Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Microsoft word - vc_japan2.doc
A Technology Review on Virtual Colonoscopy Virtual Colonoscopy: An Alternative Approach to Examination of the Entire Colon
Departments of Radiology, Computer Science and Biomedical Engineering
State University of New York, Stony Brook, NY 11794, USA
Abstract
We have developed a virtual colonoscopy system aiming toward mass screening for polyps through the entire colon. This work reviews the key technical components of the system. Introduction
Colorectal carcinoma is the second leading cause of cancer-related deaths among men and women in the United States, following lung cancer, with 56,000 deaths reported in 1998 and an estimated over 130,000 new cases per year [21]. Unfortunately the symptoms of colon cancer, such as anemia and change in bowel habits, are neither sensitive nor specific. Diagnosed cancers are often in the later stage of development, resulting in a high mortality incidence. Most colon cancer probably arises from polyps, which can take 5 to 15 years for malignant transformation. Recent studies have shown that screening of colonic polyps can reduce the mortality rate from the cancer. Optical colonoscopy and barium enema are the two most commonly used diagnostic procedures. Other tools include fecal occult blood testing (which detects only 30-40% of colorectal cancer and 10% of adenomas) and sigmoidoscopy (which fails to detect lesions in the proximal colon, where 40% of all cancers occurs, and misses 10-15% sigmoid colon carcinomas [5, 10, 15, 37]). While optical colonoscopy is accurate and can biopsy detected polyps, it is expensive ($1,800), invasive (requires scope insertion), uncomfortable (colon washing and sedation required), time consuming (hours), and carries a small risk of perforation and death (colonic perforation in one in 500 to 1000 cases and death in one in 2,000 to 5,000 cases [29]). It fails to demonstrate the entire colon in 10-15% of the cases and thus misses 10-20% of the lesions [10, 15]. Barium enema is less expensive ($400) and non-invasive, but it is less accurate (less than 78% sensitivity in detecting polyps of size from 5 to 20 mm diameter [28]), more time consuming, and requires a good deal of patient positioning and cooperation when X-ray radiographs of the colon are taken at various views. An accurate, cost-effective, non-invasive, comfortable procedure for mass screening of colonic polyps with a size less than 1 cm in diameter is extremely valuable, since the detection and removal of these small polyps will totally cure the patient. Since 1994, several pilot studies [16, 19, 23, 31, 34, 39] evaluating the feasibility of virtual colonoscopy as an alternative means for colon screening have motivated a great amount of research interests ranging from image formation, and segmentation, to visualization [1, 3, 10, 11, 13, 20, 22, 26, 27, 32, 33, 38]. This alternative means utilizes computer virtual-reality techniques to navigate inside the reconstructed three-dimensional (3D) colon model created from computed tomography (CT) or magnetic resonance (MR) images, looking for polyps. It starts with a bowel cleansing procedure, similar to that used in conventional optical colonoscopy, and is followed by inflating the colon with room air or CO2 gas --- if CT modality is utilized --- introduced through a rectal insert.
This articles was translated into Japanese and published in INNERVISION, vol.16, no.10, pp. 40-44, 2001.
A Technology Review on Virtual Colonoscopy
Abdominal images are then taken in seconds (by breath holding) with sub mm resolution in both axial and transverse directions and with excellent image contrast between the colon wall and the lumen filled with air. Image segmentation is necessary for construction of a clean colon model. A successful image segmentation depends on the bowel preparation. Computer graphics is used to navigate through the 3D colon model. A user-friendly interactive navigation is desired to inspect local suspected areas. Due to the object length, a computer aided detection (CAD) means may speed up the screening of polyps through the entire colon. For the purpose of mass screening, the bowel preparation must be easy and tolerant. The construction of the colon model shall be fully automated. The navigation through the colon model must be fast and cover the entire colon inner surface. This work reviews the key technologies necessary for virtual colonoscopy to become a mass screening modality. Description of Key Technologies
Key technologies are described below in a task specific order for performing a virtual colonoscopy: (1) Bowel Preparation Protocol Bowel preparation has been a major obstacle for both virtual and optical colonoscopy becoming a mass screening modality. The conventional bowel preparation requires ingesting a large quantity of liquid in the evening to physically wash the colon before the colonoscopy [2]. For virtual colonoscopy, we have created an alternative to the conventional bowel washing procedure by utilizing image segmentation techniques on the CT images for electronic colon cleansing [7, 22]. Our bowel preparation includes a high fluid, low residual diet for two days with contrast solution of 250 cc barium sulfate suspension (2.1% w/v, E-Z-EM, Inc.) mixed with the diet. A 120 ml of MD- Gastroview (diatriuzoate meglumine and diatriozoate sodium solutions) in equal 60 ml amounts is ingested during the evening and in the morning before the CT scan. Magnesium citrate and bisacodyl tablets are given to liquefy the stool and a suppository is taken to empty the rectum and sigmoid colon. The goal of the contrast solutions is to enhance the image intensity of the stool and liquid to enable electronic removal by image segmentation techniques [22]. This electronic colon cleansing has been evaluated using healthy volunteers with multiple CT scans [7]. Our protocol is extended by the addition of a magnesium citrate laxative, bisacodyl tablets and a suppository for physical colon washing in the evening before CT scan in order to compare the results with optical colonoscopy by patient studies. The enhanced residual stool and fluid are then the targets of our image segmentation techniques [7, 22]. Optical colonoscopy is performed following the virtual procedure. (2) Image Acquisition Protocol It is well known that a conventional (non-spiral) CT samples the transverse field-of-view (FOV) by both detector element size and angular increment. The transverse image resolution can be less than 0.5 mm by currently available imaging protocols. However, the sampling along the rotation axis is limited by the collimation gap or axial detector element size, resulting in an axial image resolution larger than clinically desired. Pushing for a narrower collimation gap will require a longer
This articles was translated into Japanese and published in INNERVISION, vol.16, no.10, pp. 40-44, 2001.
A Technology Review on Virtual Colonoscopy
acquisition time, resulting in motion artifacts and more radiation to the patient. Spiral CT improves the axial sampling without sacrificing the acquisition speed [3, 11, 37]. During a completely angular sampling with M projections evenly spaced on 180o degrees, an axial distance equivalent to the collimation gap may be assumed to be sampled M times at the corresponding M projecting angles, respectively, if a 1.0:1.0 pitch is used. These M projections with partial axial sampling can be reconstructed to achieve an axial resolution of less than the collimation gap. Currently available spiral CT scanners use linear interpolation among the M projections to reconstruct the images with the slice thickness less than the collimation gap or similar to the transverse pixel size. It is clearly seen that the axial resolution characteristics are different from the transverse resolution. Ideally we desire an isotropic resolution in the three dimensions. There are two parameters affecting the results: the collimation gap and the pitch value. In order to cover the entire colon in a single breath hold, a larger gap or a higher pitch is needed. On the other hand, a smaller gap or a lower pitch is needed for a higher axial resolution. For a single detector ring CT scanner, we have been using a protocol of 5 mm collimation and pitches of 1.5 to 2.0 (depending on the body size) for over 100 patients and volunteers. The protocol of 7 mm collimation with a pitch range of 1.0 to 1.5 could generate results with lower axial resolution, even though both require the same data acquisition time. The later takes a larger collimation gap and smaller pitch value. Our phantom experiments demonstrated the former is a better choice. By currently available multiple detector rings CT scanners, we can achieve an isotropic 1 mm resolution in three dimensions in a single breath-hold time period. For the purpose of mass screening, the radiation associated with CT scans must be minimized [17]. This is determined by the electric current through the X-ray tube. We had tested the current values from 280 mA to 100 mA. With 100 mA, there was no miss detection of polyps greater than 3 mm size, as compared with 280 mA. With our developed noise treatment technology [24], we expect to minimize the radiation, while maintaining the high image quality. (3) Image Segmentation Method Image segmentation aims to group the image elements, or voxels, of the same tissue in a 3D space. The unique feature in the image segmentation is the use of the similarity of same tissue types. This is well characterized by the Markov random field (MRF) theory [22]. However, the implementation of any MRF model requires a very intense computing effort. Our segmentation technique considers this unique feature in a different way [7]. We construct a local intensity vector for each voxel to consider the similarity. Due to the statistical repeatability property of CT scans, given the protocol of 120 kVp and a constant mA, the local intensity vectors can be mapped onto the principal component axes by the Karhunen-Loeve (K-L) transformation. In the K-L space, only the first few components carry significant information and are used to construct a feature vector for each voxel. The similarities of the feature vectors are analyzed to classify image voxels. The algorithm is a modified self-adaptive on-line quantization method [12]. Unlike most MRF methods, it is computationally efficient without the iterative time-consuming process [22]. Given the classification, we extract the labeled voxels, with consideration given to the body anatomy, using region-growing methods. Lungs and bone are identified and excluded from further processing due to their distance from the colon. Next, the enhanced stool and fluid voxels within the colon are removed together with the CO2 voxels, considering the neighboring labels. The voxel
This articles was translated into Japanese and published in INNERVISION, vol.16, no.10, pp. 40-44, 2001.
A Technology Review on Virtual Colonoscopy
located within the rectal insert at the bottom of the volumetric image is selected as the seed point to extract the colon lumen. If colon collapse happens, the lumen consists of segments. The voxel classification by the segmentation algorithm and the extraction of labeled colon-lumen voxels by region-growing method are automatically accomplished on a currently available personal computer (PC) platform in less than ten minutes. The image segmentation strategy, combined with the colonic material tagging, is termed “electronic colon cleansing” and detailed in [7, 22]. (4) Fly Path and Navigation Environment Planning Given the extracted colon lumen or segments, we desire an environment that describes the colon shape and guides the navigation without colliding on or penetrating through the colon wall. The environment consists of two components: a centerline of the colon lumen and a penalized potential field within the lumen. The centerline is conceived as a medial or symmetric axis of a single object, or the colon lumen in our case. If the colon lumen is made of several segments due to collapse, the centerline is the connected axes of these segments. This single line is also frequently named the “skeleton” of the colon lumen, which is an abstract description of the colon lumen shape. A concise definition of the skeleton is given by the center locus of the maximal disks (in two dimensions) or balls (in three dimensions) within the shape. A direct implementation of the definition is the thinning of the object layer-by-layer until only a single layer, or points as described in [25], remains. This implementation is very time consuming. Various modifications have been attempted to improve the speed [4, 8, 13, 14, 19, 30, 36, 44]. An equivalent definition of the centerline is given in [42], based on the penalized potential field, which consists of the distances between each voxel inside the colon lumen and the starting point within the rectal insert (i.e., the distance from the start, DFS-distance field) and the distances between each voxel inside the lumen and the corresponding point on the lumen boundary (i.e., the distance from the boundary, DFB-distance field) [6, 35]. The implementation of this alternative definition demonstrated its computational efficiency and statistical robustness [42]. The extracted centerline is a smooth single path and stays as close as possible to the center of the colon. The extraction is fully automatic. It provides a flight path to guide the navigation through the entire colon lumen. The penalized distance field provides an environment to assist the navigation. The DFS-distance field encourages movement from the start point toward the end point. The DFB-distance field prevents collision on the colon wall by increasing the cost for voxels that are closer to the wall. By placing a virtual camera on our submarine navigation model, the environment smoothly guides the camera from the starting point to the end point. When interactive modes are activated to move the camera closer to the colon inner surface for inspection of any abnormality, the DFB-distance field will provide a gent force to prevent the virtual camera from colliding with the wall. Our planned navigation ensures users follow the flight path for an overview of the entire inner surface [18]. The embedded interactive modes allow users to deviate from the path toward the surface for detailed inspection, quantitative measurement and virtual biopsy [41]. When returning to
This articles was translated into Japanese and published in INNERVISION, vol.16, no.10, pp. 40-44, 2001.
A Technology Review on Virtual Colonoscopy
automatic navigation, the virtual camera is gently pushed away from the colon wall back to the center flight path. The fly path and penalized potential field provide an excellent environment for our planned navigation with interactive modes to examine the entire colon. When the suspected areas on the colon inner surface are “colored” by CAD means, then we navigate from one area to the other in a fast speed and stop by each suspected area at a normal view centered on the area. This combination ensures both the view of the entire colon surface and the inspection of the details at suspected locations in an efficient manner. By our on-going development on texture analysis [43], we expect to show the polyp growth tendency, in addition to the structural details at the suspected area. (5) Volume Rendering Based Fly Through of the Colon Model
Navigation through the entire colon lumen can be achieved by either surface- or volume-based rendering computer graphics techniques. The surface-based navigation is efficient (i.e., in real time), but lacks rendering quality in terms of the surface smoothness, and most importantly, it lacks information beyond the surface. It utilizes only the constructed colon model and renders the lumen surface for geometric information. Volumetric rendering uses both the constructed colon model and the raw image data set. For each endoscopic view --- from the virtual camera to the colon inner wall --- the image density information beyond the surface is added over the raw image data set by a transfer function or weighting process. The added information is at the cost of computing effort. For a 3D volumetric rendered endoscopic view, the standard perspective projection is widely employed [34]. Various improvements have been made to achieve real time rendering of the endoscopic views during navigation. Our virtual colonoscopy navigation speed relies on years of volume rendering research [40] at the State University of New York at Stony Brook and has achieved a speed of 15 frames per second on a currently available PC platform [9]. At this rate the interactive response following mouse activations seems natural and smooth. These key technologies have been implemented in both SGI- and PC-based computer workstations [9, 40]. Integrating the technologies with a sophisticated user graphics interface (UGI) on a PC platform is presented below. Brief Presentation of Viatronix Visualization System
The key technologies were patented by the Research Foundation of the State University of New York and licensed to Viatronix Incorporated for commercial production. These key technologies were integrated into a virtual colonoscopy system, called the Viatronix Visualization System (VVS) or V3D system. It consists of two parts: one is a V3D PC processor and the other is a V3D PC viewer. The V3D processor takes the DICOM (digital image communication in medicine) formatted 2D images through Internet interface to the image acquisition device (or a CT scanner). Then it segments the images and builds up the 3D colon model and the fly-path environment. The V3D viewer takes the input of users from the keyboard and/or mouse and provides volume-based rendering of prospective projections or endoscopic views during navigation. A picture of the UGI panel of the V3D viewer is shown below.
This articles was translated into Japanese and published in INNERVISION, vol.16, no.10, pp. 40-44, 2001.
A Technology Review on Virtual Colonoscopy
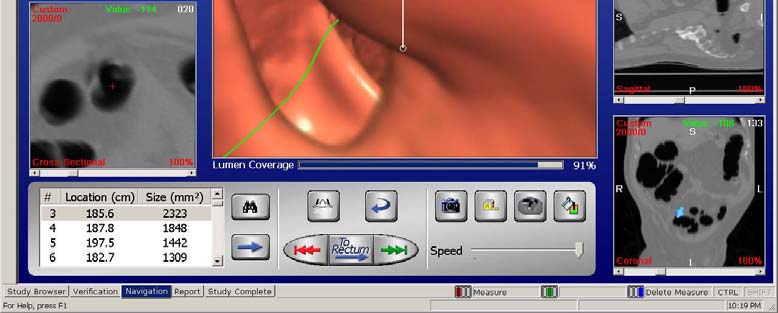
Figure 1: The computer display panel of V3D System.
Image segmentation and flight path and navigation environment planning are performed automatically by the V3D processor. (It also acts as a DICOM/PACS (picture archiving and communications system) server for image archiving and retrieval). The user only interacts with the navigation or examination portion of the V3D viewer. The user has the opportunity to verify that the automated process had worked correctly. If any correction is needed, the V3D viewer provides various interactive tools to assist the user in editing the constructed colon model. The top left of the display panel in Figure 1 shows a colon model. To facilitate the user during navigation, the V3D viewer provides multiple views of the raw patient data set. Shown down the right hand side of the display panel are 2D slice views of the transverse, sagittal and coronal images. An oblique reformatted slice perpendicular to the colon centerline is shown on the bottom left corner. The colon model on the top left shows an outside “map” view with an indication of the current virtual camera position and orientation. In the center is the 3D volumetric rendered endoscopic view using the standard perspective projection and our specifically developed, fast volume rendering strategies. All of these 2D and 3D images are correlated together so the position in the 3D volume image is overlaid on the 2D slice images, and positions of 2D slices are overlaid on the 3D volume. This provides a fast, simple means to easily analyze suspicious areas in both 2D and 3D spaces. The navigation speed (for both view rendering and display response to mouse activation) is in real time. The interactive tools include, for example, the measurements of polyp size and its location
This articles was translated into Japanese and published in INNERVISION, vol.16, no.10, pp. 40-44, 2001.
A Technology Review on Virtual Colonoscopy
from the rectum, slice cutting of polyp for internal image density display, and 3D semi-translucent view or “virtual biopsy.” Another important feature of the V3D viewer is its capability to display the covered area in real time after navigating from rectum to cecum and then back to the starting point. The V3D system was tested by phantom experiments for measurement accuracy on various data acquisition protocols (such as mA parameters, collimation gaps and pitch values). Our electronic cleansing techniques were validated using healthy volunteer scans, and polyp detection was corroborated through patient studies. The performance, as assessed by several radiologists, was very satisfactory. Discussion and Conclusion
It is a challenging task to develop virtual colonoscopy as a mass screening modality. The bowel preparation must be acceptable for the general population. The image segmentation and feature extraction for electronic colon cleansing must be accurate, robust, and efficient, with the capability to correct for colon segment collapses. The flight path and navigation environment planning must be robust and smooth enough to ensure a complete coverage of the entire colon surface. The volume rendering speed must be real time with 3D information for virtual biopsy and other quantitative texture analysis. The V3D system relies on key technologies that require a less strenuous bowel preparation, use a fully automated electronic colon cleansing technique with the ability to minimize the collapse effect, and provide a real time volume rendered navigation with user-friendly interactions for quantitative measurements of polyp size and location, especially with the capability for virtual biopsy and texture analysis using the 3D information. The phantom experiments suggested a narrower collimation gap and higher pitch for improved detection of smaller polyps. With protocols of 5 mm collimation and a pitch range of 1.5 to 2.0, it is possible to detect polyps as small as 3 mm in size. The possibility increases dramatically for larger polyps. Electronic colon cleansing was evaluated by healthy volunteer studies and showed the feasibility of using a much reduced colon preparation procedure. This may lead to the removal of patient preparation as the major obstacle to virtual colonoscopy becoming an accepted mass screening modality. The system currently takes less than 15 minutes to process the image data set used to build the colon model on a currently available PC platform or the V3D processor. The navigation for complete coverage of the entire colon surface also takes less than 15 minutes on a PC platform or the V3D viewer. The polyp detectability shown by the V3D system using a limited number (approximately 150) of patients is very encouraging. Compared to the findings of optical colonoscopy with a polyp size of greater than 5 mm, the V3D system identified all the polyps, and furthermore, detected more polyps located behind colon folds where optical colonoscopy is blind. The V3D system found some 3 mm
This articles was translated into Japanese and published in INNERVISION, vol.16, no.10, pp. 40-44, 2001.
A Technology Review on Virtual Colonoscopy
polyps that were not seen by the initial optical colonoscopy, and were verified by repeated optical colonoscopy. A larger scale clinical trial is needed and is in progress. Acknowledgment:
This work was supported by NIH Grant CA82402 of the National Cancer Institute, NSF Grant MIP9527694, and Viatronix Inc. References:
1 D. Ahlquist, A. Hara, and C. Johnson, “Computed tomographic colography and virtual colonoscopy,”
Gastro Endoscopy Clin North Am, vol. 7, pp. 439-452, 1997.
2 C. Bartram, “Bowel preparation – principles and practice,” Clin Radiology, vol. 49, pp. 365-367, 1994. 3 C. Beaulieu, S. Napel, B. Daniel, et al, “Detection of colonic polyps in a phantom model: implications for
virtual colonoscopy data acquisition,” J Computer Assisted Tomography, vol. 22, pp. 656-663, 1998.
4 I. Bitter, M. Sato, M. Bender, K. McDonnel, A. Kaufman, and M. Wan, “CEASAR: a smooth, accurate
and robust centerline extraction algorithm,” Proc IEEE Visualization’2000, pp. 45-52, 2000.
5 J. Bond, “Virtual colonoscopy – promising, but not ready for widespread use,” New England Journal of
Medicine, vol. 341, pp. 1540-1542, 1999.
6 G. Borgefors, “Distance transformations on digital images,” Computer Vision Graphics Image
7 D. Chen, Z. Liang, M. Wax, L. Li, B. Li, and A. Kaufman, “A novel approach to extract colon lumen
from CT images for virtual colonoscopy,” IEEE Trans on Medical Imaging, vol. 19, pp. 1220-1226, 2000.
8 R. Chiou, A. Kaufman, Z. Liang, L. Hong, and M. Achniotou, "Interactive fly-path planning using
potential fields and cell decomposition for virtual endoscopy," IEEE Trans on Nuclear Science, vol. 46, pp. 1045-1049, 1999.
9 F. Dachille, K. Kreeger, M. Wax, A. Kaufman, and Z. Liang, “Interactive navigation for PC-based virtual
colonoscopy,” Proc SPIE Medical Imaging, vol. 4321, to appear, 2001
10 H. Felon, D. Nunes, P. Schroy, M. Barish, P. Clarke, and J. Ferrucci, “A comparison of virtual and
conventional colonoscopy for the detection of colorectal polyps,” New England J Medicine, vol. 341, pp. 1496-1503, 1999.
11 J. Fletcher, C. Johnson, R. MacCarty, T. Welch, J. Reed, and A. Hara, “CT colonoscopy: potential pitfalls
and problem-solving techniques,” American Journal of Roentgenology, vol. 172, pp. 1271-1278, 1999.
12 Gersho and R. M. Gray, Vector Quantization and Signal Compression, Boston: Kluwer, 1992. 13 Y. Ge, D. Stelts, and D. Vining, “3D skeleton for virtual colonoscopy,” Lecture Notes in Computer
14 Y. Ge, D. Stelts, J. Wang, and D. Vining, “Computing the centerline of a colon: a robust and efficient
method based on 3D skeleton,” J Computer Assisted Tomography, vol. 23, pp. 786-794, 1999.
15 S. Grandqvist, “Distribution of polyps of the large bowel in relation to age: a colonoscopic study,” Scand
J Gastroenterology, vol. 16, pp. 1025-1031, 1981.
16 A. Hara, C. Johnson, J. Reed, D. Ahlquist, H. Nelson, R. Ehman, C. McCollough, and D. Ilstrup,
"Detection of colorectal polyps by CT colography: feasibility of a novel technique," Gastroenterology, vol. 110, pp. 284-290, 1996.
17 A. Hara, C. Johnson, J. Reed, D. Ahlquist, H. Nelson, R. Ehman, and W. Hermsen, “Reducing data size
and radiation dose for CT colonography,” Am J Roentgenology, vol. 168, pp. 1181-1184, 1997.
18 T. He, L. Hong, D. Chen, and Z. Liang, “Reliable path for virtual endoscopy: ensuring complete
examination of human organs,” IEEE Trans on Visualization and Computer Graphics, to appear, 2001.
19 L. Hong, A. Kaufman, Yi-Chih Wei, A. Viswambharan, M. Wax, and Z. Liang, "3D virtual
colonoscopy," In 1995 Proceedings of Biomedical Visualization, eds. by M. Loew and N. Gershon, Atlanta, Georgia, pp. 26-33, 1995.
This articles was translated into Japanese and published in INNERVISION, vol.16, no.10, pp. 40-44, 2001.
A Technology Review on Virtual Colonoscopy
20 L. Hong, Z. Liang, A. Viswambharan, A. Kaufman, and M. Wax, "Reconstruction and visualization of 3D
models of colonic surface," IEEE Trans on Nuclear Science, vol. 44, pp. 1297-1302, 1997.
21 H. Landis, T. Murray, S. Bolden, and P. Wingo, “Cancer Statistics, 1998. CA,” Cancer J Clin, vol. 48, pp.
22 Z. Liang, F. Yang, M. Wax, J. Li, J. You, A. Kaufman, L. Hong, H. Li, and A. Viswambharan, "Inclusion
of a priori information in segmentation of colon lumen for 3D virtual colonoscapy," Conf Record IEEE NSS-MIC, Albuquerque, New Mexico, Nov. 1997.
23 W. Lorensen, F. Jolesz, and R. Kikinis, “The exploration of cross-sectional data with a virtual
endoscope,” in Interactive Technology and the New Medical Paradigm for Health Care (ed. by R. Satava and K. Morgan), pp. 221-230, 1995.
24 H. Lu, I. Hsiao, X. Li, J. Hsieh, and Z. Liang, “Analysis of noise property in low-dose CT projections and
noise treatment by scale transformations,” Conf Record IEEE NSS-MIC, to appear, 2001.
25 C. Ma and M. Sonka, “A fully parallel 3D thinning algorithm and its applications,” Computer Vision and
Image Understanding, vol. 64, pp. 420-433, 1996.
26 E. McFarland, J. Brink, J. Loh, G. Wang, V. Argiro, D. Balfe, J. Heiken, and M. Vannier, "Visualization
of colorectal polyps with spiral CT colography: evaluation of processing parameters with perspective volume rendering," Radiology, vol. 205, pp. 701-707, 1997.
27 E. McFarland and J. Brink, “Helical CT colonoscopy (virtual colonoscopy): the challenge that exists
between advancing technology and generalizability,” Am J Roentgenology, vol. 173, pp. 549-559, 1999.
28 C. Morosi, G. Ballardini, and P. Pisani, “Diagnostic accuracy of the double-contrast enema for colonic
polyps in patients with or without diverticular disease”, Gastrointest Radiol, vol. 16, pp. 345-347, 1991.
29 P. Orsoni, S. Berdah, C. Verrier, A. Caamano, B. Sastre, R. Boutboul, J. Grimaud, and R. Picaud,
“Colonic perforation due to colonoscopy: a retrospective study of 48 cases”, Endoscopy, vol. 29, pp. 160-164, 1997.
30 D. Paik, C. Beaulieu, R. Jeffery, G. Rubin, and S. Napel, “Automatic flight path planning for virtual
endoscopy,” Medical Physics, vol. 25, pp. 629-637, 1998.
31 T. Parkins , "Computer lets doctors fly through the virtual colon," Journal of National Cancer Institute,
32 J. Reed and C. Johnson, “Automatic segmentation, tissue characterization, and rapid diagnosis
enhancements to the computed colographic colonoscopy analysis workstation,” J Digital Imaging, vol. 10, pp. 70-73, 1997.
33 A. Royster, A. Gupta, H. Fenlon, and J. Ferrucci, “Virtual colonoscopy: current status and feature
implications,” Acad Radiology, vol. 5, pp. 282-288, 1998.
34 G. Rubin, C. Beaulieu, V. Argiro, H. Ringl, A. Norbash, J. Feller, M. Dake, R. Jeffrey, and S. Napel,
"Perspective volume rendering of CT and MR images: applications for endoscopic imaging," Radiology, vol. 199, pp. 321-330, 1996.
35 T. Saito and J. Toriwaki, “New algorithm for Euclidean distance transformation of an N-dimensional
digitized picture with applications,” Pattern Recognition, vol. 27, pp. 1551-1565, 1994.
36 Y. Samara, M. Fiebrich, A. Dachman, J. Kuniyoshi, K. Doi, and K. Hoffmann, “Automatic calculation of
the centerline of the human colon on CT images,” Acad Radiology, vol. 6, pp. 352-359, 1999.
37 B. Simons, A. Morrison, R. Lev, and W. Verhoek-Oftendahl, "Relationship of polyps to cancer of the
large intestine," J National Cancer Institute, vol. 84, pp. 962-966, 1992.
38 P. Springer, A. Dessl, S. Giacomuzzi, A. Stohr, G. Bodner, and W. Buchberger, “Virtual CT
colonoscopy: examination techniques, limitations and perspectives,” Aktuelle Radiology, vol. 7, pp. 301-304, 1997.
39 D. J. Vining, D. Gelfand, R. Bechtold, E. Scharling, E. F. Grishaw, and R. Shifirin," Technical feasibility
of colon imaging with helical CT and virtual reality," 1994 Annual Meeting of Am Roentgen Ray Soc, New Orleans, pp. 104, 1994.
40 M. Wan, W. Li, K. Kreeger, I. Bitter, A. Kaufman, Z. Liang, D. Chen, and M. Wax, “3-D virtual
colonoscopy with real-time volume rendering,” Proc SPIE Medical Imaging, vol. 3978, pp. 165-171, 2000.
This articles was translated into Japanese and published in INNERVISION, vol.16, no.10, pp. 40-44, 2001.
A Technology Review on Virtual Colonoscopy
41 M. Wan, F. Dachille, K. Kreeger, S. Lakare, M. Sato, A. Kaufman, M. Wax, and Z. Liang, “Interactive
electronic biopsy for 3D virtual colonoscopy,” Proc SPIE Medical Imaging, vol. 4321, to appear, 2001.
42 M. Wan, Z. Liang, Q. Ke, L. Hong, I. Bitter, and A. Kaufman, “Automatic centerline extraction for
virtual colonoscopy,” Submitted to IEEE Trans on Medical Imaging, 2001.
43 Z. Wang and Z. Liang, “Feature based rendering for 2D/3D partial volume segmentation datasets,”
submitted to Proc SPIE Medical Imaging, 2002.
44 Y. Zhou and A. W. Toga, “Efficient skeletonization of volumetric objects,” IEEE Trans on Visualization
and Computer Graphics, vol. 5, pp. 196-209, 1999.
This articles was translated into Japanese and published in INNERVISION, vol.16, no.10, pp. 40-44, 2001.
Bijlage 4. Nederlandse lijst van mutagene stoffen (1 juli 2013) Lijst met mutagene stoffen als bedoeld in artikel 4.11 van het Arbeidsomstandighedenbesluit Ter verduidelijking van de vraag om welke stoffen en processen het hier in ieder geval gaat, houdt het Ministerie van Sociale Zaken en Werkgelegenheid een lijst2 bij van mutagene stoffen die moeten worden geclassificeerd als cate
Firma: 2 de Febrero, 1971 Normativa Dominicana: Resolución No. 316. Fecha 18 de Marzo, 1976 Gaceta Oficial: No. 9395. Fecha 3 de Marzo, 1976, Pág. 276 Colección de Leyes: Año 1976, Pág. 276 Suscrita en el Tercer Período Extraordinario de Sesiones de la AsambleaGeneral, celebrada en Washington, DC, el 2 de febrero de 1971LOS ESTADOS MIEMBROS DE LA ORGANIZACIÓN DE ESTADO

 A Technology Review on Virtual Colonoscopy
Figure 1: The computer display panel of V3D System.
Image segmentation and flight path and navigation environment planning are performed automatically by the V3D processor. (It also acts as a DICOM/PACS (picture archiving and communications system) server for image archiving and retrieval). The user only interacts with the navigation or examination portion of the V3D viewer. The user has the opportunity to verify that the automated process had worked correctly. If any correction is needed, the V3D viewer provides various interactive tools to assist the user in editing the constructed colon model. The top left of the display panel in Figure 1 shows a colon model. To facilitate the user during navigation, the V3D viewer provides multiple views of the raw patient data set. Shown down the right hand side of the display panel are 2D slice views of the transverse, sagittal and coronal images. An oblique reformatted slice perpendicular to the colon centerline is shown on the bottom left corner. The colon model on the top left shows an outside “map” view with an indication of the current virtual camera position and orientation. In the center is the 3D volumetric rendered endoscopic view using the standard perspective projection and our specifically developed, fast volume rendering strategies. All of these 2D and 3D images are correlated together so the position in the 3D volume image is overlaid on the 2D slice images, and positions of 2D slices are overlaid on the 3D volume. This provides a fast, simple means to easily analyze suspicious areas in both 2D and 3D spaces. The navigation speed (for both view rendering and display response to mouse activation) is in real time. The interactive tools include, for example, the measurements of polyp size and its location
This articles was translated into Japanese and published in INNERVISION, vol.16, no.10, pp. 40-44, 2001.
A Technology Review on Virtual Colonoscopy
from the rectum, slice cutting of polyp for internal image density display, and 3D semi-translucent
A Technology Review on Virtual Colonoscopy
Figure 1: The computer display panel of V3D System.
Image segmentation and flight path and navigation environment planning are performed automatically by the V3D processor. (It also acts as a DICOM/PACS (picture archiving and communications system) server for image archiving and retrieval). The user only interacts with the navigation or examination portion of the V3D viewer. The user has the opportunity to verify that the automated process had worked correctly. If any correction is needed, the V3D viewer provides various interactive tools to assist the user in editing the constructed colon model. The top left of the display panel in Figure 1 shows a colon model. To facilitate the user during navigation, the V3D viewer provides multiple views of the raw patient data set. Shown down the right hand side of the display panel are 2D slice views of the transverse, sagittal and coronal images. An oblique reformatted slice perpendicular to the colon centerline is shown on the bottom left corner. The colon model on the top left shows an outside “map” view with an indication of the current virtual camera position and orientation. In the center is the 3D volumetric rendered endoscopic view using the standard perspective projection and our specifically developed, fast volume rendering strategies. All of these 2D and 3D images are correlated together so the position in the 3D volume image is overlaid on the 2D slice images, and positions of 2D slices are overlaid on the 3D volume. This provides a fast, simple means to easily analyze suspicious areas in both 2D and 3D spaces. The navigation speed (for both view rendering and display response to mouse activation) is in real time. The interactive tools include, for example, the measurements of polyp size and its location
This articles was translated into Japanese and published in INNERVISION, vol.16, no.10, pp. 40-44, 2001.
A Technology Review on Virtual Colonoscopy
from the rectum, slice cutting of polyp for internal image density display, and 3D semi-translucent