Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
No job name
Proteomics: From Basic Research to Diagnostic Application. A Review of Requirements & Needs† Frank Vitzthum,*,‡ Fritz Behrens,‡ N. Leigh Anderson,| and John H. Shaw§ Dade Behring Marburg GmbH, Emil-von-Behring-Str. 76, 35041 Marburg, Germany, Dade Behring Inc.,1717 Deerfield Road, Deerfield, Illinois 60015-0778, and The Plasma Proteome Institute, P.O. Box 53450,Received March 28, 2005
For several years proteomics research has been expected to lead to the finding of new markers thatwill translate into clinical tests applicable to samples such as serum, plasma and urine: so-called invitro diagnostics (IVDs). Attempts to implement technologies applied in proteomics, in particular proteinarrays and surface-enhanced laser desorption ionization time-of-flight mass spectrometry (SELDI-TOFMS), as IVD instruments have initiated constructive discussions on opportunities and challenges inherentin such a translation process also with respect to the use of multi-marker profiling approaches andpattern signatures in IVD. Taking into account the role that IVD plays in health care, we describe IVDrequirements and needs. Subject to stringent costs versus benefit analyses, IVD has to provide reliableinformation about a person’s condition, prognosis or risk to suffer a disease, thus supporting decisionson treatment or prevention. It is mandatory to fulfill requirements in routine IVD, including diseaseprevention, diagnosis, prognosis, and treatment monitoring or follow up among others. To fulfill IVDrequirements, it is essential to (1) provide diagnostic tests that allow for definite and reliable diagnosistied to a decision on interventions (prevention, treatment, or nontreatment), (2) meet stringentperformance characteristics for each analyte (in particular test accuracy, including both precision ofthe measurement and trueness of the measurement), and (3) provide adequate diagnostic accuracy,i.e., diagnostic sensitivity and diagnostic specificity, determined by the desired positive and negativepredictive values which depend on disease frequency. The fulfillment of essential IVD requirements ismandatory in the regulated environment of modern diagnostics. Addressing IVD needs at an earlystage can support a timely and effective transition of findings and developments into routine diagnosis. IVD needs reflect features that are useful in clinical practice. This helps to generate acceptance andassists the implementation process. On the basis of IVD requirements and needs, we outline potentialimplications for clinical proteomics focused on applied research activities. Keywords: in vitro diagnostic • clinical chemistry • clinical proteomics Introduction
opportunities will emerge and that the number and value ofprotein diagnostics will increase. The latter is of special interest,
Proteomics opens new horizons in many research areas of
because reliable diagnostic information, in particular IVD data,
life sciences. This is particularly true for research efforts in the
is essential for choosing the appropriate intervention.1
field of medicine. Clinical proteomics may be defined as a
Technologies applied in proteomics research, in particular
subset of proteomics activities in the field of medicine, which
SELDI-TOF MS and protein array techniques, are thought to
promises to accelerate the discovery of new drug targets and
be moving from research-focused applications to clinical
protein disease markers useful for in vitro diagnostics (IVD).
laboratories as routine instruments for protein analysis.2 In
IVD is based on the extracorporeal analysis of tissues and body
conjunction with the routine implementation of such tech-
fluids. Thus, it is expected that new pharmaceutical treatment
nologies in the clinical laboratory it has been argued that multi-marker profiling approaches or pattern signatures will be the
† Part of the Biomarkers special issue.
next generation of protein IVD’s and shift paradigms in IVD.3
* To whom correspondence should be addressed. Dade Behring Marburg
GmbH, New Marker Research & Development, P.O. Box 1149, 35001 Marburg,
These goals and expectations for clinical proteomics should
Germany. Tel: +49 (6421) 39-4473. Fax: +49 (6421) 39-5347. E-mail:
be assessed critically in view of the role of IVD in health care.
We believe that the success of clinical proteomic marker
searches and of the technologies applied in proteomics and
their ability to enter routine IVD testing depends on the ability
Journal of Proteome Research 2005, 4, 1086-1097 In Vitro Diagnostic Requirements Impacting Proteomics
to fulfill IVD requirements and to adequately address IVD
financial resources at its disposal (List 1). A detailed discussion
needs.4 Thus, we set out to provide an industry perspective on
of these aspects is outside the scope of this article. Thus, we
the role of IVD in health care, a view of the requirements and
will focus on the crucial necessity to fulfill the requirements of
needs of IVD, and the potential implications for clinical
the IVD market and to address unmet diagnostic needs.
proteomics that should be considered, if a timely and effec-tive transfer of research results to laboratory diagnostics issought. Role of in Vitro Diagnostics in Health Care
IVD plays an essential role in health care by (1) providing
reliable information about a person’s condition and (2) sup-porting treatment decision making,5 both occurring in con-junction with a physicians’ examination, which may includeanamnesis, physical examination, and in vivo diagnostics (e.g.,computed tomography and nuclear magnetic resonance imag-ing). A third purpose, which has been proposed by McNeil andAdelstein,6 is to better understand disease mechanisms andevolution. This last purpose is outside the realm of routine IVD,but is nevertheless important, since it should provide betterIVDs that will hopefully enter that realm.
IVD tests are estimated to contribute up to 94% of the
objective data in clinical records and may influence 60-70%of critical decision making.1,7 In addition, major cost reduc-tions within the worldwide health expenditures could beachieved through a more efficient use of IVDs or better IVDs(www.VDGH.de).
Despite the importance of IVD and the essential role of the
clinical laboratory, it usually accounts for less than 5% of theexpenditures in clinics (www.VDGH.de).1,7 The proportionalshare of laboratory costs in worldwide health expenditures iseven lower, accounting for around 1% to 2% of the health carecosts (www.VDGH.de). Even so, the expenditures necessary forlaboratory diagnosis are often deemed too high, and the valueof laboratory diagnosis is very often underestimated. Addressing Diagnostic Needs Justifies the Significant
Together with the financial constraints in health care, this
Efforts for Product Development
misperception generates enormous cost pressure on clinicallaboratories and consequently on any equipment or test
The significant efforts and risks associated with product
provider that serves this market directly or indirectly. For this
development are justified, if a new test addresses major
reason, stringent cost and benefit considerations are a perma-
nent challenge in IVD and in the translation of research
Examples of major diagnostic needs are cardiovascular
applications generated by clinical proteomics into useful tests
diseases, infectious diseases, malignant neoplasms, and chronic
diseases of the central nervous system, among others. It is
Nevertheless, IVD testing represents a significant value
encouraging to see that proteomics strives to address these
proposition for improving outcomes, shortening hospital stays,
diseases,10 in particular cardiovascular diseases.11-15 Cardio-
etc. and substantially reducing the costs associated with
vascular disease, the leading cause of death worldwide (http://
healthcare. Though there will continue to be a need to justify
www.who.int/whr/2004/annex/topic/en/annex_2_en.pdf), rep-
the costs associated with IVD tests, the primary responsibility
resents a particularly telling example.
of IVD is to help reduce mortality, morbidity and improve the
Acute cardiac events and chronic heart failure both have a
quality of life. It is evident that IVD can help to save lives and
long history in the patient. There is an unquestionable need
costs (www.VDGH.de).8 There will continue to be great poten-
for early determination of disorders which might eventually
tial for improving IVDs and this dynamic offers clinical pro-
lead to these events and once they occur provide reliable
information on the event itself, about the prognosis, andadequate treatment. In the area of infectious disease, increased
Considerations Underlying Industry Perspectives and
crowding of domestic animals interacting with the ever denser
Decision Making Processes
and more mobile human population create chains of infectionswithin the species but also across species. Early diagnosis and
A decision making process in the diagnostics industry has
measures to prevent spread of infectious agents are of increas-
been outlined comprehensively by Zolg and Langen.9 From the
ing concern. As the populations of industrialized countries grow
perspective of an IVD company, new markers and technologies
to include proportionally older individuals, diseases of aging
must lead to products that improve diagnosis and also give a
like cancer and chronic disorders of the central nervous system
reasonable return on investment. Each company has to con-
are of growing importance in our society and need to be better
sider numerous factors before investing the limited human and
addressed by diagnostics and treatment measures. Journal of Proteome Research • Vol. 4, No. 4, 2005 Vitzthum et al. It is Essential to Fulfill IVD Requirements and Advantageous to Address IVD Needs
To fulfill the requirements and meet needs of the IVD market
(List 1) it is essential to provide valuable diagnostics atacceptable costs. Valuable diagnostics fulfill basic IVD require-ments, i.e., they have to accomplish the following:
(1) provide most definite and reliable diagnostic information,
that supports decisions on intervention (prevention, treatmentor nontreatment)
(2) meet objective specifications to show sufficient test
• precision of the measurement and• trueness of the measurement, and(3) exhibit the required level of diagnostic accuracy, including
Figure 1.
Dependence of the frequency of a nondiseased
population and a diseased population versus a measure shows
determined by the desired positive predictive values and
the relationship between sensitivity and specificity, decision
negative predictive values, which depend on disease frequency
thresholds (cutoff points), predictive values, and test accuracy.
For simplicity hypothetical Gaussian distributions are displayed.
From a regulatory and IVD industry perspective it appears
The measure typically denotes results of a surrogate test or a
advantageous to consider the following descriptions and
test for contributory diagnostic evidence (e.g., single and multiple
examples, which could facilitate a smoother transition of
analytes or patterns). A pathognomonic test (gold standard),
clinical proteomics findings and developments from basic
which constitutes definitive diagnostic evidence, is used to assigndiseased and nondiseased. Sensitivity is defined as true positive/
research to routine diagnostic applications.
true positive + false negative; TP/(TP + FN). Specificity is defined
Valuable Diagnostic Tests Provide Most Definite and
as true negative/(true negative + false positive); TN/(TN + FP). Reliable Information to Support the Decision Making on
Sensitivity and specificity in the populations is determined by
Interventions
the position of the cutoff point. Clearly, there is a reciprocalrelationship between sensitivity and specificity. By choosing
A diagnostic test that does not result in information that
different cutoff points a single test can be used differently. To
supports decisions on interventions, i.e., treatment, nontreat-
confirm the presence of a disease the rule-in threshold (test with
ment or prevention, including risk stratification and prognosis,
high specificity) is used while the rule-out threshold (test with
is of limited value, even if the result is interesting from a
high sensitivity) is used to exclude disease presence. To deter-
research viewpoint. The most successful tests are those that
mine the performance of a test in a population, it is important to
provide a clear-cut basis for prevention, treatment alternatives
know what proportion of positive tests correctly indicate thepresence of the disease (positive predictive value, PPV), i.e., TP/
or nontreatment. An excellent example for markers that provide
(TP + FP), and if a test is negative, what proportion indicates
definite and reliable diagnostic information impacting medical
absence of the disease (negative predictive value, NPV), i.e.,
practice is cardiac troponins (cTns).16 cTns have been demon-
TN/(TN + FN). Disease frequency, (TP + FN)/(TN + FP), i.e.,
strated to significantly improve sensitivity and specificity in the
AUCdiseased/AUCnondiseased, affects these values. For example, the
detection of acute myocardial infarction (AMI) compared to
PPV decreases with decreasing frequency of the disease accord-
other diagnostic methods, in particular the combination of
ing to (values have to be multiplied appropriately if PPV is
electrocardiography (ECG) and the traditional markers.17
supposed to be displayed in percent):21 PPV ) TP/(TP + FP) )
In this case, a new diagnostic category, known as acute
frequency × sensitivity/(frequency × sensitivity) + (1 - fre-
coronary syndrome (ACS), including AMI as the most serious
quency) × (1 - specificity)). The impact of test accuracy dependson imprecision that skews and broadens curves (not displayed)
form of the ACS, had to be established to accommodate
and bias that shifts curves (displayed as biased decision thresh-
troponin positive patients who did not meet the WHO criteria
old). Of note, when the assessment of surrogate tests is per-
for AMI that time.16 The test was able to detect real disease
formed by using only a population comprising the “sickest of
more sensitively (i.e., smaller infarcts) than previous diagnostic
the sick” and the “wellest of the well”5 one can easily imagine
methods. According to recommendations by The Joint Euro-
that diseased an nondiseased will be unrealistically separated.
pean Society of Cardiology and American College of Cardiology
The performance of the surrogate test will then usually be
(ESC/ACC) Committee a redefinition of myocardial infarction
has been proposed and ECG is still required, but no longersufficient to diagnose AMI.18 Any detectable cTn above a
usually not defined by a numerical value in terms of the
defined threshold in a patient’s circulation is a sign of myo-
measurand. It is an essential performance characteristic,
cardial damage, which requires medical intervention.16
because it is usually critical to achieve the required level ofdiagnostic accuracy (see below, Figure 1). Thus, failure to
Accuracy of Measurement is an Essential Performance
achieve sufficient test accuracy can under some circumstances
Characteristic which Encompasses Precision and Trueness of Measurement Precision of Measurement. Precision of measurement (test
The accuracy of measurement (test accuracy) is the closeness
precision) is the closeness of agreement between independent
of the agreement between the result of a measurement and a
test results obtained under stipulated conditions. Precision
conventional true value of the measurand. It includes both
depends on the distribution of random errors. The measure of
precision and trueness of measurement.19,20 Test accuracy is
precision is usually expressed in terms of imprecision. The
Journal of Proteome Research • Vol. 4, No. 4, 2005 In Vitro Diagnostic Requirements Impacting Proteomics
imprecision of measurements is the estimated random com-
established for the use as standards, calibrators, controls, the
ponent of error deduced from the statistical distribution of
verification of a measurement method, or the assignation of
repeatedly measured values. In IVD imprecision is mainly
values, e.g., conventional true values.20,21 As it is not always
expressed by the coefficient of variation (CV: standard devia-
possible to determine the true value by a measurement that is
associated with a systematic and random error, it is useful to
Precision of a distinct measurement procedure can be
define a single conventional true value that is preferentially
subdivided according to specified conditions.19
internationally accepted, e.g., as is the case with glycated
Repeatability of results of measurements can be defined as
hemoglobin.25 Instead of dealing with different “true values”
closeness of the agreement between the results of successive
depending on the method applied, physicians can rely on a
measurements of the same parameter carried out under the
single conventional true value. Thus, the implementation and
same conditions of measurement. These conditions are called
application of reference materials can help to reduce the risk
repeatability conditions. Repeatability conditions include the
of uncertain or incorrect data interpretation.
same measurement procedure, the same observer, the same
Usually, highly purified chemicals are weighed out for the
measuring instrument, used under the same conditions, the
preparation of a solution with a specified concentration or for
same location, and repetition over a short period of time.
the calibration of solutions of unknown strength. A secondary
Repeatability is often termed in laboratory medicine "within-
reference material usually contains one or more analytes in a
run” imprecision, a term now considered obsolete.19
matrix that reproduces or simulates the expected. The values,
Reproducibility relates to change in conditions, i.e., different
e.g., conventional true values, have been assigned by a formal
laboratories, instruments, operators, and measuring systems
process of value transfer from a primary reference material.
(calibrants, reagent batches, etc.), a wide range of patient
Certified reference materials (CRM) are usually also matrix
samples exhibiting unusual features and is often termed
based and have one or more of its values certified by a
interlaboratory imprecision or total imprecision. The term total
technically valid procedure. CRMs are accompanied by or
imprecision is likewise considered obsolete.19
traceable to a certificate or other document of a certifying body.
It is important to note that IVD precision figures are typically
Standard reference materials are CRMs and a trademark name
given as interlaboratory precisions, a much wider scope of
of the National Institute of Standards and Technology. Tertiary
variation than covered by usual proteomics studies, which
reference materials are typically industry standards, calibrators,
typically deal with precision within a run in one laboratory.
and controls that contain one or more analyte in an appropriate
Even so, total interlaboratory test imprecision in IVD is typically
matrix. The concentration of the analytes is usually based on
in the range of 1.5-10% CV (much less than typical values
Objective Test Accuracy (Both Trueness and Precision of Trueness of Measurement. The trueness of a measurement Measurement) Specifications Have to be Met in IVD. For
is the agreement between the average value obtained from a
established diagnostic tests, objective test accuracy specifica-
large series of test results and a nationally or internationally
tions are available to judge analytical performance character-
accepted reference value (true or conventional true value). It
istics.26 Specifications may be derived from professional
denotes the systemic error component, expressed as bias.19,20
recommendations, e.g., guidelines from international, national
Reference materials and reference methods are the best
expert groups, institutional groups, expert individuals, from
guarantee for correct calibration and thus trueness of measure-
regulatory and legislation authorities, from organizers of ex-
ment.20 A reference method or reference measurement proce-
ternal quality assessment schemes and proficiency testing
dure is defined as a thoroughly investigated measurement
programs or simply from published data on the state of the
procedure, clearly and exactly describing the necessary condi-
art. For example, for cTn assays a CV of 10% reproducibility at
tions and procedures, for the measurement of one or more
the 99th percentile limit is suggested.27 The 99th percentile of a
property values that has been shown to have trueness of
reference control group denotes the decision limit. A percentile
measurement and precision of measurement commensurate
is a value on a scale of one hundred that indicates the percent
with its intended use and that can therefore be used to assess
of a distribution that is equal to or below it. cTns indicate
the accuracy of other measurement procedures for the same
myocardial necrosis when the maximum concentration exceeds
property(-ies), particularly in permitting the characterization
the decision limit on at least one occasion during the first 24
Of note, reference methods do not necessarily represent
Test accuracy specifications may also be assessed through
internal/procedural controls that may be used together with
the impact of the trueness of a measurement expressed as bias
external controls in laboratories for quality control purposes.24
and the imprecision of a measurement on diagnostic sensitivity
Internal/procedural controls are designed into a system to
and specificity and the consequences for clinical decision
monitor one or more components of errors including errors
making for specific clinical situations.28 More general test
of the analytical process (e.g., reagent function), operator
accuracy specifications refer to the two major IVD scenarios,
variance (e.g., sample processing and handling), and environ-
i.e., (1) monitoring individual patients and (2) diagnosis using
mental factors (e.g., variations in temperature, humidity).
reference intervals. Here, test accuracy specifications may best
External controls are not designed into a test system. They are
be based on the components of biological variation within
materials similar to patient samples with expected properties
subjects (CVI) and between subjects (CVG). A common view is
commercially prepared or inhouse prepared samples, profi-
that imprecision of a measurement should be below 0.5 × CVI
ciency test samples with confirmed results, reference or control
organism strains, patient specimens with established values
Of note, a test has to be sufficiently robust and specific to
previously tested, and control materials (other than those lots
cope with matrix effects and interferences and still fulfill the
used to calibrate the system, i.e., standards). Reference materi-
required specifications of precision. Interferences or interfering
als are materials or substances with properties that are
substances are often considered to be components of the
Journal of Proteome Research • Vol. 4, No. 4, 2005 Vitzthum et al. Table 1. General Test Accuracy Specifications Including Both, Imprecision of the Measurement and Trueness of the Measurement (expressed as bias)26a a Specifications depend on within-subject (CVI) and between-subject (CVG) variations.
sample that contribute to the measurement signal, e.g., he-
a marker.30 This together with matrix effects from the other
moglobin in specific photometric analyses. Matrix effects do
constituents of the respective sample have a significant impact
usually not contribute directly to the measurement signal but
on diagnostic performance and obviously on the success of
indirectly through physical or physicochemical properties of
research activities, too.21,31-33 Biological specimens used for
the sample, e.g., viscosity, adsorption processes, reaction
diagnosis include whole blood, serum, plasma, urine, cere-
brospinal, synovial, amniotic, pleural, pericardial, peritoneal,
Test precisions of clinical analyzers may be used as an
cervical, seminal fluids, nipple aspirates, sweat, saliva, exhaled
orientation guide for precision specifications, too. For example,
air, various types of solid tissues, feces, etc.34,35 Serum is the
in a multicentric evaluation of analytical performance of 33
specimen most frequently applied in IVD followed by different
protein assays a dedicated immunoassay analyzer exhibited a
plasma types and urine,36 while the pathology laboratory
median total CV of 3.4% with a 2.5th and 97.5th percentile of
generally requires tissues and cells, e.g., erythrocytes, platelets,
the imprecision distribution at 1.3% and 13.0%.29
lymphocytes, etc. for cytopathological investigations. It is Advantageous to Address Needs that Contribute to the
Every specimen type has its pros and cons with respect to
Overall Performance. Besides the requirements regarding test
the scope of a study and the technologies applied. There is no
accuracy, it is advantageous to address needs that contribute
such thing as a universal or ideal specimen type that could be
to the overall performance characteristics (List 1). Costs as-
generally recommended. Often, it is necessary to work with the
sociated with a test, including the instrument and consumables,
specimens that are available anyhow. However, if possible, one
which may be summarized in terms of cost per reportable
should avoid choices of specimens and processing procedures
result, are important factors for the acceptance of a test and
that inherently preclude some future analysis. Blood is easily
have to be balanced in view of potential savings achieved by
accessible and there are usually no contraindications to a
performing a test. Depending on the field of application,
standard blood draw. Serum and plasma display moderate
features such as ease of use, degree of automation, throughput,
variability if compared to other specimens such as urine.
turn-around-time, menu breadth, open channels (for nonpro-
Nevertheless, serum and different plasma types exhibit signifi-
prietary tests), instrument footprint, connectivity to the labora-
cant variability. On the other hand, they are considered to
tory information management system, service quality and
mirror best the whole human proteome.37 Serum allows for
continuity have to be addressed. In conclusion, tests, assay
various testing including electrolytes, proteins, peptides, me-
formats and instruments have to fulfill objective quality
tabolites, etc. This is particularly advantageous, if additional
specifications and should be at least compatible with the state
testing (“adds on”) as a consequence of a first result is required,
because it may eliminate the need of additional blood draws
The compatibility of a new test’s format with existing
and thus saves time. To have maximal freedom of testing and
diagnostic test processes, i.e., preanalytics, actual analysis, and
because of limitations regarding the draw of various different
post-analytics, may also factor into the overall performance
specimen types, ideally one specimen type should be applicable
characteristics. Preanalytical processes include the order of the
for all determination. However, some blood constituents
test(s) based on the physician’s request to support diagnosis
require special collection and storage conditions.38
of a patient, sample collection, transportation of the sample,
Plasma, in particular heparinized plasma, is preferred when
accession of the sample into the laboratory, processing of the
a quick answer is critical, because clotting time is saved.
sample (e.g., centrifugation, sorting, aliquoting, loading of the
Citrated plasma is mainly applied for coagulation analysis.
instrument), reagent setting and calibration of the instrument,
Anticoagulants, preservatives, and other additives influence the
and match ordered test(s) and sample. Post-analytical processes
composition of the specimen and may interfere with certain
include approval of test results, their collection, transmission,
analysis.21,38 Thus, it is of importance to carefully select the
appropriate display (e.g., charts) and documentation, waste
application of these compounds in blood collection tubes or
disposal, sample storage, inventory, and order management,
their addition at a later point after the collection process.30,35
The collection of a specimen is crucial, too.32,33 For example,
Some of the processes mentioned above are of particular
for blood specimens it is important to consider how the blood
importance for proteomic studies. First, it is crucial to have
was drawn. Factors such as timing of collection, position of
detailed information on the donor, e.g., on gender; age; dietary,
the patient (lying, seated) and the time period the patient was
smoking, alcohol consumption and other habits; patient his-
in this position (impacting hematocrit), stress for the patient
tory; medication; pregnancy; post/pre-menopausal; suspicion
associated with the blood collection, type of collection (veni-
or confirmed diagnosis of disease(s); clinical laboratory results;
puncture, arterial puncture, skin puncture, etc.), site of collec-
tion and its preparation (e.g., cleaning of the site), tourniquet
The specimen type used, its collection, transportation,
technique (e.g., time of venous occlusion), order of sampling
processing, storage, etc., and the respective stability of a marker
(first, second, third tube), the quantity of blood withdrawn (e.g.,
can dramatically influence the concentration and integrity of
dilution of citrated plasma), and obviously the person who
Journal of Proteome Research • Vol. 4, No. 4, 2005 In Vitro Diagnostic Requirements Impacting Proteomics
draws the blood impact the composition of the specimen. Thesame is true for parameters of collection devices or collectionsets applied, e.g., needle gauge, single draw or multi-drawneedles, and bag or tube types applied. Here, the material (glassor plastic) should be considered as well as other features suchas siliconized tubes (potential activation and acceleration ofclotting, reduction of adhesion of clots), gel or nongel separa-tors (gel serves as a mechanical barrier, which eliminates thechanges that occur when the clot or cells are in contact withserum or plasma), and additives such as clotting coagulantsand preservatives.
The main factors that should be considered upon transpor-
tation are timing and temperature among others. Processingtechniques may also impact the quality of a specimen.32,33 Thecoagulation process to gain serum may depend on volumes,clot activator (type, concentration), clotting time, and temper-ature. G-force, duration and temperature are factors that haveto be considered upon centrifugation of serum and plasma. For plasma samples activation of platelets at low temperatures
Figure 2. Receiver operating characteristic (ROC) curves are used
can be an issue. Also, platelet depletion and the technique
to determine the diagnostic accuracy of an assay. When popula-
applied (second centrifugation step or filtration) may be
tion overlap completely, no differentiation between diseased and
considered.32 Storage is another important aspect. The influ-
nondiseased is possible (dotted line), leading to a useless test
ence of freezing and thawing procedures, storage formats,
with an AUROC of 0.5. When there is no overlap, the ROC curve
temperature and duration as well as repeated freeze and
superimposes along the axes (dashed line). This perfect test has
thawing can significantly impact the quality of specimens.32,33,39
an AUROC of 1. Typically, there is a distinct overlap of popula-
In conclusion, to ensure a high degree of consistency and
tions as outlined in Figure 1, which creates ROC curves between
to reduce the risk of error in subsequent analyses, strict
the two extremes, e.g., the displayed hypothetical curve (solid
adherence to optimized protocols or standard operating pro-
cedures is mandatory for each sample throughout the whole
or 95% confidence intervals, because this gives a clearer picture
process, which has to be subject to thorough quality assurance
of the strength of the data.47 Details have been extensively
and control procedures including documentation.40-45
AUROC: A Measure of Diagnostic Accuracy. A summary Diagnostic Accuracy: The Ability to Discriminate States
measure of diagnostic accuracy is the area under the ROC curve
of Health and Disease
(AUROC), which incorporates sensitivity and specificity. Itrepresents the overlap between the healthy and diseased
The diagnostic accuracy, i.e., diagnostic sensitivity and
population. An AUROC of 1 would represent a perfect diag-
diagnostic specificity, of a test is its ability to discriminate
nostic accuracy (no population overlap) and an AUROC of 0.5
between alternative states of health and disease. Frequently,
would represent no difference between groups (no diagnostic
there are more than two states to be differentiated. However,
value). It is rather unlikely that a diagnostic test reaches an
the clinical question can often (but not always) be dichoto-
AUROC of 1, because it is hardly possible to select a medical
mized where the objective is to separate patients into two
decision level or cutoff point that completely discriminates
groups based on the presence or absence of a certain disease
between two groups. Thus, the major challenge of IVD tests
(Figure 1). In 1971, Lusted postulated that the measure of the
lies in the selection of the right cutoff points, i.e., sacrifice
performance of the observer measures the worth of a diagnostic
sensitivity for specificity or vice versa.
test and that receiver (or relative) operator characteristic or
Of note, complex diseases, where it is necessary to differenti-
receiver operating characteristic (ROC) curves (Figure 2) pro-
ate multiple disease states, co-morbidities or mimics, and
vide an ideal means of studying observer performance.46 Since
chameleons usually hamper the finding of efficient cutoff points
then, ROC curves have been widely used to determine the
to achieve high diagnostic accuracy. In addition, these diseases
diagnostic accuracy of a test in IVD and clinical proteomics.
often exhibit complex time-dependent physiological or patho-
Receiver Operator Characteristic (ROC) Curves: Sensitivity
logical processes, which may aggravate the finding of single
versus 1-Specificity. To outline major challenges associated
IVD markers useful to differentiate states. For example, it is
with laboratory tests and clinical proteomics approaches, basics
challenging to find IVD marker(s) to rule-in ischemic stroke
of diagnostic performance measures are briefly outlined. ROC
within the first 3 h after onset of symptoms, which is the
curves represent graphically the inverse relationship between
treatment window for thrombolytic therapy. As the acquisition
specificity or 1-specificity and sensitivity (Figure 2). Sensitivity
of cerebrospinal fluid is usually contraindicated serum or
is the ability of a test to detect the condition of interest, for
plasma markers are needed. The crossing of the blood-brain-
example the number of true positives of an affected group, i.e.,
barrier by potential brain specific markers into the circulation
detection of disease when it is truly present. Specificity is the
within a short time frame and eventual renal clearance
number of the true negative results of the unaffected group,
processes challenge the finding of appropriate markers. Finding
i.e., recognition of condition absence when it is truly absent.
a rule-in marker for ischemic stroke is also challenging, because
1-specificity is the number of false positives. As the reliability
of the heterogeneous etiology of stroke. Ischemic strokes have
of determinations of sensitivity and specificity depend on the
to be discriminated from hemorrhagic strokes (subarachnoidal,
size of the chosen population, it is essential to provide the 90%
intracranial) and transient ischemic attacks and multiple
Journal of Proteome Research • Vol. 4, No. 4, 2005 Vitzthum et al.
mimics such as alcohol withdrawal, hypoglycemia, intoxication,
approaches of multi marker testing in the diagnostic labora-
seizures (epileptic), amnesia, multiple sclerosis, migraine,
tory: (1) the series approach, i.e., test A is applied first and all
tumors, closed head injuries, infections, and inflammatory
those specimens with a positive result are retested with test B
processes (meningitis, encephalitis, abscesses). This example
or vice versa, etc., or (2) the parallel approach, i.e., tests A and
also clarifies, why laboratory diagnosis is often based on the
B are measured at once. The advantage of serial testing is the
typically positive impact on pretest probability and conse-quently on PVs and its cost-effectiveness, in particular for the
Predictive Values Display How a Test Will Perform in a
screening of large populations for a rare condition, because
Population and Denote the Probability of the Patient to
most patients receive only one test. The potential disadvantage
Have the Diagnosed Condition
is the delay in treatment while waiting for the results of
To assess the diagnostic accuracy of a test when applied to
a population, the effect of disease frequency has to be
There are different ways in which test results can be
considered. Critical parameters of the diagnostic performance
combined, e.g., by the OR rule or the AND rule.49 For parallel
of a test are predictive values (PVs). The PV of a positive test
result (PPV) is the percentage of patients with positive test
OR rule: The diagnosis is positive, if either test A or test B is
results that are diseased. The PV of a negative test result (NPV)
positive. Both tests must be negative for the diagnosis to be
is the percentage of patients with negative test results that are
nondiseased. PVs are not measures for the intrinsic diagnostic
AND rule: The diagnosis is positive only, if both test A and
accuracy of a test, they are a function of both the sensitivity
test B are positive. Either test A or test B can be negative for
and specificity of a test and the frequency of a disease (see
text of Figure 1). Whether prevalence or incidence is more
When the serial testing process is performed the common
adequate to determine predictive values is determined by the
particular application. The incidence of a disease is the number
OR rule: If the first test is positive, the diagnosis will be
of cases that arise during a distinct period of time in a given
positive; otherwise, the second test is performed. If the second
population. The prevalence is the frequency of the disease at
test is positive, the diagnosis will be positive; otherwise, the
a certain point in time in a given population.
As the decrease of disease frequency goes along with a
AND rule: If the first test is positive, apply the second test.
decrease of the PPV, even tests with high sensitivity and
If the second test is also positive, the diagnosis will be positive;
specificity fail as screening tests when applied to the general
otherwise the diagnosis will be negative.
population with a low disease frequency. For example, the
The sensitivities and specificities for the OR rules and the
comparatively low prevalence of distinct cancers is one of the
AND rules are the same for the parallel and the serial ap-
reasons, why it is so difficult to implement cost-effective cancer
proach.49,51 For the OR rule, the sensitivity is higher than either
screening tests as routine screening tools. Even the prostate
specific antigen (PSA) test, the only FDA-approved serum IVD
specificity is lower than either test individually (Sp
cancer screening test to-date is questioned to be useful as a
SpA ∪ SpB). With the AND rule it is vice versa. The specificity is
prostate cancer screening tool, because of the limited predict-
higher than either test individually (Sp +
ability and the absence of prognostic value. Elevated PSA values
SpA ∪ SpB), but the sensitivity is lower than either test
do not tell, if the cancer is aggressive or not and if any surgery
would save years of life at the cost of significant morbidity. In
The AND approach appears attractive to exclude the pres-
view of these aspects and because of the heterogeneity of
ence of a disease, because sensitivity is increased, though as a
cancer, it is an extremely difficult charter, to find routine
tradeoff, specificity is lower. When negative, these AND testing
screening markers for distinct cancer types. But as cancer is
profiles may have a high NPV. Therefore, they are useful for
one of the leading causes of death (http://www.who.int/whr/
clinicians to rule-out a variety of diagnoses. In the diagnostic
2004/annex/topic/en/annex_2_en.pdf) and as early, pre-
workup, the OR approach may be preferentially performed.
symptomatic diagnosis dramatically improves the odds of
This approach is very predictive of the presence of a particular
successful treatment, there is undoubtedly an unmet diagnostic
disease, confirmation or rule-in, because of the high specificity.
Of course, when more than two tests are applied a flexible
Clearly, the results of a diagnostic test cannot be assessed
combination of series and parallel testing and the OR or AND
properly, without knowing the probability of the condition
rule may also be performed. Nevertheless, even the use of
before the test is performed.5 However, the PVs are post-test
multiple tests of independent markers does not resolve the
probabilities of the condition (revised or posterior prob-
tradeoff between sensitivity and specificity21 and issues associ-
abilities). When a patient’s history, signs and symptoms, or
ated with positive and negative predictive values.
results of independent diagnostic tests performed previously
Here, it should be noted that a set of observations can also
are available, the pretest probability (the probability of the
be considered as a single multivariate observation (patterns or
condition before the test is applied) has to be taken into
profiles) and interpreted as such by a multivariate comparison.
account. The determination of the pretest probability, e.g., by
A multivariate reference or decision region can prevent the
Bayes’ theorem, is beyond the scope of this article. It has been
addition of false-positive results, which is usually the case for
extensively reviewed elsewhere.5,21,49,50
the performance of multiple, univariate comparisons. Thegeneration of algorithms to efficiently combine diagnostic
Different Approaches to Perform and Combine Multiple
information, e.g., by neuronal networks, has been shown to
According to the aspects mentioned above, two or more tests
The contribution of the diagnostic accuracy of single or
are often performed to diagnose patients. There are two basic
multiple laboratory tests has to be seen in concert with
Journal of Proteome Research • Vol. 4, No. 4, 2005 In Vitro Diagnostic Requirements Impacting Proteomics Table 2. Purposes for the Application of IVD Tests or Respective Marker Types Acute markers are used when an acute disease event occurs and
cTns that are used to rule-in AMI and B-type natriuretic peptide
should help in the process of differential diagnosis to provide
(BNP) and N-terminal pro BNP (NT-proBNP) to rule-out heart
the information necessary for a specific treatment.
failure in patients with acute dyspnoe.16,78
Screening markers identify diseased preferentially in an asympto-
The detection of protein in urine, in particular albumin, is a
matic stage within a population to start treatment as soon as
possible, which usually goes along with a high treatment success. Generally, screening markers are applied in population subgroupswith increased risk and disease frequency to achieve adequate PVs. Primary risk assessment markers are used to assess the risk of
Total cholesterol, triglycerides, LDL cholesterol, HDL cholesterol,
a healthy individual to suffer from a disease in the future.
high sensitivity C-reactive protein (hsCRP), among others aremarkers used for primary cardiovascular risk assessment.53,55
Secondary risk assessment, prognostic or progression markers
Cardiac troponins are used in the secondary risk assessment for
are used to determine how the disease may potentially
AMI patients as an indicator for the risk of adverse outcomes,
develop, the risk of a diseased patient to suffer recurrent
i.e., morbidity and mortality.16 As primary risk assessment
markers, secondary risk assessment markers help to determineaggressiveness of a treatment and balance the benefits andside effects. Disease staging or classification markers help to classify
Determination of certain proteins in urine, kidney and urinary
tract diseases can be classified into prerenal, renal,and postrenal.79
Treatment response stratification markers are used to predict
Hemostasis markers may be determined before a distinct anti-
the likeliness of a response to a pharmacon before its
coagulation therapy is started.22 Viral resistance markers and
application to prevent adverse effects and to initiate
antibiotics resistance testing in bacteria are further examples.
the most effective therapeutic treatment. Treatment or therapeutic monitoring markers are used to
Blood lipids are applied to follow the impact of exercise, nutrition,
determine and monitor the effectiveness of a treatment.
and eventually therapeutic interventions. Therapeutic drug monitoring is based on the determination of
Immunosuppressive drugs, like sirolimus, everolimus, tacrolimus,
pharmaca administered to treat a patient. In this sense, it is
and cyclosporin A, have to be monitored closely to prevent
not a marker type, but listed for the sake of completeness.
graft rejection and to minimize adverse therapy effects.75
Compliance markers provide information on treatment
Glycosylated hemoglobin A (HbA1c) can be used to monitor
insulin therapy compliance80 and carbohydrate deficienttransferrin (CDT)81 may be applied to control compliancewith alcohol withdrawal therapy.
complementary diagnostic information to support precise
concentrations of CRP indicate acute inflammatory processes.54
treatment decision making, too. As outlined above, patient
whereas persistent low concentrations of CRP are used as a
information from the physicians’ examination are crucial. For
primary cardiovascular risk assessment marker.55 cTns are
example, parameters such as age, smoking, high blood pres-
applied as acute markers for the event (AMI) itself, to determine
sure, family history of myocardial infarction, diabetes mellitus,
the size of the damage, and they also provide prognostic
etc., in concert with laboratory markers such as LDL choles-
terol, HDL cholesterol, and triglycerides, among others, aremajor factors included in algorithms for the risk assessment
Tests for Definitive Diagnostic Evidence, Surrogate Tests, and Tests Providing Contributory Diagnostic Evidence
Tests are also classified by their role in the diagnostic
Requested Diagnostic Information Determines the
process56 as pathognomonic tests, surrogate tests, and tests that
Required Diagnostic Accuracy
provide contributory diagnostic evidence. Obviously, this clas-
As outlined above, the disease type, its complexity, and its
sification may not be entirely clear-cut in practice.47 Pathog-
frequency within a given population, determine diagnostic
nomonic tests (tests for definitive diagnostic evidence) are
accuracy requirements and how to perform and combine
defined (or assumed) to uniquely define a disease and are used
multiple tests to achieve appropriate PVs. Thus, diagnostic
in the classification of diseased and nondiseased. Therefore,
accuracy requirements are also determined by the requested
these tests are used as “gold standards” to assess the diagnostic
diagnostic information or marker type, because this determines
accuracy of alternative tests (Figure 1). By definition a patho-
disease frequency and degree of differentiation between disease
gnomonic test displays the highest attainable diagnostic ac-
states. Different diagnostic applications of disease-specific
curacy. Clearly, this assumption can only be validated by
proteins have been outlined comprehensively by Zolg and
comparison to a less well-established test, which may subse-
Langen.9 Main IVD marker types are presented in Table 2.
quently be shown to better uniquely define the disease.47
In most cases of laboratory diagnosis, the same analytes can
Usually, the pathognomonic test, e.g., a biopsy, is expensive,
also be used for different diseases and as different marker types
elaborate, time-consuming, unpleasant for the patient, or
(Table 2) to obtain different diagnostic information. For
associated with a morbidity or even mortality risk. A surrogate
example, CRP is the classic acute phase protein.54 High
test is used as a substitute for a pathognomonic test. A test for
Journal of Proteome Research • Vol. 4, No. 4, 2005 Vitzthum et al.
contributory diagnostic evidence contributes to, but does not
for optimization of individual assay performance to reach
establish itself, a diagnostic decision. Typically, surrogate tests
specifications, regarding specimen types, concentration range,
or tests for contributory diagnostic evidence are inexpensive,
precision of the measurement, trueness of the measurement
less unpleasant for the patient, and display little association
(calibration and traceability to reference materials), correlation
with morbidity or mortality. On the other hand, they are
to other methods (in particular reference methods), cross-
associated with diagnostic inaccuracy.
reactivity, matrix effects and interferences, e.g., hemolysis(which generates a red color interfering with some colorimetric
Discovery, Confirmation and Exclusion Tests
assays), icterus (in which high levels of the yellowish pigmentbilirubin interfere), lipemia (in which turbidity from lipoprotein
Pathognomonic tests, surrogate tests or tests providing
particles interferes with some optical measurement tech-
contributory diagnostic evidence may be classified as outlined
niques), interfering antibodies in the sample (which can, for
in Table 2. Their use for the discovery, confirmation or
example, bind directly to one of the antibodies in a sandwich
exclusion of a disease allows for another level of classification.57
immunoassay and give a false signal) and other substances.
A discovery test is used in disease screening (Table 2), a
Standardization, quality control and assurance including de-
confirmation test to confirm (rule-in, test with high specificity)
tailed and appropriate documentation, if possible according
a suspected disease, and an exclusion test to exclude (rule-
to standard operating procedures40-45 is of particular impor-
out, test with high sensitivity) the presence of a suspected
tance for preanalytical processes to provide samples of high
disease. By applying different decision thresholds (cutoffs or
quality, but obviously important for the subsequent diagnostic
cut-points) more than one of these purposes can be served by
a single test and the respective marker (Figure 1). When a
For an initial search for marker candidates, a phase I study,
disease is serious and should not be missed, a disease is
it may be legitimate to focus on the most prominent disease
treatable, false positive results do not have serious psychologi-
states and keep the sample number to a minimum. The
cal or economic consequences for the patient, e.g., neonatal
number of samples needed for a phase I study depends on the
screening for phenylketonuria or hypothyroidism, an exclusion
conjectured diagnostic accuracy and the ratio of diseased
test is used. When a disease is not treatable or curable, the
knowledge that the disease is absent is reassuring to the patient,
Proteomics appears to be a useful tool for such initial studies,
and false positive results have serious psychological or eco-
because it provides information on a huge number of proteins
nomic consequences for the patient, e.g., multiple sclerosis and
and protein variants at once. To facilitate transition to routine
advanced carcinoma, the confirmation test is used.47
diagnosis with its requirements for diagnostic accuracy and testaccuracy, it is advisable to switch to an assay format or
Potential Implications on Applied Clinical Proteomics
instrument for subsequent study phases, which is routinelyused in the diagnostic laboratory, e.g., switch from MS to ELISA.
If a smooth transition of clinical proteomics findings and
developments to routine diagnosis is desired, then it is impor-
This also applies to multi-marker approaches, if a reasonable
tant to fulfill IVD requirements and address needs (see above
number of markers to be combined is not exceeded. The tests
and List 1). The requirements and needs should be considered
can be performed serially or in parallel and the reported results
differently depending on the objective.
can be combined by the AND or OR approach as well asmultivariate analyses with high flexibility including other testtypes, e.g., electrolytes, functional hemostasis test, etc. and of
Considerations for the Search for New IVD Markers
course additional diagnostic information, e.g. age, gender, body
The choice of the disease, the desired diagnostic information
or marker type (Table 2), and the performance of any existing
The validation, including subsequent study phases, will
diagnostic procedures determine the diagnostic accuracy that
establish the value of emerging markers, alone or in combina-
has to be achieved by tests based on a single or multiple new
tion, and show if they are robust enough to move to IVD.
marker(s). It is also advisable to consider that the initial search
Validation may be defined as documented evidence that the
for new IVD markers should allow for transition to routine IVD
specific, unequivocally described method, process, or technol-
instruments (typically as immunoassays) and preferentially lead
ogy, operating within the established parameters, performs
to serum or plasma tests of the marker candidates, if the marker
effectively and reproducibly to produce a result that meets
is supposed to be tested in the clinical laboratory. This does
predetermined specifications and quality attributes within given
not necessarily mean that serum or plasma is always the
variations with a high degree of statistical assurance.
primary choice of specimen for the initial search for new
In phase II studies, accuracies of two or more diagnostic tests
markers. Concentration issues and other considerations may
are often compared. Patients difficult to diagnose with early
propose to start with solid tissues or other fluids.58,59 If a new
or atypical disease, other conditions that might interfere with
marker requires a new technology platform, then its use will
the test, and controls with conditions that mimic the disease
be substantially delayed while the clinical laboratory com-
of interest challenge the candidates.
munity evaluates the platform and investigates the economics
The hurdle in phase III studies is usually to assess and
of the test. Typically an investment in a new platform is not
compare diagnostic accuracy of different tests. Here, the value
justified if it provides only a single new test.
of a test is determined in a defined but generalizeable popula-
The preanalytical processes, i.e., acquisition of the sample
tion, i.e., in a clinical trial with a large cohort of patients with
and its handling, should be transferable to the routine environ-
the selection of appropriate controls.48 The costs of such studies
ment. Thus, acceptance of a marker whose routine detection
are a major issue when one considers that the margins in the
required a novel method of serum collection would be inhibited
diagnostic industry are much smaller than the margins in the
in comparison to an equivalent marker measurable in standard
pharmaceutical industry. Also, the pressure of the funding
serum or plasma. The single immunoassay test per tube is ideal
bodies appears to be greater for diagnosics. Journal of Proteome Research • Vol. 4, No. 4, 2005 In Vitro Diagnostic Requirements Impacting Proteomics Transition of Technologies Applied in Proteomics
will be necessary to generate adequate and more complex
Research, Namely Protein Arrays and Mass
controls and standards, and ultimately reference materials. Spectrometry, to Routine IVD
The manufacturing process will be more complex, but one
may expect an increase of the overall efficiency with respect
One of the major challenges of technology transition from
to the manufacturing time and costs through consolidation of
proteomics research to IVD is the test accuracy, both precision
multiple tests in a single package. However, lot to lot variability
and trueness (see above). To prove test accuracy, it is necessary
and stability of spotted arrays could be an issue. Quality control
that the technologies applied enable the application or estab-
will be more difficult and troubleshooting of failures becomes
lishment of guidelines and standard operating procedures32,60
more complicated. Final quality control failures for single
in concert with quality control, quality assurance, and stan-
analyte performance will compromise the entire product. The
dardization measures, e.g., by applying reference material.61
batch processes used to manufacture beads, e.g., for “bead
The establishment of or the correlation to reference materials
arrays”, at least partially circumvent some of these issues.
and reference methods are the best guarantee for correct
Third-party patents frequently have to be accessed before
calibration and thus trueness of measurement20 to meet
commercial use of technologies, tests, reagents (e.g., antibodies
specifications, e.g., those of Table 1. This is particularly
or antigens) applications, etc. Availability of licenses and costs
important for the establishment of common reference intervals
may restrict the number of components that can be employed
and cutoff points to allow for harmonized clinical decision
for a given multi-marker array and thus hamper its application
making and disease management. Patient monitoring over time
in IVD. The inhibiting effect of “royalty-stacking”, well-known
is one example that does clearly illustrates the requirement of
in the pharmaceutical industry may become especially signifi-
high test accuracy, in particular trueness of the measurement
that has to be maintained over time. The application and
From a regulatory perspective more complex evaluations and
implementation of reference materials in proteomics as cur-
validations, which include the assay format and the instruments
rently applied in IVD may be one of the first steps to account
themselves, will require large cohort studies and significant
for this challenge. A review on reference materials and the
registration efforts. Recalls of the whole system due to inap-
benefits of their application in clinical proteomics is beyond
propriate performance of a single component affect customers’
access to multiple tests. Different reimbursement rates and
The parallel measurement of many different proteins is the
usage of the single analytes, the combination of markers, or a
inherent characteristic of technologies applied in proteomics
distinct microarray, also in view of regional distinctions, could
research. The yet unresolved questions are due to the extremely
also hamper the application of microarrays. The flexibility of
different concentrations of the proteins to be measured in a
the customer to perform serial testing or only testing a subset
very complex matrix like serum. A vivid example in inflamma-
of tests is impaired with regard to financial trade offs, too.
tory processes is the simultaneous determination of the
Mass Spectrometry in IVD: Challenges Associated with the
abundant haptoglobin (Hp) (adult serum or plasma reference
Detection of Proteins and Protein Profiles and a Successful
intervals calculated in relation to IFCC/BCR/CAP Certified
History of the Determination of Low Molecular Weight
Reference Material 470 are 0.03-0.20 g/L for Hp 1-1and Hp
Compounds. Some of the aspects outlined for arrays (see
2-2, and 0.04-0.20 g/L for Hp 2-1) and the traces of inter-
above) also apply to MS technologies, in particular to those
leukin 6 (serum or plasma reference interval < 10 ng/L).
that use arrays or chips such as surface-enhanced laser
An interesting feature of the technologies applied in pro-
desorption/ionization time-of-flight (SELDI-TOF) MS. Recently,
teomics research, is the application of small sample volumes
Aivado et al.64 demonstrated that automation, analysis of
down to a few microliters. However, this is currently not critical
replicates, and standardization of the drying process signifi-
in routine IVD since most current-generation clinical analyzers
cantly decreased imprecision of SELDI-TOF MS protein analy-
require less sample and reagent volumes than was previously
ses. After optimization CVs ranged from 25.7% to 32.6%
depending on the signal-to-noise ratio threshold used. Even
The decision to apply single laboratory tests on standard
though lower imprecisions for SELDI-TOF MS protein analyses,
instruments optimized for each protein or microarray or MS
e.g., CVs less than 10% have been reported,65 in view of
technologies will probably depend on the number and type of
precision requirements (see above and Table 1) further im-
different proteins that need to be measured in parallel to
provements are required for the application of SELDI-TOF MS
provide a diagnostic result, the diagnostic accuracy and the
However, as the SELDI-TOF MS approach is thought to
Challenges for Protein Array Technologies. High density
generate profile signatures that correlate to a disease, it will
protein arrays may be suited for high throughput screening and
be interesting to see to what extent profile signatures and
discovering initial correlations, but low density arrays seem to
algorithms improve diagnostic accuracy.2,3 This improvement
be more likely to reflect some aspects of IVD requirements and
will need to be substantial to compensate for the lack of
needs.62,63 Performance, manufacturing, intellectual property
accuracy in the measurement of individual analytes, as well as
issues, regulations and application challenges should be ad-
many additional issues associated with SELDI-TOF MS analysis
dressed for a smooth introduction of this technology into the
and studies that have been extensively discussed elsewhere.66-71
The concept of profiling has a long history in laboratory
Performance specifications (see above) like test precision,
medicine (e.g. serum protein electrophoresis), and thus it is
compatibility of multiple assay components, compatibility of
not a shift in paradigms3 but it could rather be expected that
concentration ranges of the different analytes, cross-reactivities,
novel profiling approaches, e.g., via MS technologies, would also
matrix effects, and interferences appear to be especially chal-
contain diagnostic information. Especially, as it may appear
lenging when different proteins are to be measured in parallel
unlikely that a single marker will be sufficient to adequately
in a single vessel. To achieve test trueness, significant efforts
diagnose complex diseases in its early phase (see above). Journal of Proteome Research • Vol. 4, No. 4, 2005 Vitzthum et al.
On the other hand, the number of distinct discriminators
are sufficiently daunting that quantitative mass spectrometry
commonly found in profiles65,67,69,71 reveals that a few signals/
may have value as an additional format for multiplexing protein
markers are usually sufficient for diagnosis. This may eliminate
measurements in the future given aggressive technology de-
the need for complete pattern or profile information for routine
IVD applicationssthe needles within the haystack are ofinterest, not the haystack itself that actually obstructs the view
References
on the needles. Consequently, a limited number of singleimmunoassays whose individual results are combined by an
(1) Forsman, R. W. Clin. Leadersh. Manag. Rev. 2002, 16 (6), 370-
algorithm would be sufficient or even advantageous for ac-
(2) Petricoin, E. F.; Liotta, L. A. Clin. Chem. 2003, 49 (4), 533-534.
curate diagnosis (see above). Ultimately, even single markers
(3) Petricoin, E. F.; Liotta, L. A. Clin. Chem. 2003, 49 (8), 1276-1278.
have been and may be found in future that are useful for the
(4) Vitzthum, F.; Schwarz, H.; Behrens, F. Mol. Cell Proteomics 2004,
Besides the MS approach of profile signatures without
(5) Sox, J., H. C.; Blatt, M. A.; Higgins, M. C.; Marton, K. I. MedicalDecision Making. ed.; Butterworth-Heinemann: Boston, 1989.
identifying measured components, MS is widely used to detect
(6) McNeil, B. J.; Adelstein, S. J. J. Nucl. Med. 1976, 17 (6), 439-448.
distinct, identified analytes. Identifying analytes allows for the
(7) Forsman, R. Clin. Leadersh. Manag. Rev. 2000, 14 (6), 292-295.
development and implementation of reference materials for
(8) Morimoto, T.; Hayashino, Y.; Shimbo, T.; Izumi, T.; Fukui, T. Int.J. Cardiol. 2004, 96 (2), 177-181.
standardization, calibration, recovery determination, quality
(9) Zolg, J. W.; Langen, H. Mol. Cell Proteomics 2004, 3 (4), 345-
control, and quality assurance.66 For the detection of distinct
low molecular weight molecules MS has been used as a
(10) Jungblut, P. R.; Zimny-Arndt, U.; Zeindl-Eberhart, E.; Stulik, J.;
diagnostic instrument in IVD for many decades,68 e.g., for
Koupilova, K.; Pleissner, K. P.; Otto, A.; Muller, E. C.; Sokolowska- Kohler, W.; Grabher, G.; Stoffler, G. Electrophoresis 1999, 20 (10),
newborn screening to detect inborn errors of metabolism,72,73
toxicology and forensic applications,74 immunosuppressive
(11) McGregor, E.; Dunn, M. J. Hum. Mol. Genet. 2003, 12 (2), 135-
drug testing,75 drugs of abuse,76 and doping of athletes.77 In
(12) Van Eyk, J. E. Curr. Opin. Mol. Ther. 2001, 3 (6), 546-553.
these applications, appropriate internal standards are used to
(13) Granger, C. B.; Van Eyk, J. E.; Mockrin, S. C.; Anderson, N. L.
achieve appropriate test accuracy. MS analyses are even applied
Circulation 2004, 109 (14), 1697-1703.
as reference methods. For example, the determination of a
(14) Stanley, B. A.; Gundry, R. L.; Cotter, R. J.; Van Eyk, J. E. Dis.
distinct glycated peptide is used as an IFCC (International
Markers 2004, 20 (3), 167-178.
(15) Allard, L.; Lescuyer, P.; Burgess, J.; Leung, K. Y.; Ward, M.; Walter,
Federation of Clinical Chemistry) reference method for the
N.; Burkhard, P. R.; Corthals, G.; Hochstrasser, D. F.; Sanchez, J.
determination of hemoglobin A1c with inter-laboratory CVs of
C. Proteomics 2004, 4 (8), 2242-2251.
1.4% to 2.3%.25 This form of MS technology, quite distinct from
(16) Bodor, G. S. LabMed. Int. 2004, March/April, 13-14.
the use of unidentified feature patterns, is a potential alternative
(17) Adams, J. E.; Sicard, G. A.; Allen, B. T.; Bridwell, K. H.; Lenke, L.
G.; Davila-Roman, V. G.; Bodor, G. S.; Ladenson, J. H.; Jaffe, A. S.
for use in the validation and small-scale application of novel
N. Engl. J. Med. 1994, 330 (10), 670-674.
(18) Alpert, J. S.; Thygesen, K.; Antman, E.; Bassand, J. P. J. Am. Coll.Cardiol. 2000, 36 (3), 959-969. Conclusions
(19) Clinical and Laboratory Standards Institute (CLSI) formerly
National Committee for Clinical Laboratory Standards (NCCLS)
As candidate diagnostic markers begin the process of adap-
homepage: harmonized terminology database www.nccls.org.
¨ ttner, J. Eur. J. Clin. Chem. Clin. Biochem. 1995, 33, 975-1022.
tation to IVD use, much time and effort can be saved by
(21) Burtis, C. A.; Ashwood, E. R. Tietz Fundamentals of Clinical
recognizing at the outset the important criteria by which IVD
Chemistry, ed.; W. B. Saunders Company an imprint of Elsevier
tests are judged. An IVD test is not simply a better or cheaper
Science: Philadelphia, London, New York, St. Louis, Sydney,
measurement than can be obtained with the technologies used
(22) Thomas, L. Clinical Laboratory Diagnostics, ed.; TH-Books
for discovery: it is also a measurement that has a fairly definite
Verlagsgesellschaft: Frankfurt, 1998.
meaning in the context of the patient’s overall clinical picture
(23) International Standards Organization (ISO), Terms and Definitions
and especially treatment. In many ways, new markers should
Used in Connection with Reference Materials (ISO Guide 30 (E/F)), 2 ed.; ISO: Geneva, 1992.
be considered separately from new measurement technolo-
(24) Bandy, M. IVD Technol. 2005, March, 24-9.
gies: a new marker could be brought into use much more
(25) Jeppsson, J. O.; Kobold, U.; Barr, J.; Finke, A.; Hoelzel, W.;
rapidly as a test on an existing, validated platform (e.g.,
Hoshino, T.; Miedema, K.; Mosca, A.; Mauri, P.; Paroni, R.;
immunoassay) than on a novel technology platform whose
Thienpont, L.; Umemoto, M.; Weykamp, C. Clin. Chem. Lab. Med. 2002, 40 (1), 78-89.
acceptance is naturally slowed by economic (new clinical lab
(26) Fraser, C. G.; Petersen, P. H. Clin. Chem. 1999, 45 (3), 321-323.
investment), regulatory, and other factors. This fact argues
(27) Apple, F. S.; Wu, A. H.; Jaffe, A. S. Am. Heart J. 2002, 144 (6),
strongly that candidate IVD markers should be identified and
(28) Klee, G. G. Clin. Chem. 1993, 39 (7), 1514-1518.
fully characterized as part of the discovery process, and should
(29) Lammers, M.; Gentzer, W.; Boni, P.; Fitzner, R.; Guarmeur-Jardel,
then transition to a technology base better suited to adoption
C.; Ledue, T. B. Multicentric performance evaluation of the BN
in the clinical laboratory. The opportunity to combine immu-
ProSpec plasma protein analyzer system.; AACC Congress, Chicago
noassay technologies and MS, which would be applied as a
(30) Holland, N. T.; Smith, M. T.; Eskenazi, B.; Bastaki, M. Mutat. Res.
sophisticated detector that can unambiguously identify ligands
2003, 543 (3), 217-234.
appears to be attractive. On the other hand, the costs associated
(31) Haab, B. B.; Geierstanger, B. H.; Michailidis, G.; Vitzthum, F.;
with the application of MS as a detection unit in comparison
Forrester, S.; Okon, R.; Saviranta, P.; Brinker, A.; Sorette, M.;Perlee, L.; Suresh, S.; Drwal, G.; Adkins, J. N.; Beer, I.; Omenn, G.
to other detection technologies are currently considered pro-
Proteomics 2005, in press.
hibitive and most MS instrumentation falls far short of the
(32) Rai, A. J.; Gelfand, C. A.; Haywood, B. C.; Warunek, D. D.; Skobe,
robustness, automation, and user-friendliness required for
C.; Schuchard, M. D.; Mehigh, R. J.; Cockrill, S. L.; Scott, G. B. I.;
routine laboratory operation. Nevertheless, while immunoas-
Tammen, H.; Schulz-Knappe, P.; Speicher, D. W.; Vitzthum, F.; Habb, B. B.; Siest, G.; Chan, D. W. Proteomics 2005, in press.
says dominate IVD protein measurements presently, it appears
(33) Biobank, T. U. Sample Handling and Storage Subgroup Protocol
that the challenges of multiplexing such tests (e.g., on arrays)
and Recommendations, ed.; UK Biobank: Manchester, 2004. Journal of Proteome Research • Vol. 4, No. 4, 2005 In Vitro Diagnostic Requirements Impacting Proteomics
(34) Vitzthum, F. Entwicklung und Untersuchung Automatisierungs-
(54) Tillet, W. S.; Francis, T. J. Exp. Med. 1930, 52, 561-571. gerechter Physikalisch-Mechanischer Desintegrationsverfahren fu
(55) Ridker, P. M.; Buring, J. E.; Shih, J.; Matias, M.; Hennekens, C. H. ¨ tzte, Humanmedizinische Infektionsdi-Circulation 1998, 98 (8), 731-733. agnostik [Development and Evaluation of Automated Physical and
(56) Feinstein, A. R. Clinical Epidemiology: The Architecture of ClinicalMechanical Disintegration Technologies for Nucleic Acid BasedResearch, ed.; WB Sauenders Company: Philadelphia, 1985; p
Diagnosis of Infectious Diseases], ed.; Fraunhofer IRB Verlag:
(57) Feinstein, A. R. Clinical Biostatistics, ed.; The CV Mosby Com-
(35) Landi, M. T.; Caporaso, N. IARC Sci. Publ. 1997, 142, 223-236.
(36) Glover Leonard & Redshaw Management Consultancy: Labora-
(58) Lescuyer, P.; Allard, L.; Zimmermann-Ivol, C. G.; Burgess, J. A.;
tory workload segmentation audit of medium to high specimen
Hughes-Frutiger, S.; Burkhard, P. R.; Sanchez, J. C.; Hochstrasser,
throughput laboratory locations in Europe; Glover Leonard &
D. F. Proteomics 2004, 4 (8), 2234-2241.
Redshaw: Brussels, Bronxville, 1997; p 71.
(59) Zimmermann-Ivol, C. G.; Burkhard, P. R.; Le Floch-Rohr, J.; Allard,
(37) Anderson, N. L.; Anderson, N. G. Mol. Cell Proteomics 2002, 1
L.; Hochstrasser, D. F.; Sanchez, J. C. Mol. Cell Proteomics 2004,
(38) Winsten, S.; Gordesky, S. E., Transportation of specimens. In
(60) White, N.; Zhang, Z.; Chan, D. W. Clin. Chem. Lab. Med. 2005, Selected methods of clinical chemistry, ed.; Faulkner, W. R.;
AACC: Washington, DC, 1982; Vol. 9, p 11-15.
(61) Petricoin, E.; Wulfkuhle, J. D.; Espina, V.; Liotta, L. A. J. Proteome
(39) Aziz, N.; Nishanian, P.; Mitsuyasu, R.; Detels, R.; Fahey, J. L. Clin.Res. 2004, 3, 209-217. Diagn. Lab. Immunol. 1999, 6 (1), 89-95.
(62) Stoll, D.; Templin, M. F.; Schrenk, M.; Traub, P. C.; Vohringer, C.
(40) National Committee for Clinical Laboratory Standards (NCCLS),
F.; Joos, T. O. Front Biosci. 2002, 7, c13-32. Blood collection on filter paper for neonatal screening programs:
¨ ller, H.-J.; Vieth, F.; Risse, B. approved standard LA4-A3. 3 ed.; NCCLS: Wayne, PA, 1997. Laborwelt 2004, 4, 38-39.
(41) National Committee for Clinical Laboratory Standards (NCCLS),
(64) Aivado, M.; Spentzos, D.; Alterovitz, G.; Otu, H. H.; Grall, F.;
Procedures for collection of skin puncture blood specimens:
Giagounidis, A. A. N.; Wells, M.; Cho, J.-Y.; Germing, U.; Czibere,
approved standard H4-A4. 4 ed.; NCCLS: Wayne, PA, 2000.
A.; Prall, W. C.; Porter, C.; Ramoni, M. F.; Libermann, T. A. Clin.
(42) National Committee for Clinical Laboratory Standards (NCCLS),
Chem. Lab. Med. 2005, 43 (2), 133-140. Evacuated tubes and additives for blood specimen collection:
(65) Petricoin, E. F.; Ardekani, A. M.; Hitt, B. A.; Levine, P. J.; al., e. approved standard H1-A4. 4 ed.; NCCLS: Wayne, Pa, 1996. The Lancet 2002, 359, 572-577.
(43) National Committee for Clinical Laboratory Standards (NCCLS),
(66) Hortin, G. L. Clin. Chem. 2005, 51, 3-5. Procedures for collection of diagnostic bllod specimens by veni-
(67) Diamandis, E. P. Clin. Chem. 2003, 49 (8), 1272-1275. puncture: approved standard H3-A4. 4 ed.; NCCLS: Wayne, Pa,
(68) Diamandis, E. P. Mol. Cell Proteomics 2004, 3 (4), 367-378.
(69) Baggerly, K. A.; Morris, J. S.; Coombes, K. R. Bioinformatics 2004,
(44) National Committee for Clinical Laboratory Standards (NCCLS),
Procedures for the handling and transport of domestic diagnostic
(70) Coombes, K. R. Clin. Chem. 2005, 51, 1-2. specimens and etiologic agents: approved standard H5-A3. 3 ed.;
(71) Sorace, J. M.; Zhan, M. BMC Bioinformatics 2004, 4 (24), 1-13.
(72) Venditti, L. N.; Venditti, C. P.; Berry, G. T.; Kaplan, P. B.; Kaye, E.
(45) National Committee for Clinical Laboratory Standards (NCCLS),
M.; Glick, H.; Stanley, C. A. Pediatrics 2003, 112 (5), 1005-1015. Routine urinalysis and collection, transportation, and preservation
(73) Chace, D. H.; Kalas, T. A.; Naylor, E. W. Clin. Chem. 2003, 49 of urine specimens: approved guideline GP16-A. ed.; NCCLS:
(74) Dooley, K. C. Clin. Biochem 2003, 36 (6), 471-481.
(46) Lusted, L. B. Science 1971, 171 (977), 1217-9.
(75) Streit, F.; Armstrong, V. W.; Oellerich, M. Clin. Chem. 2002, 48 (6
(47) Henderson, R. Ann. Clin. Biochem. 1993, 30, 521-39.
(48) Obuchowski, N. A.; Lieber, M. L.; Wians, F. H., Jr. Clin. Chem.
(76) Niedbala, S.; Kardos, K.; Salamone, S.; Fritch, D.; Bronsgeest, M.;
2004, 50 (7), 1118-25.
Cone, E. J. J. Anal. Toxicol. 2004, 28 (7), 546-552.
(49) Zhou, X.-H.; Obuchowski, N. A.; McClish, D. K. Statistical Methods
(77) Frison, G.; Tedeschi, L.; Favretto, D.; Reheman, A.; Ferrara, S. D. in Diagnostic Medicine, ed.; John Wiley & Sons: New York, 2002. Rapid Commun. Mass Spectrom. 2005, 19 (7), 919-927.
¨ ttner, J. Beurteilung Klinisch-Chemischer Analy-
(78) Weber, T.; Auer, J.; Eber, B. Curr. Pharm. Des. 2005, 11 (4), 511-
senergebnisse. In Lehrbuch der Klinischen Chemie und Patho-biochemie, 3 ed.; Greiling, H., Gressner, A. M., Eds.; Schattauer:
(79) Hofmann, W.; Regenbogen, C.; Edel, H.; Guder, W. G. Kidney Int.
Stuttgart, New York, 1995; p 73-114. Suppl. 1994, 47, 111-114.
(51) Griner, P. F.; Mayewski, R. J.; Mushlin, A. I.; Greenland, P. Ann.
(80) Bowker, S. L.; Mitchell, C. G.; Majumdar, S. R.; Toth, E. L.;
Intern. Med. 1981, 94 (4 Pt 2), 557-592.
Johnson, J. A. CMAJ. 2004, 171 (1), 39-43.
(52) Voss, R.; Cullen, P.; Schulte, H.; Assmann, G. Int. J. Epidemiol.
(81) Wick, H. D. Schweiz Rundsch Med. Prax 1999, 88 (42), 1711- 2002, 31 (6), 1253-1264.
(53) Assmann, G.; Cullen, P.; Schulte, H. Circulation 2002, 105 (3), Journal of Proteome Research • Vol. 4, No. 4, 2005
Thurs H5 v2_Layout 1 17/08/2010 16:00 Page 52Reprinted in IVIS with the permission of BEVA Thursday 9th September 2010 Neurology Sponsored by University of Liverpool 16.20–16.40 ‘How to’ interpret equine cervical radiographs and other imaging modalities Richard J. Piercy Royal Veterinary College, London, UK. Plain radiography of the cervical vertebrae can be used to
Obra de Teatro Infantil en 2 Actos De: Madeleine Porr Colaboraron: Jesús Fernández Neda Avelino Couceiro Eladio Reyes Arias Katya Pineiro Contiene: EL RAP DEL PAN ALEGRE Autor: Hernán de la Caridad Herrera Ruiz 10 de Octubre de 2001 Reparto por orden de aparición: Indias e Indios . Marqués de Canete . Soldado 1. Soldado 2. Soldad
 Proteomics: From Basic Research to Diagnostic Application.
Proteomics: From Basic Research to Diagnostic Application. In Vitro Diagnostic Requirements Impacting Proteomics
In Vitro Diagnostic Requirements Impacting Proteomics Vitzthum et al.
Vitzthum et al.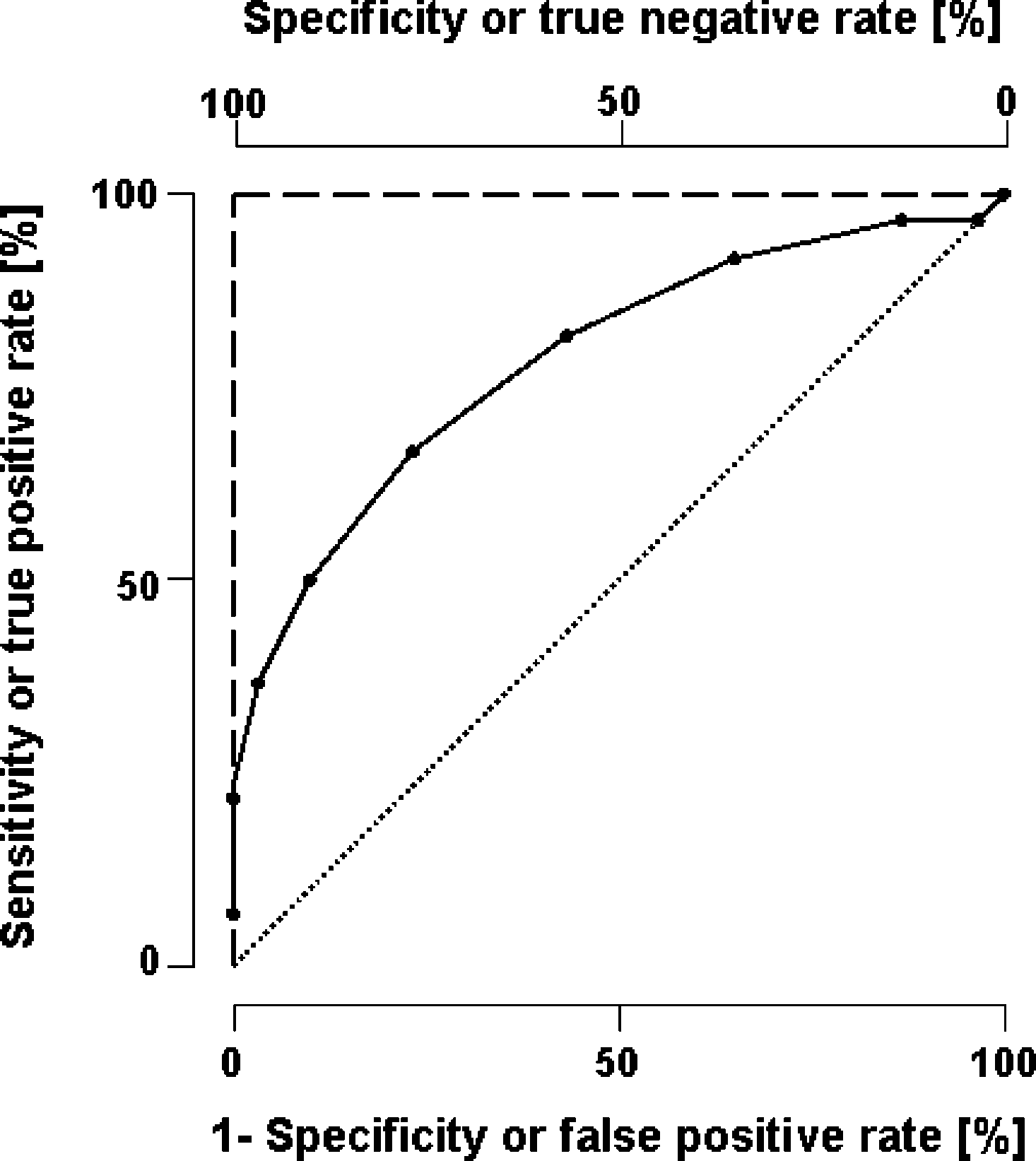 In Vitro Diagnostic Requirements Impacting Proteomics
In Vitro Diagnostic Requirements Impacting Proteomics