canal.
odontal ligament with some type of osseous-like tissue
The enamel was etched by applying 34% phosphoric
forming apically to the MTA (Fig 11). Periodontal tissues
acid for 60 seconds (Fig 7), followed by irrigation with
appeared healthy, pocket depths were 2mm on the
sterile saline. A dentine-bonding agent (Clearfill,
buccal and distal, and 1mm on the palatal and mesial
Morita, Kuraray, Japan) was applied, and a size 3 zir-
aspects and no increased tooth mobility was present.
conia post (Fig 8) was adhesively fixed (Panavia TC,
On June 27th 2002, the patient was scheduled for a
Morita, Kuraray, Japan). The access cavity was sealed
further recall appointment with his clinician. The tooth
with a composite (Fig 9), (Herculite, Kerr, Romulus,
was still asymptomatic. Radiographically, some osseous
Apexification and coronal restoration Publication
2000. ence Fig 9 Access cavity sealed with composite, January 21st 2000. Fig 11 Recall radiograph, July 11th Fig 12 Recall radiograph, June 27th Fig 13 Recall radiograph, June 27th
structure had formed apically to the MTA, which had
The periodontal tissues showed local gingivitis around
taken a root-like shape, to the extent that a lamina dura
the labial aspect of tooth 21, pocket depths were 3mm
appeared to have formed (Figs 12 and 13). The peri-
on the mesial and distal, and 1mm on the palatal and
odontal tissues appeared healthy, pocket depths were
2mm on the buccal aspect, no mobility was present.
2mm on the mesial and distal, and 1mm on the palatal
A 10-year recall check was performed by the
and buccal aspects, and no increased mobility was
patient’s clinician on January 5th 2009. The tooth was
present. In the meantime, the patient underwent ortho-
asymptomatic. The periapical radiograph showed an
intact periodontal ligament surrounding the root-like
On April 24th 2006, the patient was scheduled for
structure apically to the MTA (Fig 15). Periodontal tis-
another recall appointment. The tooth was asympto-
sues appeared healthy, pocket depths were within
matic. Apically to the root-like structure exhibiting a
normal limits and no increased tooth mobility was
normal periodontal ligament, there was another radio-
present. The clinical crown of the tooth appeared
opaque area followed by a radiolucent zone (Fig 14). Apexification and coronal restoration Publication
Recall radiograph, April 24th o Fig 15 Recall radiograph, January 5th 2009. Fig 16 Intraoral view January 5th 2009. Discussion
Recent studies showed that soaking the tooth in
doxycycline17 or covering the root with minocycline18
Although the tooth was not replanted within the first
significantly enhanced revascularisation in dogs.
20 minutes after avulsion, the root exhibited almost no
The apical barrier technique using MTA seems
external resorption, even 10 years after the trauma.
very promising in traumatic tooth injuries with open
Perhaps even revascularisation as well as continued
apices11,12. As MTA has been found to be able to
root development would have been possible if the
ensure a tight closure of an apical foramen and to
most recent treatment protocols13-15 had been fol-
promote cementum coverage directly upon the MTA
lowed. Regenerative endodontics promotes a para-
surface, a double seal of the root canal can be
digm shift in treating endodontically involved imma-
achieved6-9. Short-term placement of calcium
ture permanent teeth. This ranges from performing
hydroxide in the root canal with the purpose of dis-
apexification procedures to conserving any dental
infecting the root canal and dentinal tubules, dissolv-
stem cells that might remain in the disinfected viable
ing pulp remnants and also drying up the apical zone
tissues so as to allow tissue regeneration and repair to
before obturation of the root canal with MTA,
achieve apexogenesis/maturogenesis16.
appears to be a good alternative to the long-term use
Apexification and coronal restoration Publication
Cvek M. Prognosis of luxated non-vital maxillary incisors n
of calcium hydroxide from a mechanical point of view
treated with calcium hydroxide and filled with gutta-per-
(fracture resistance)19. However, further prospective
cha. A retrospective clinical study. Endod Dent Traumatol
long-term outcome studies should be designed to
compare this procedure with the traditional calcium
Andreasen JO, Farik B, Munksgaard E.C. Long-term calci-um hydroxide as a root canal dressing may increase risk of
root fracture. Dent Traumatol 2002;18:134-137.
Reinforcement of the thin dentinal walls seems to
Torabinejad M, Pitt Ford TR, Abedi HR, Kariyawasam SP,Tang HM. Tissue reaction to implanted root-end filling ma-
be critical in these cases. According to Kerekes et al4,
terials in the tibia and mandible of guinea pigs. J Endod
approximately 30% of these teeth will fracture during
Torabinejad, M, Pitt Ford TR, McKendry DJ, Abedi HR,
or after endodontic treatment. Therefore, it is recom-
Miller DA, Kariyawasam SP. Histologic assessment of min-
mended that intracoronal adhesive restorations are
eral trioxide aggregate as a root-end filling in monkeys. JEndod 1997;23:225-228.
placed to strengthen these teeth internally20. The use
Nakata TT, Bae KS, Baumgartner JC. Perforation repair
of a bonded all-ceramic high-toughness post made of
comparing mineral trioxide aggregate and amalgam usingan anaerobic bacterial leakage model. J Endod 1998;
zirconia may have helped to increase the fracture resist-
ance of this fragile tooth and to improve the aesthetic
10. Roberts HW, Toth JM, Berzins DW, Charlton DG. Mineral
trioxide aggregate material use in endodontic treatment:
outcome when compared with non-precious alloy
a review of the literature. Dent Mater 2008;24:149-164.
posts (which may have lead to discoloration of the
11. Simon S, Rilliard F, Berdal A, Machtou P. The use of miner-
tooth)21. However, the future may be in the restoration
al trioxide aggregate in one-visit apexification treatment:aprospective study. Int Endod J 2007;40:186-197.
of these teeth with tooth-coloured bonded fibre posts
12. Holden DT, Schwartz SA, Kirkpatrick TC, Schindler WG.
exhibiting almost the same modulus of elasticity as
Clinical outcomes of artificial root-end barriers with MineralTrioxide Aggregate in teeth with immature apices. J Endod
dentine and being easier to remove in cases of
13. Trope M. Regenerative potential of dental pulp. J Endod
Considering the alternative treatment options dis-
14. Jung IJ, Lee SJ, Hargreaves KM. Biologically based treat-
cussed earlier, the patient and his parents highly appre-
ment of immature permanent teeth with pulpal necrosis: acase series. J Endod 2008;34:876-887.
ciated the advantages of the endodontic approach,
15. Shabahang S, Torabinejad M, Boyne PP, Abedi HR,
especially in the long-term, as this meant high patient
McMillan P. A comparative study of root-end induction us-ing osteogenic protein-1, calcium hydroxide, and mineral
comfort, an acceptable aesthetic outcome and rea-
trioxide aggregate in dogs. J Endod 1999;25:1-5.
16. Huang GT. A paradigm shift in endodontic management of
immature teeth: conservation of stem cells for regeneration. J Dent 2008;36:379-386.
17. Cvek M, Cleaton-Jones P, Austin J, Lownie J, Kling M, Fatti
Acknowledgements
P. Effect of topical application of doxycycline on pulp revas-cularization and periodontal healing in reimplanted monkeyincisors. Endod Dent Traumatol 1990:64:170-176.
The author would like to thank Prof Hülsmann for his
18. Ritter AL, Ritter AV, Murrah, V, Sigurdsson A, Trope M. Pulp
revascularization of replanted immature dog teeth after
valuable help during the preparation of this manuscript.
treatment with minocycline and doxycycline assessed bylaser Doppler flowmetry, radiography, and histology. DentTraumatol 2004;20:75-84.
19. Andreasen JO, Munksgaard EC, Bakland, LK. Comparison
References
of fracture resistance in root canals of immature sheep teethafter filling with calcium hydroxide or MTA. Dent Traumatol
Trope M. Clinical management of the avulsed tooth. Dent
20. Katebzadeh N, Dalton BC, Trope M. Strengthening imma-
Trope M, Chivian N, Sigurdsson A. The role of endodontics
ture teeth during and after apexification. J Endod
after dental traumatic injuries. In: Cohen S, Burns R (eds).
Pathways of the pulp ed 8., St. Louis: Mosby-Elsevier,
21. Strub JR, Pontius O, Koutayas S. Survival rate and fracture
strength of incisors restored with different post and core
Rafter M. Apexification: a review. Dent Traumatol 2005;
systems after exposure in the artificial mouth. J Oral Rehabil
Kerekes K, Heide K, Jacobsen I. Follow-up examination of
22. Ferrari M, Vichi A, Garcia-Godoy F. Retrospective study of
endodontic treatment in traumatized juvenile incisors. J
the clinical performance of fiber posts. Am J Dent 2000;13
CHATTANOOGA-HAMILTON COUNTY HEALTH DEPARTMENT Household medical waste, such as sharps, bandages, Bandages and Dressing Disposal and medications, can be harmful to human health It is also recommended that soiled bandages, and the environment when improperly managed. disposable sheets and medical gloves be disposed of Improper disposal of medical waste can cause injury- with special c
Used to show a point in space where someone or something is, or where an event is happening. At a party/club/funeral etc at an event while it is taking place Used to show a particular period of time during which something happens Used to show the person or thing that an action is directed or aimed at Used to show the thing that caused an action or feeling Ex) The children all laughed at
 CASE REPOR t
CASE REPOR t Apexification and coronal restoration
Apexification and coronal restoration
 Apexification and coronal restoration
Apexification and coronal restoration
 Apexification and coronal restoration
Apexification and coronal restoration



 Apexification and coronal restoration
Apexification and coronal restoration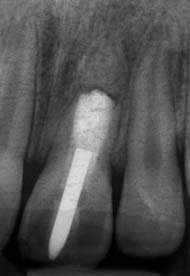

 Apexification and coronal restoration
Apexification and coronal restoration