Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
Copd and spirometry.pdf
ORIGINAL ARTICLES CLINICAL GUIDELINE Guideline for Office Spirometry in Adults, 2004 South African Thoracic Society Standards of Spirometry Committee: E M van Schalkwyk, C Schultz, J R Joubert, N W White Objective. To provide clinical guidelines for office spirometry
Conclusions. The indications for spirometry must be specific
and clear. Spirometry equipment must meet internationally
Options. More stringent guidelines are required for diagnostic
accepted performance standards and carry proof of
validation. Equipment must be regularly calibrated and
Outcomes. To minimise variations in standard practice and
maintained. Individuals performing spirometry must be
improve the quality and usefulness of spirometry in the
adequately trained and demonstrate a high level of
competence. Subject preparation, testing and quality control
Evidence. Recommendations are based on key international
of results must be carried out according to published
publications as well as research publications regarding
guidelines. Finally, test results must be interpreted according
reference values for South Africans.
to current diagnostic guidelines, taking into account the
Benefits, harm and costs. The medical, social and economic
purpose of the test, appropriateness of reference values and
benefits and costs of standardisation of office spirometry in
South Africa were considered in the recommendations. S Afr Med J 2004; 94: 576-587. Validation. The document has been reviewed and endorsed bythe South African Thoracic Society. 1. Abbreviations
guidelines for the standardisation of spirometry.2-4 Morerecently, selective South African reference standards have
ATPS = ambient temperature, ambient pressure, saturated with
become available for the normal range of forced vital capacity
water vapour; ATS = American Thoracic Society; BTPS = body
(FVC) and forced expiratory volume in 1 second (FEV1). 5-10 This
temperature, ambient pressure, saturated with water vapour;
statement is prompted by increased utilisation of office
ECSC = European Community for Steel and Coal; ERS =
spirometry in South Africa and a perceived need for simplified
European Respiratory Society; FEV1 = forced expiratory
guidelines for use at primary contact level, i.e. in the clinic or
volume in 1 second; FVC = forced vital capacity; LLN = lower
practice. Diagnostic and research lung function laboratories
limit of normal; PEF = peak expiratory flow; RSD = residual
will require more comprehensive guidelines than proposed in
standard deviation; SATS = South African Thoracic Society;
TLC = total lung capacity; VC = vital capacity. 3. Definitions 2. Introduction Spirometry. Spirometry is one of a number of tests to evaluate
Spirometry is an essential part of a complete respiratory
respiratory function. The basic spirometric procedure involves
evaluation, but inadequate standards and variations in
the measurement of gas volume and rate of airflow during a
standard operating procedures exist that reduce its clinical
maximal, forced expiration. The mechanical properties of the
usefulness.1 Good quality spirometry necessitates a competent
airways, lung, pleura, chest wall and respiratory muscles all
operator, accurate and reliable equipment and a co-operative
patient. Furthermore, it involves a series of standard
Spirometer. Spirometers operate on one of two principles:
procedures and quality control checks to produce technically
• Volume-type spirometers determine volume directly and
satisfactory results. Finally, the results take reference standards
have the advantages of low cost and ease of operation.
into account and are interpreted with consideration of the
However, data processing and storage capacity may be
limited, unless the spirometer contains a microprocessor.
Various authorities have published comprehensive
• Flow-type spirometers make use of a flow-sensor
(pneumotach) to derive volumes. They are computerised,
Corresponding author: Dr E M van Schalkwyk, Department of Medicine,
provide quick reference values, produce flow-volume loops
Stellenbosch University, PO Box 19063, Tygerberg, 7505, e-mail emvs@sun.ac.za
enabling instant pattern recognition and can usually store
July 2004, Vol. 94, No. 7 SAMJ ORIGINAL ARTICLES
large data sets. On the other hand, they require greater
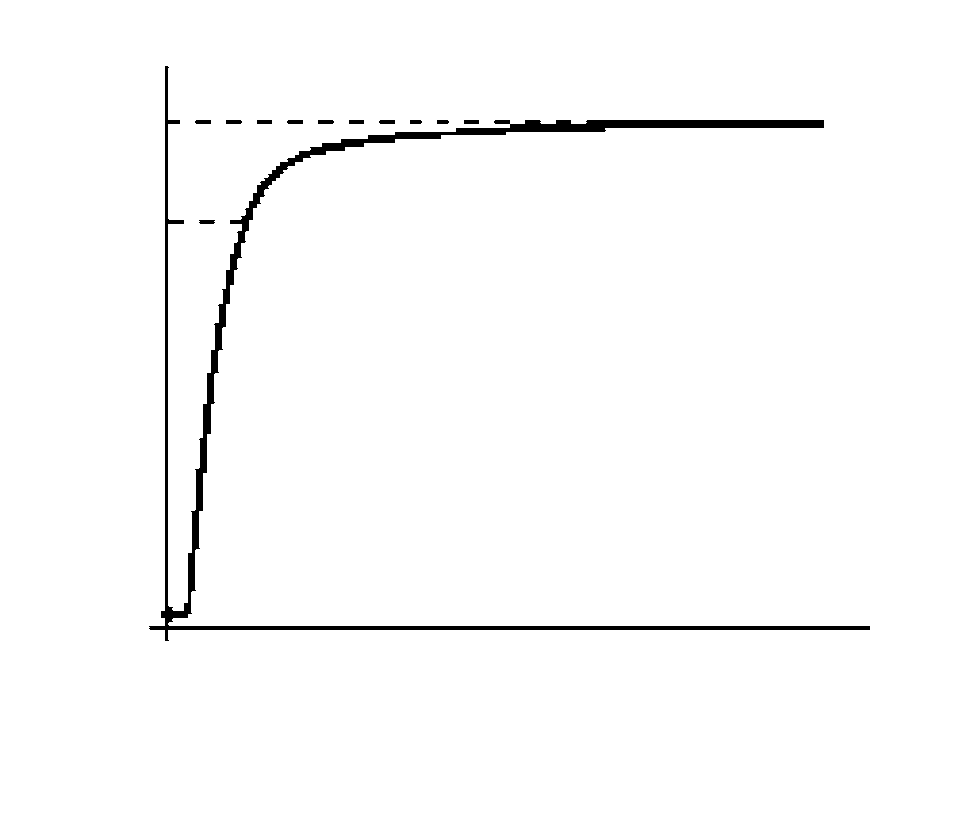
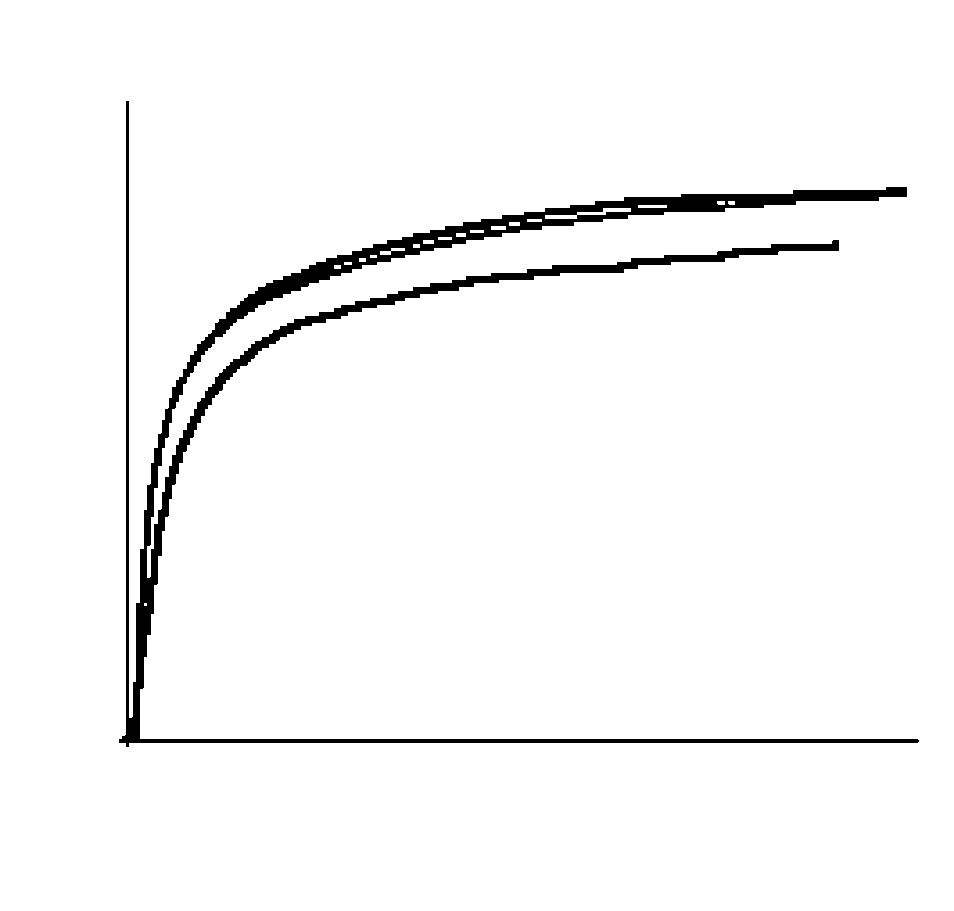
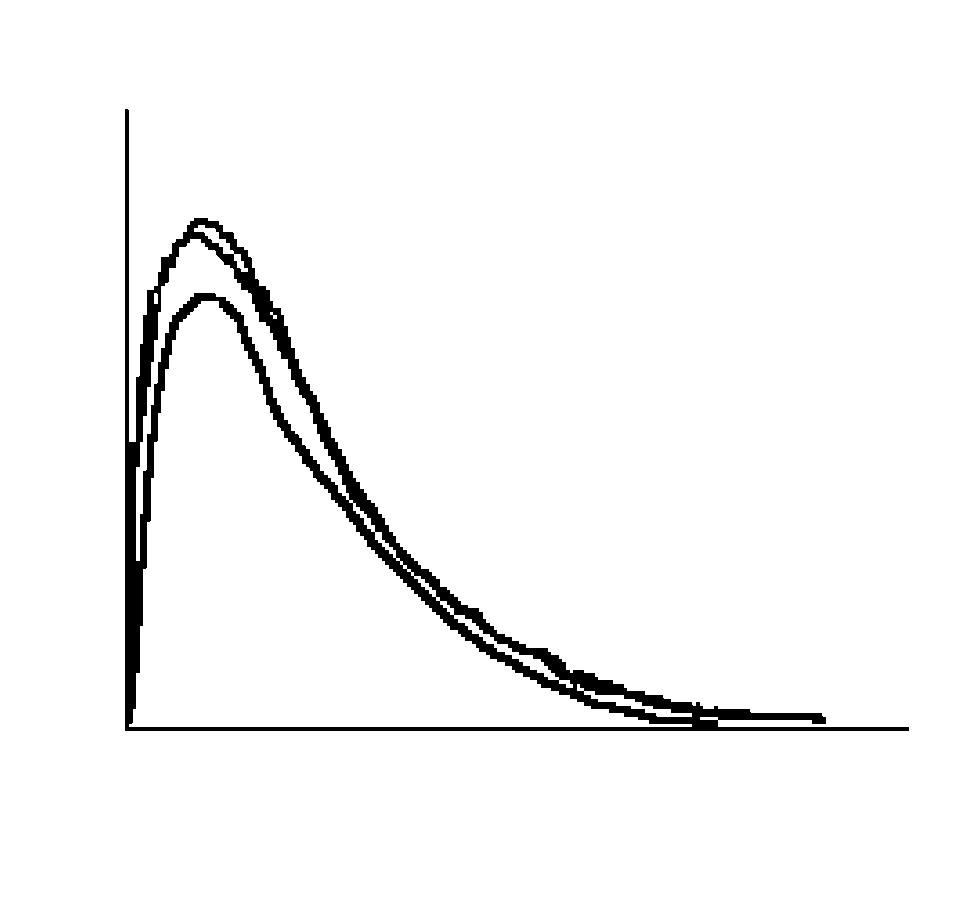
time curves (Fig. 1a) and flow-type devices generate flow-
expertise to operate, calibrate and maintain.
volume curves (Fig. 1b). Newer flow-type spirometers can
Spirogram. Spirograms are the graphic displays produced by
spirometers. In addition to graphs, they provide the measured
Measurements. Depending on type and level of
values (observed), the reference values (predicted) and the
sophistication, spirometers can produce a range of measurements
measured values expressed as a percentage of the reference
that may assist in the clinical interpretation of results:
values (% predicted). Volume-type devices generate volume-
• Vital capacity (VC): VC is the total volume of gas inhaled from
the position of maximal expiration or exhaled from theposition of maximal inspiration. It is measured with a
relaxed/slow breathing manoeuvre either during inspiration
or expiration. VC is expressed in litres (BTPS). BTPS refers toa standardised volume at normal body temperature (37°C) atambient pressure, saturated with water vapour.
• Forced vital capacity (FVC): FVC is the maximum volume of
gas exhaled from the position of maximal inspiration bymeans of a rapid, maximally forced expiratory effort,
• Forced expiratory volume in 1 second (FEV1): FEV1 is the volume
of gas exhaled during the first second of the FVC manoeuvre,expressed in litres (BTPS).
• FEV1/FVC%: FEV1/FVC% is observed FEV1 expressed as per
cent of observed FVC (FEV1/FVC × 100).
• Peak expiratory flow (PEF): PEF is the maximum flow
generated with a FVC manoeuvre, expressed in litres per
second (BTPS). Measurements of FVC, FEV1 and FEV1/FVC% are the
minimum required for diagnostic interpretation of results. VC
measurements are useful for evaluating dynamic collapse of
small airways as found in emphysema. Calibration. Calibration is the process whereby the accuracy
(truthfulness) and precision (repeatability) of a device such as aspirometer are tested and corrected using a gold standard such
as a calibration syringe with a standard volume. Validation. Validation is the process of establishing and
certifying the accuracy and precision of a device. Operator. The term operator refers to the person performing 4. Indications for spirometry
Specific and clear indications for spirometry are helpful in theinterpretation of results. The most frequent clinical indications
for spirometry are listed below:• To confirm a diagnosis in:
• Individuals with suspected obstructive or
• To grade respiratory impairment in.
• Medico-legal cases (e.g. assurance or disability)
• Individuals on treatment action plans (e.g. COPD)
• Individuals for lung resection, and individuals for
thoracotomy or upper-abdominal surgery if they
Fig. 1. (a) Volume-time, and (b) flow-volume curves. In the flow-typespirometer FEV1 is a derived value. It can only be read from the flow-volume graph if a 1-second timer is displayed.
July 2004, Vol. 94, No. 7 SAMJ ORIGINAL ARTICLES
• To monitor changes in lung function in:
volume or flow) and linearity (consistency) of the entire system
• Individuals with chronic respiratory diseases — to
from the measuring components to the recording and display
evaluate responses to treatment and disease
components. The American Thoracic Society (ATS) has
published minimal performance criteria for diagnostic and
• Workers regularly exposed to substances known to cause
monitoring spirometers and guidelines for validating
equipment using waveform-generated calibration syringes.2
Selective ATS recommendations for diagnostic spirometers are
provided in Tables I and II. Table II provides standards for
• Individuals with persistent respiratory symptoms,
graph output. Manufacturers should follow these guidelines to
including shortness of breath (dyspnoea), chest
ensure that spirometers provide accurate data that are
tightness, wheezing, coughing, sputum production and
comparable between different settings and over time.
Commercially available devices for monitoring of FEV1 and PEF
• New employees with potential for exposure to
have disadvantages for office spirometry because they may be
substances known to cause respiratory diseases —
less accurate, usually cannot be calibrated to ensure their
performance, and graphical displays may be absent or
• Workers with significant exposure to substances
inadequate for evaluation of test quality.
known to cause respiratory diseases.
Spirometry is frequently applied in the occupational
• The BTPS-correction facility that meets ATS standards: The
environment for surveillance purposes. Its sensitivity and
volume of exhaled gas is measured outside the body at
specificity for detecting early disease varies and a screening
ambient conditions, designated ATPS (ambient temperature,
programme should be tapered to the specific needs of the
ambient pressure, saturated with water vapour). These gas
workplace. For example, early changes of COPD or asbestosis
measurements are corrected to reflect conditions inside the
are detectable with spirometry, whereas early changes of
lung (BTPS). Without this facility, mathematical correction
silicosis are better detected with chest radiography. For
occupational asthma, because of its varying nature, arespiratory symptoms questionnaire is frequently combinedwith spirometry in screening or surveillance programmes. Table II. Minimum scale factors for spirograms* 5. Specifications for spirometers 5.1 Proof of validation
Spirometers may lack accuracy and precision. Prospective
*For the flow-volume curve exhaled flow is plotted upwards and exhaled volumetowards the right in a 2:1 ratio.
purchasers of equipment should seek its proof of validation. Accuracy depends on the resolution (minimal detectable
Table I. Selective minimum volume and flow criteria for diagnostic spirometers
July 2004, Vol. 94, No. 7 SAMJ ORIGINAL ARTICLES
• Facility to generate real-time spirograms — to enhance
occluded. Any volume change greater than 10 ml after 1 minute
indicates a leak. Faults are corrected and calibration repeated.
• Stated source(s) of reference values and facility to select or
5. Remaining problems are logged and referred to the
• Computer-driven technical quality indicators that meet ATS
The use of biological standards such as, for example, the
standards (computer automatically evaluates test quality
operator for daily volume calibration (biological calibration)
based on pre-programmed criteria and gives prompts).
cannot replace the use of a calibration syringe. Lung function
• Printing facility for record-keeping purposes.
testing involves a ‘system’ consisting of three main
• Adequate facility to save large numbers of tests and test
components: spirometer, operator and test subject. Each of
quality indicators where needed, for example, for
these can be a source of variation in measurements and syringe
calibration is required in order to isolate the device. Biological
• Availability of after-sales service.
standards are useful for testing software irregularities such as,
In addition to mechanical validation, spirometers can also
for example, inconsistencies in the calculation of predicted
be tested in real-life situations involving human subjects.12
values. Also, when they are used in conjunction with a
SATS recommend that independent professional advice
physical standard (calibration syringe), biological standards are
from a registered pulmonology training laboratory or the
useful to test the proficiency of operators.
Spirometry Training and Certification Committee of the South
In addition to daily volume calibration, spirometers must be
African Thoracic Society (SATS) be obtained before a new
maintained routinely according to the manufacturer’s
specifications. This includes the cleaning of pneumotachs atleast once a week (more frequently if there is visible
5.2 Calibration
condensation), as they are particularly sensitive to moisture
All diagnostic spirometers must be volume-calibrated at least
and secretions. Other components of the spirometer, for
daily using a calibrated syringe with a volume of at least 3 l to
example the time clock, must also be calibrated from time to
ensure that they remain accurate during use. During industrial
time. For these and other maintenance functions the
surveys in which a large number of subject manoeuvres are
manufacturer must routinely check spirometers at least 6 - 12-
performed, calibration must be checked each morning and at
least twice during the day. In circumstances where thetemperature may change markedly over the day, for example
6. Responsibilities of operators
in field surveys, more frequent temperature corrections arenecessary.
Calibration involves the following steps:
6.1 Skills
1. The spirometer is switched to calibration mode (to
Operators must have an understanding of the principles
prevent BTPS-correction because room air is injected). Room
underlying the measurement and equipment operation. They
temperature and barometric pressure readings are entered. In
must also be able to ensure optimal subject co-operation,
the absence of a barometer, barometric pressure readings can
provide acceptable, reproducible results and recognise common
be obtained from the local airport or weather bureau.
abnormalities. Training of pulmonary medical technologists
2. Calibration syringe size is specified. A 3 l syringe is
includes this competency and competency to perform
recommended. Currently, the use of 2 l and 1 l syringes is not
advanced lung function tests and laboratory quality assurance.
The SATS is in the process of developing a curriculum, training
3. The calibration syringe is connected to the spirometer and
materials and a means of certification of proficiency in
the maximum volume of air injected. Flow-type spirometers
performing spirometry for people other than pulmonary
are calibrated by injection of the maximum volume from the
syringe at least three times, each time at a different speed, tocover a range of flow rates. Calibration is complete when the
6.2 Quality assurance
recorded volumes are within 3% or 50 ml, whichever is the
A quality assurance programme is critical to ensure a well-
greater, for each flow rate tested. In the event of in-line
functioning spirometry laboratory.13 This may be difficult to
(antimicrobial) filters being used, calibration should be done
attain in a routine clinical practice. At a minimum, a
with a filter installed. The quality of the filter must be such
calibration and maintenance log as well as electronic or hard
that the spirometry system still meets ATS standards.
copies of whole spirograms must be kept so that accuracy and
4. Volume-type spirometers are checked for air leaks if the
precision of past tests can be verified. Additionally, standard
measured volume remains outside the acceptable range. A leak
operating procedures should be documented and kept for
can be detected by applying a slight constant positive pressure
with the calibration syringe while the spirometer outlet is
July 2004, Vol. 94, No. 7 SAMJ ORIGINAL ARTICLES 6.3 Infection control
the day will allow for overnight decontamination of
Various components of the spirometry system, including
equipment. (Note: indications for spirometry in known
mouthpieces, nose clips, pneumotachs, valves and tubing, are
potential vehicles for transmission of infection to subjects and
For decontamination/sterilisation procedures, consult the
staff. Transmission of upper respiratory tract infections, enteric
user manual or contact the infection control unit or lung
infections and blood-borne infections such as hepatitis and
function laboratory at an academic hospital near you.
HIV, can potentially occur through direct contact when testsubjects have open sores in the mouth, bleeding gums or
7. Preparation of subjects
haemoptysis. Tuberculosis and viral and nosocomial infectionscan also occur, indirectly, through inhalation of aerosol droplets
7.1 Exclusion criteria
from the spirometer or surroundings. The type of testmanoeuvre determines whether inhalation from the spirometer
The main exclusion criterion for spirometry in routine clinical
takes place. This has a major influence on the extent of
practice is current respiratory infections in individuals for
infection control needed. An expiratory manoeuvre without
impairment/disability assessment. Respiratory infections can
inhalation from the spirometer reduces the potential for cross-
cause temporary lung function impairment and spirometry, if
infection dramatically and is the method of choice for mass
required, should be done only once infections, including
Infection control recommendations for expiratory 7.2 Personal information manoeuvres without inhalation from the spirometer: • Spirometry should be performed in a well-lit and ventilated
The following information is required for reference purposes
(section 9.2) and must be entered into the programme: weight
• Hands must be washed immediately after direct handling of
and standing height, age, sex and race. For height and weight
mouthpieces or other potentially contaminated spirometer
measurements the subject should be barefoot and wear only
parts, and between subjects, to avoid operator exposure and
light clothing. It is also useful for interpretation purposes to
cross-contamination. Gloves should be worn for personal
record the time of last bronchodilator use and smoking status.
protection if there are open cuts or sores on the operator’shands. 7.3 Positioning and preparation
• A clean disposable mouthpiece or a disinfected re-usable
The subject must be made to feel comfortable. Shelter him/her
mouthpiece must be used for every test subject. Any other
from other subjects to minimise inhibitions or distractions.
spirometer part coming into direct contact with mucosal
Loosen tight clothing. Leave well-fitting dentures in, but
surfaces must be decontaminated/sterilised.
remove loose-fitting ones. Test the subject sitting upright on a
• Spirometers must be cleaned regularly according to the
firm chair with his/her chin slightly elevated and neck slightly
manufacturer’s recommendations and the frequency of tests
extended. This posture should be maintained during the
done. Any part with visible condensation from expired air
forced expiration. Discourage excessive bending at the waist.
must also be decontaminated before re-use.
Use of a nose clip is strongly recommended. Instruct the
Additional infection control recommendations for
patient when to insert the mouthpiece, for example, at the end
manoeuvres involving inhalation from the spirometer system
of maximal inspiration. Ensure that the subject does not bite
or part of the system:
the mouthpiece too hard, that the lips are sealed tightly around
• In-line filters must be used and replaced after each subject,
it, and that the tongue does not obstruct the mouthpiece in any
• Involved parts of the system (i.e. spirometer, breathing
Ensure maximum subject co-operation. Submaximal efforts
tubes and resistive element of the pneumotach) must be
are a frequent cause of abnormal results. Explain techniques in
decontaminated/sterilised/flushed after each subject.
simple terms and demonstrate them to the patient. For
(Note: re-calibration is necessary every time a system has
example, explain that: ‘I am going to have you blow into the
machine to see how big your lungs are and how fast the air
Special precautions for patients with haemoptysis or
comes out. It does not hurt but requires your co-operation and
known transmissible infections such as tuberculosis:
lots of effort.’ Explain and demonstrate the use of a nose clip
• In-line filters must be used routinely (even if expiratory
and mouthpiece. Remind the patient of a few key points. ‘Be
manoeuvres are performed exclusively) with sterilisation of
sure to take as deep a breath as possible, blast out hard and do
not stop blowing until I tell you to do so.’ Give feedback about
• Equipment must be decontaminated/sterilised/flushed
the performance, encourage and describe what improvements
completely after each case. Testing such cases at the end of
July 2004, Vol. 94, No. 7 SAMJ ORIGINAL ARTICLES 8. Execution of tests
be expelled from the lungs), lasting until the volume-timecurve has clearly reached a plateau or the flow-volume
8.1 Test manoeuvres
curve has progressively returned to zero flow.
Test manoeuvres are determined in part by the setting and
All technically unsatisfactory trials must be rejected.
level of sophistication of the spirometer:
Common patterns are illustrated in Figs. 2 - 4.
• Expiratory-only method. For reasons of ease, cost and
infection control this method is recommended for mass
8.2.2 Reproducibility
screening. It consists of a FVC test with or without a slow
Suboptimal effort by the test subject is a frequent cause of
VC test. For the FVC test, the test subject is required to
diminished lung function results. Ensuring reproducibility of
inhale maximally before inserting the mouthpiece and
test results is a way of verifying that the test subject co-
starting the test. Expiration must be rapid, forceful and
operates fully and provides maximal effort. Reproducibility is
complete, lasting at least 6 seconds. If significant
defined as two curves in which the difference in FVC and
obstruction is demonstrated, proceed with a slow VC test.
FEV1, respectively, do not exceed 0.2 l. Reproducibility is
The slow VC test is preceded by a maximal inspiration, the
usually evident from the spirogram at a glance (Fig. 5). Testing
mouthpiece is inserted and the patient then breathes out ina relaxed fashion and for as long as possible. Allow for upto 15 seconds. Only the VC is recorded. The rationale forperforming a slow VC test is as follows: the slow VC providesadditional information on the characteristics of the obstructivedefect. A reduction in FVC compared with slow VC suggestsdynamic collapse of unsupported airways during forced expirationleading to air trapping. This pattern is typically seen in
• Inspiratory-expiratory method. With this method both
inspiration and expiration are recorded to generate a flow-volume curve on a flow-type spirometer. Typically, after
insertion of the mouthpiece, a period of quiet breathing isfollowed by a complete expiration, a rapid, forceful and
complete inspiration and finally, a rapid, forceful andcomplete expiration. Some programmes prompt for an
expiratory manoeuvre followed by an inspiratory
manoeuvre. However, the first method is recommended,because this will reveal air trapping as described in the
previous section. Reduced FVC compared with forced,inspiratory VC is suggestive of air trapping. 8.2 Test quality
The final step in ensuring data quality is the evaluation ofspirograms for acceptability and reproducibility.8.2.1 Acceptability A technically acceptable FVC trial (Fig. 1) must exhibit the
following qualities:• A ‘crisp’, unhesitating start.
• PEF of the flow-volume curve achieved within the first 25%
of the volume expired from maximum inspiration. (Most
individuals are able to produce PEF within the first 15% of
• A continuous smooth exhalation without artefacts caused
by coughing, variable effort, second inhalations or leaks
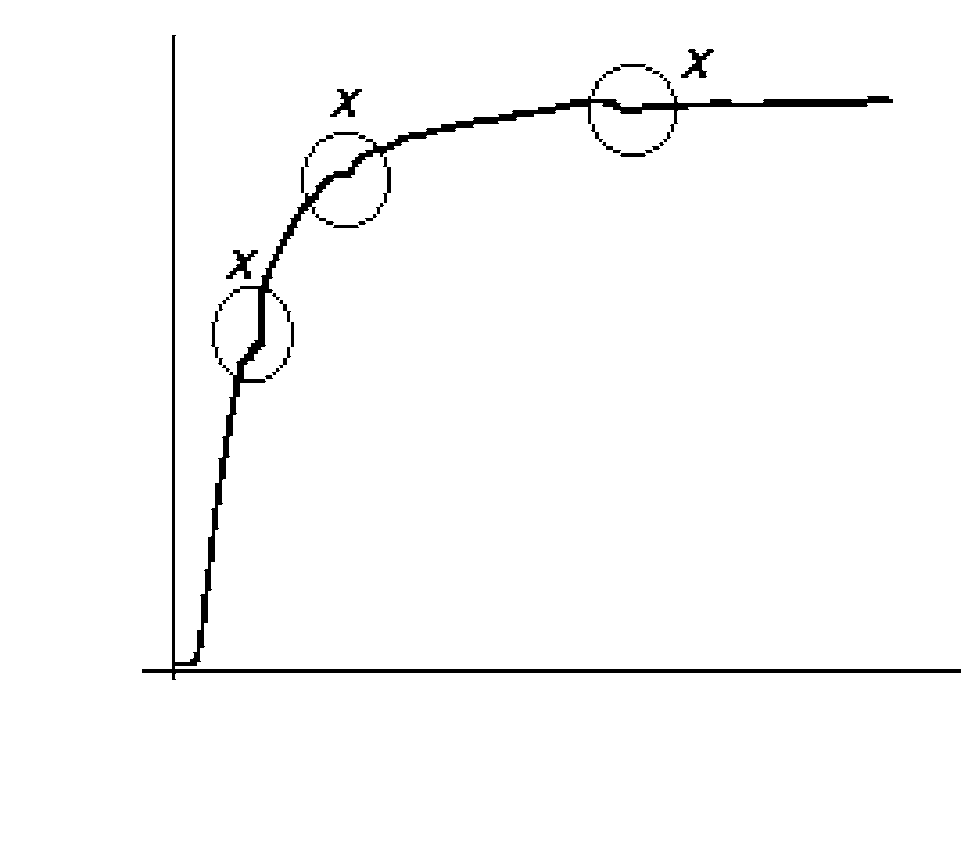
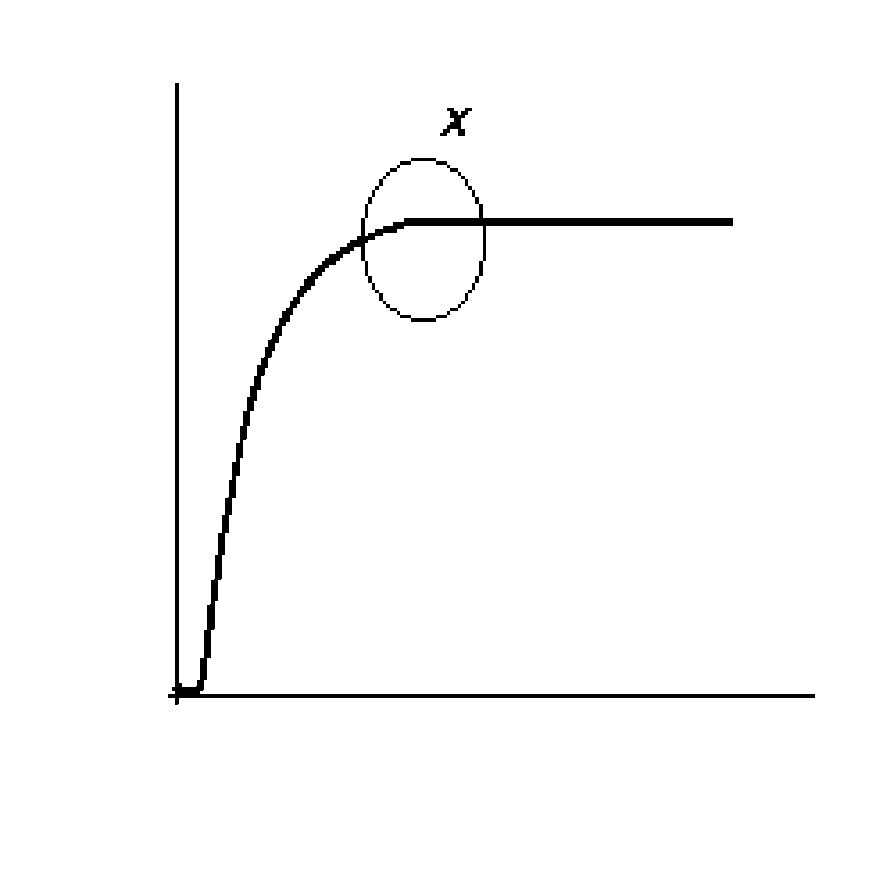
Fig. 2. (a) Volume-time, and (b) flow-volume curves exhibiting
• A complete exhalation (to the point where no more air can
cough artefacts (X) that can influence observed FVC and FEV1.Volume-time graphs are better for evaluating end-of-test quality.
July 2004, Vol. 94, No. 7 SAMJ ORIGINAL ARTICLES
must continue until a minimum of three technically acceptableFVC trials have been obtained, at least two of which are
reproducible. However, no more than eight trials should beperformed during a single session, because fatigue induced by
repeated FVC trials can lead to reduced results. Subjects withasthma sometimes demonstrate spirometry-inducedbronchoconstriction leading to a progressive reduction in lung
function with successive trials. This finding will be of interestto the clinician and all acceptable curves should be kept for
reporting. Failure to obtain reproducibility after eight trialsmust be documented, but selection of the best curve mayproceed.
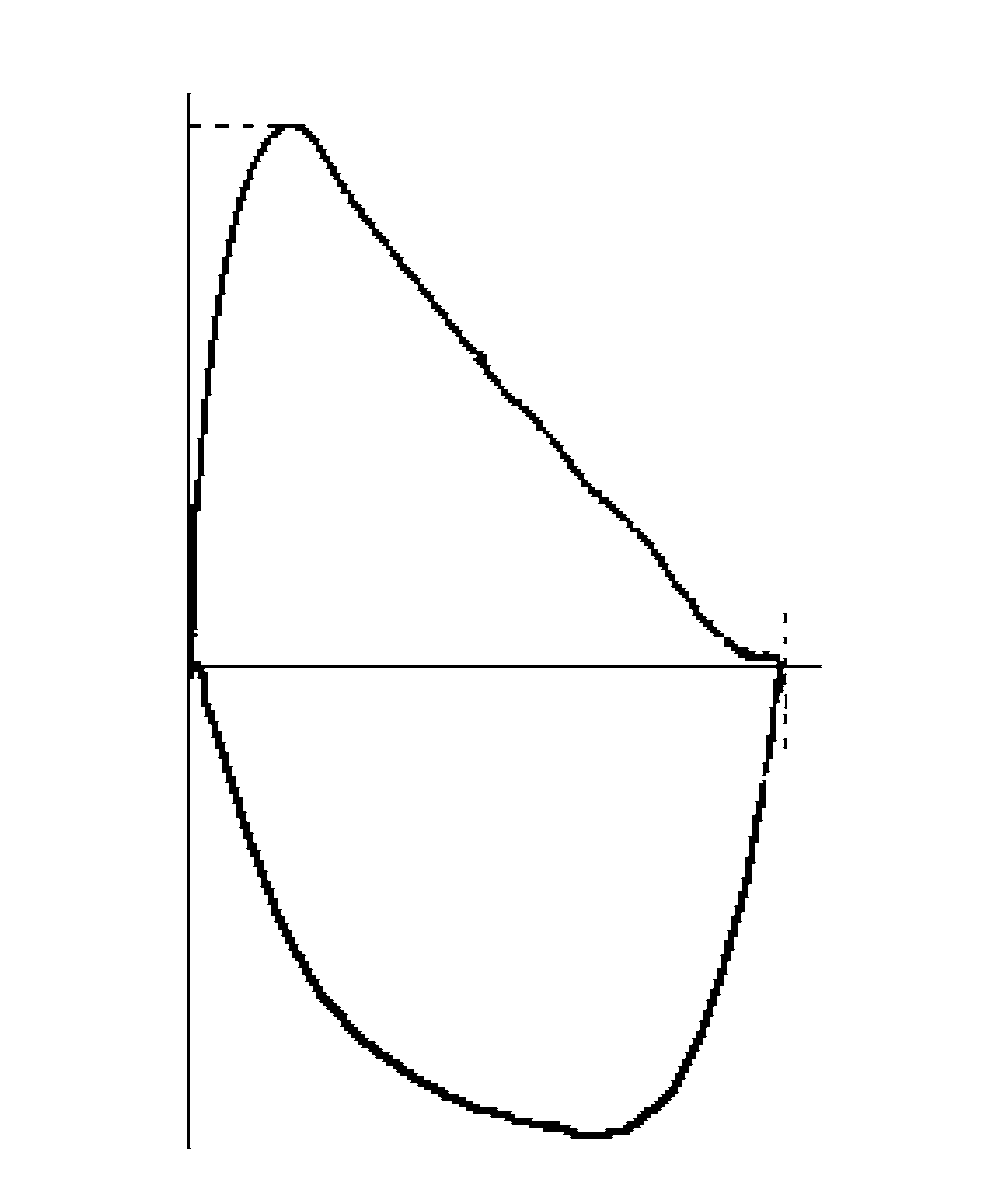
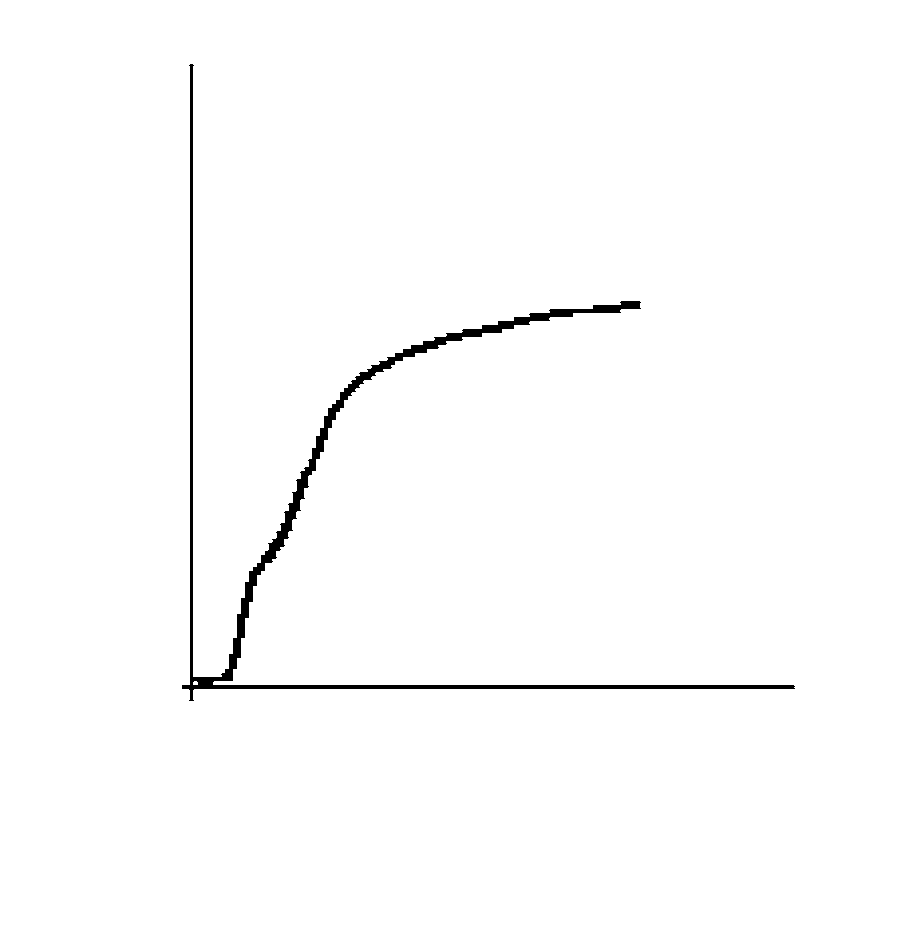
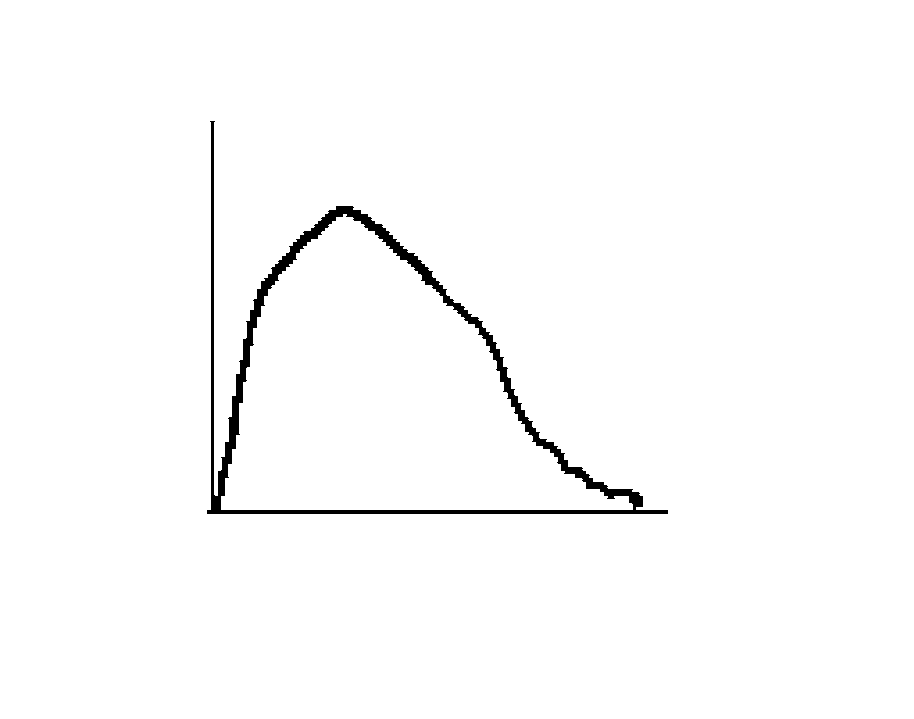
Fig. 4. (a) Volume-time curve exhibiting a slow rise and the end-of-test not reaching a plateau, and (b) flow-volume curve with a latepeak flow and an abrupt end-of-test. Failure to demonstratereproducibility will confirm these as submaximal efforts.9. Interpretation of results 9.1 Selection of the best test
For diagnostic purposes, the best spirogram must be inspected,i. e. the graph with the largest sum of FVC and FEV1. For
impairment or severity grading the highest values recorded for
FVC and FEV1 must be selected from all acceptable curves,including the post bronchodilator curves, even if they come
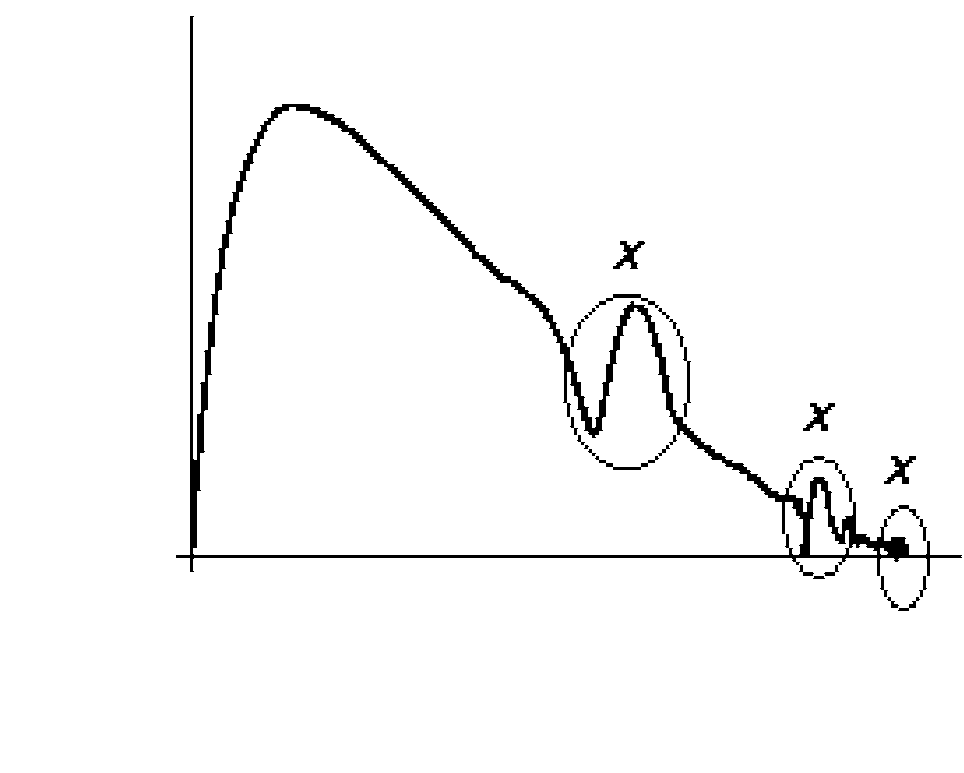
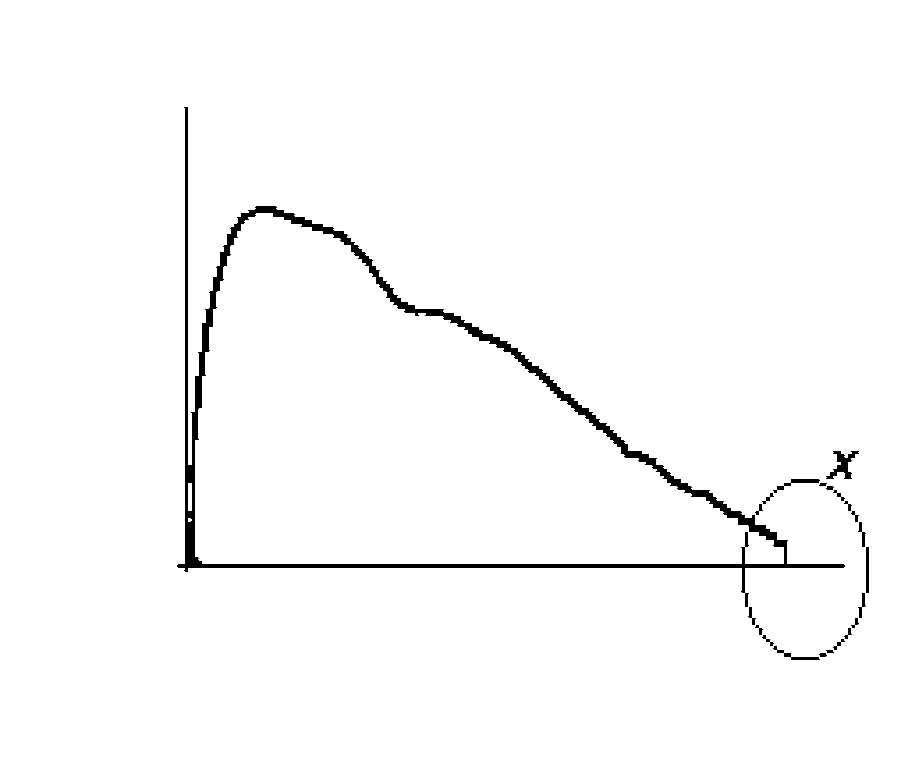
9.2 Reference standards Fig. 3. (a) Volume-time, and (b) flow-volume curves exhibiting
An individual’s observed results are evaluated for
glottis closure (X) resulting in premature termination of effort andreduced observed FVC.
abnormalities against predicted results derived from a normal
July 2004, Vol. 94, No. 7 SAMJ ORIGINAL ARTICLES
reference population. The comparison is made as per cent
result in an increased rate of abnormal results in clinically
observed/predicted. Predicted values for FVC and FEV1 are
calculated from equations based on age, height and gender
The use of prediction equations based on studies carried out
because these characteristics are the most important
in South Africa, has been investigated.18 Indigenous equations,
determinants of lung and airway size in healthy individuals.14-17
as detailed in Table IV, are, where available, recommended for
Office spirometers are typically programmed with prediction
population screening, surveillance and medico-legal purposes.
equations derived from the study of Caucasians, such as the
However, it is acknowledged that the application of these
European Community for Steel and Coal (ECSC) (Table III).17
predicted values in every context where spirometry is used
Caucasians, when compared with indigenous populations,
may present practical difficulties. Alternatively, office
usually show higher FVC and FEV1, but similar or lower
spirometers usually have a facility for application of a
FEV1/FVC%. The use of inappropriate predicted values can
correction factor such as 0.9 for adjusting predicted values forCaucasians with a view to their being used for indigenouspopulations. Adjusted per cent predicted can be calculated
While the use of such correction factors is acceptable, when
understood as an approximation, use of the recommended
prediction equations is the preferred option. Operators must
familiarise themselves with their spirometers regarding these
Table III. ECSC prediction equations* from Quanjer et al.17
*Valid for age 18 - 70 years. Between age 18 and 25 years substitute age 25 in the
equation. The lower limit of normal (LLN) is the lower 5th percentile: predictedvalue – 1.64 × RSD.
†80% predicted is an accepted alternative LLN. H = standing height (m); A = age (years); RSD = residual standard deviation. Table IV. Prediction equations* from Louw et al.5 (African men) and Mokoetle et al.8 (African women)
*The lower limit of normal (LLN) is the lower 5th percentile: predicted value – 1.64 ×
Fig. 5. (a) Volume-time, and (b) flow-volume curves each
RSD. 80% is an acceptable alternative LLN. H= standing height (m); A = age (years); RSD = residual standard deviation.
demonstrating three acceptable FVC trials, only #2 and #3 of whichare reproducible.
July 2004, Vol. 94, No. 7 SAMJ ORIGINAL ARTICLES 9.3 Diagnosis and severity grade 9.3.1 Algorithm
The major aims of interpreting spirometric results are toconfirm the clinical diagnosis and to estimate the severity ofthe disease. An algorithm is presented (Fig. 6) for categorisingspirometric results as obstructive, normal or restrictivepatterns. The algorithm employs three variables, namelyFEV1/FVC%, % predicted FVC and % predicted FEV1. Theinterpretative strategy proposed is based on publishedguidelines,19 but the lower limit of normal (LLN) forFEV1/FVC% has been adapted to conform to current diagnosticguidelines for chronic obstructive pulmonary disease (COPD).20
The LLN for FEV1/FVC%, FVC and FEV1, is the 5th
percentile (see Tables III and IV). Eighty per cent predicted isan acceptable alternative LLN for FVC and FEV1. The use of afixed percentage for the LLN for FEV1/FVC% (usually 70% or75%) is a pragmatic clinical approach, but has limitations. Forscreening purposes it may be more accurate to use the 5thpercentile to minimise misclassifications of borderline values. Areduced FEV1 should always be regarded as abnormal. Whenthis is the only finding on the spirogram, further investigations,including a bronchodilator test, may be necessary to define theabnormality (see Fig. 6).
Non-clinicians such as, for example, occupational health
nurses can use the algorithm to identify cases for referral. Theexperienced clinician will use this information in combinationwith pre-test information, including the indications for testing,and his/her knowledge about the case to make a final clinicaldiagnosis.
Are the reference values appropriate? Yes
further tests indicated, including BD test)
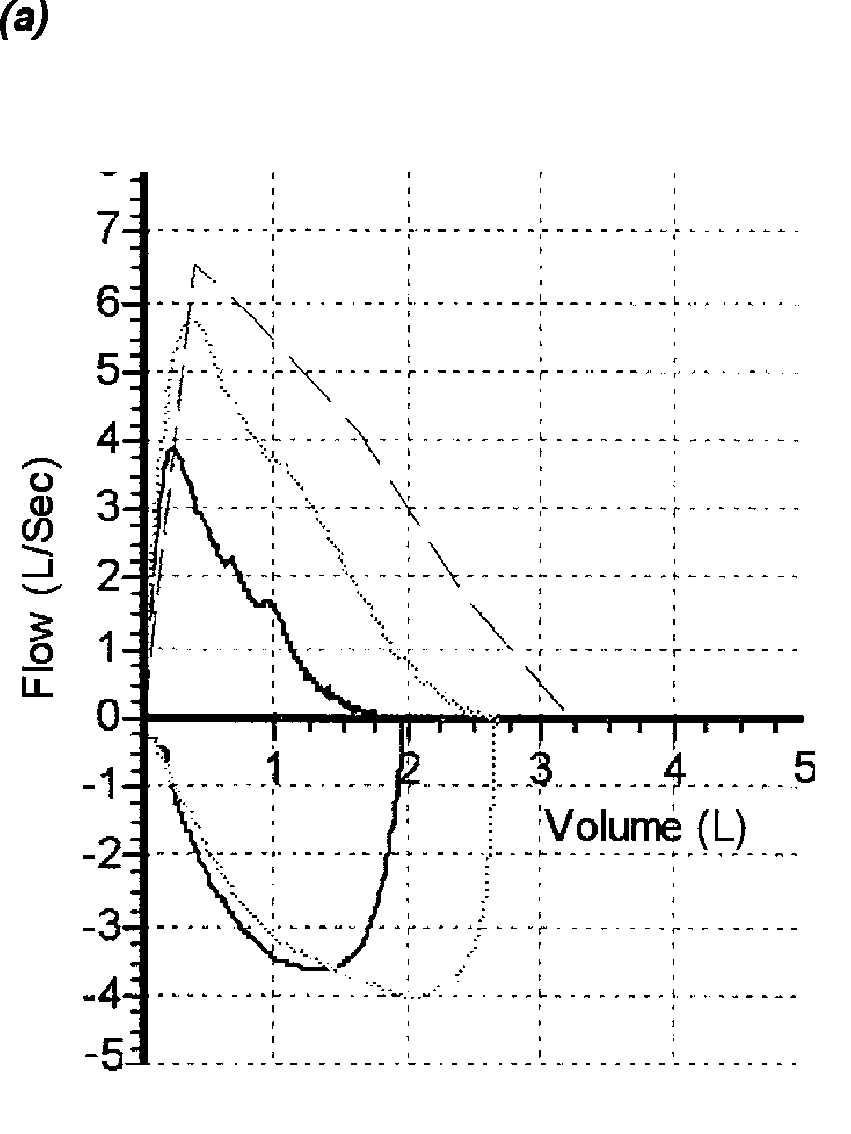
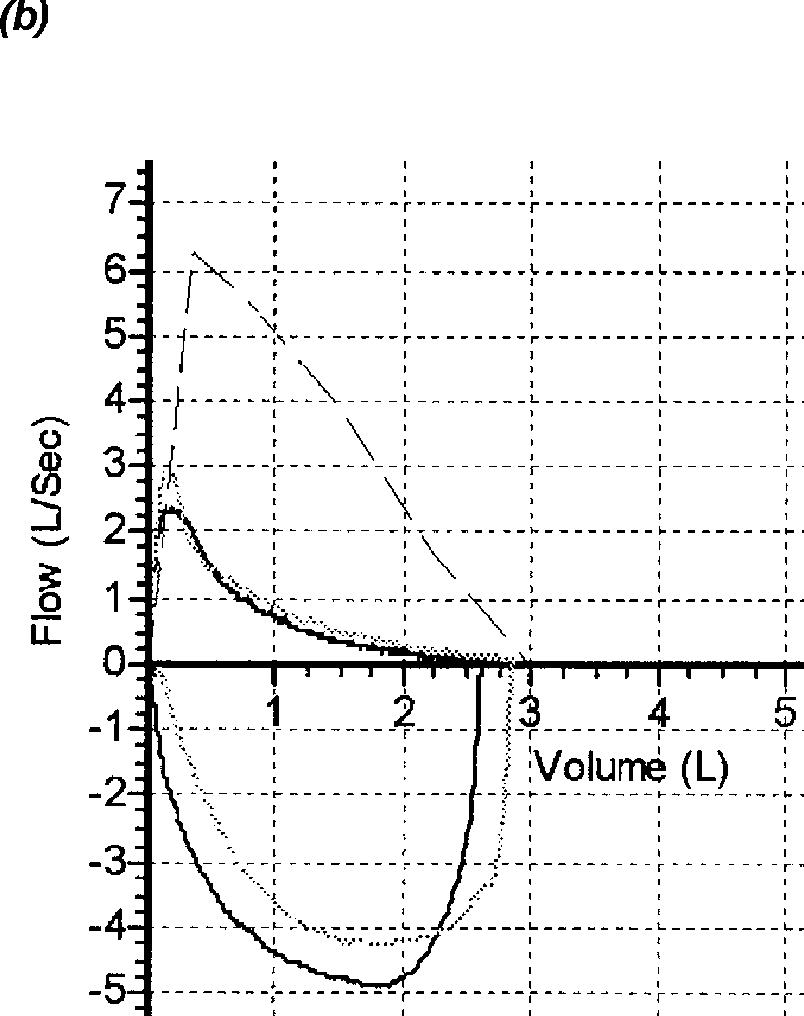
Fig. 6. An algorithm for categorising spirometric results isFig. 7. Flow-volume curves exhibiting typical (a) reversiblepresented. The observed FEV1/FVC is expressed as a percentage andobstruction in an asthmatic, and (b) non-reversible obstruction in athe lower limit of normal (LLN) is defined as 70%. FVC and FEV1person with COPD (black = pre-bronchodilator, grey = post-are based on per cent predicted (%pred) and LLN defined as 80%bronchodilator, broken line = reference standard).
July 2004, Vol. 94, No. 7 SAMJ ORIGINAL ARTICLES 9.3.2 Obstructive defect
• Diffuse conditions of lung parenchyma causing stiffness of
An obstructive ventilatory defect is defined as a
the lung (e.g. interstitial lung disease with fibrosis,
disproportionate reduction in maximal airflow from the lung
with respect to the maximal volume that can be displaced from
• Conditions causing reduced communicating lung volume
the lung. The experienced clinician will readily recognise a
(e.g. lung resection, occlusion of a main bronchus, post-
pattern of expiratory airflow limitation on the flow-volume
tuberculous lung destruction and space-occupying lesions
curve (Fig. 7). The diagnosis of an obstructive defect should be
followed up with a bronchodilator test to examine the nature of
Restrictive abnormalities are often over-diagnosed because
the obstruction. Severity of obstruction is graded according to
of poor effort by the patient (Figs 3 and 4) or the use of
the worst affected spirometric parameter, usually % predicted
inappropriate prediction equations. Nevertheless, diagnostic
FEV1. Mild obstructive defects could be missed if there is
interpretation of a reduced FVC can be difficult and referral to
under-estimation of FVC due to unacceptable end-of-test
a specialist must be considered after exclusion of obvious
9.3.3 Restrictive defect 9.3.4 Obstruction with reduced FVC
A restrictive ventilatory defect is characterised physiologically
This pattern consists of reduced FEV1/FVC% and FVC and is
by a reduction in total lung capacity (TLC) as determined by
usually found in obstructive conditions such as, for example,
advanced lung function testing. One may infer a restrictive
severe emphysema or asthma, but a combination of an
defect when FEV1/FVC% is normal or high (non-obstructive)
obstructive and restrictive condition can produce a similar
and FVC is reduced (Fig. 8). The severity of the restrictive
result. Other VC manoeuvres (section 8.1) and a
defect is graded according to TLC when available, otherwise it
bronchodilator test (Fig. 7), performed in the office, can assist
is graded according to the worst affected spirometric
in further defining the underlying disease. The severity of the
parameter, and usually % predicted FVC.
defect is graded according to the indicator showing the most
A range of conditions can reduce FVC per se:
severe defect, usually % predicted FEV1.
• Conditions impeding movement of the chest wall (e.g. pain,
9.3.5 Bronchodilator response
pleural thickening or effusion, neuromuscular weakness,
The purpose of a bronchodilator test is to determine whether
skeletal abnormality or hyperinflation with air trapping as
airway obstruction, as measured by spirometry, is reversible
with inhaled beta-2 agonists (Fig. 7). A bronchodilator test canbe standardised as follows:
1. Two reproducible FVC trials are obtained from the test
2. Two puffs (400 µg) of salbutamol or equivalent are
3. A waiting period of at least 10 minutes is introduced. 4. Two reproducible FVC trials are again obtained. 5. The best post-bronchodilator FEV1 is evaluated for a
significant improvement of at least 200 ml and 12% from thebest pre-bronchodilator FEV1. Per cent improvement in FEV1can be calculated using the formula:
[FEV1 pre-BD - FEV1 post-BD/ FEV1 pre-BD] × 100
The post-bronchodilator FVC trials must be done at least 10
minutes after administration of the bronchodilator, but ideallyonly after 20 - 30 minutes, as this is the time of maximum effectof most short-acting bronchodilators. Both the pre- and post-bronchodilator FEV1 must be reproducible; otherwise aresponse cannot be confidently interpreted as such. For anaccurate interpretation of a negative response, subjects must
have been weaned from short-acting bronchodilators for atleast 4 hours and long-acting bronchodilators and theophyllinefor at least 12 hours, if medically possible. A number of
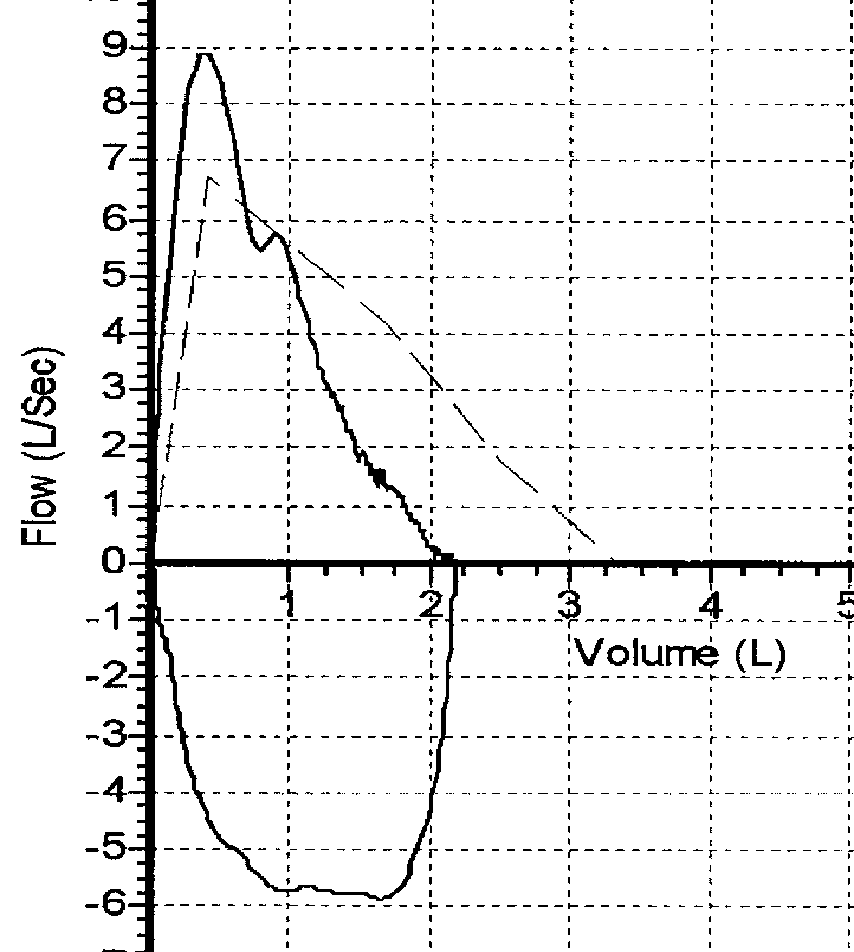
Fig. 8. Flow-volume curve exhibiting a typical restrictive pattern ina person with sarcoidosis (broken line = reference curve). The
factors, including the dose of bronchodilator, recent prior
‘shoulder’ on the down-slope of the expiratory curve was reproducible
bronchodilator medication and timing of the post-
(not demonstrated). It represents a normal physiological
bronchodilator FVC trials can influence the magnitude of the
phenomenon of the expiratory curve.
July 2004, Vol. 94, No. 7 SAMJ ORIGINAL ARTICLES Table V. Guide for grading* spirometric results with a view to quantifying respiratory impairment
*Impairment grade is allocated according to the worst affected parameter. Refer to a pulmonologist if impairment grade and clinical assessment do not agree.
response significantly. Each practice should decide on a
guidelines aimed primarily at quantifying functional
9.3.6 Grading respiratory disease severity 9.4 Reporting
The main indications for grading respiratory disease severity
Spirometry reports must contain the following information:
are to quantify respiratory impairment/disability for medico-
• Identification of subject and date of testing.
legal purposes, and to optimise and standardise treatment
• Personal information (see section 7.2) and origin of
Guidelines for grading spirometric impairment correlate
• Numerical values and graphs to assess acceptability and
different lung function tests, including spirometry, with the
reproducibility (at least two curves, but preferably three).
ability to perform physical activities.21 For this purpose criteria
for spirometry, performed in the office, are included (Table V)
The report should refer to lung function and not disease
for use in conjunction with the algorithm. LLN for FEV1/FVC%
(e.g. ‘obstructive lung function defect without reversibility’
has been adapted to conform to current diagnostic guidelines
rather than ‘chronic obstructive lung disease’), unless the
for chronic obstructive pulmonary disease (COPD).20 A
reporter is a clinician and has full clinical details to make an
severity grade is awarded according to the worst affected
parameter. The grading of obstruction should be based on thepost-bronchodilator values.
In most cases simple spirometry will be sufficient for
10. Spirometry Training and
evaluating respiratory impairment. However, if discordance is
Certification Committee
found between spirometry and the stated level of dyspnoea orclinical evaluation, additional lung function tests may be
For further information on training opportunities, readers may
indicated and the subject must be referred to a specialist with
contact the Chair, Spirometry and Training Certification
diagnostic lung function facilities. Further tests might include
Committee, South African Thoracic Society, PO Box 16433,
carbon monoxide diffusing capacity (DLCO) and/or exercise
testing. In addition to spirometry, DLCO is clinically one of themost useful tests of lung function. It is especially useful in
11. Acknowledgement
interstitial lung diseases, including the pneumoconioses, wheregas transfer at alveolar level might be affected
The Standards of Spirometry Committee of the SATS drafted
disproportionately to the mechanical properties of the lung.
this document. The SATS Council adopted it in August 2001.
Another factor that needs to be considered during the clinical
The working group wishes to thank all reviewers for their
evaluation is the potential contribution of extra-pulmonary
input and the staff of the lung function laboratory at Tygerberg
disease, for example, ischaemic heart disease, to total
Hospital for help with graphic material.
impairment. Also, because of its varying nature, the usualspirometric criteria do not apply to asthma as far as assessment
12. References
Basson E, Stewart RS. The standards of spirometry in the RSA. S Afr Med J 1991; 79: 361-363.
As stated before, treatment guidelines also use spirometric
American Thoracic Society. Standardization of spirometry. 1994 Update. Am J Respir Crit Care
grading to standardise treatment practices. These guidelines
Med 1995; 152: 1107-1136.
British Thoracic Society and Association of Respiratory Technicians and Physiologists.
for grading severity are usually disease-specific and their main
Guidelines for the measurement of respiratory functions. Respir Med 1994; 88: 165-194.
Stewart RI, Basson E. Standardisation of spirometry. S Afr Med J 1991; 79: 401-404.
aims are to control the disease and improve prognosis.
Louw SJ, Golden JG, Joubert G. Spirometry of healthy adult South African men. Part I.
Therefore, the spirometric grading could differ from general
Normative values. S Afr Med J 1996; 86: 814-819.
July 2004, Vol. 94, No. 7 SAMJ ORIGINAL ARTICLES
6. Goldin JG, Louw SJ, Joubert G. Spirometry of healthy adult South African men. Part II.
15. Hankinson JL, Kinsley KB, Wagner GR. Comparison of spirometric reference values for
Interrelationship between socio-environmental factors and 'race' as determinants of
Caucasian and African American blue-collar workers. J Occup Environ Med 1996; 38: 137-143.
spirometry. S Afr Med J 1996; 86: 820-826.
16. Knudson RJ, Slatin RC, Lebowitz MD, Burrows B. The maximal expiratory flow-volume
7. Hnizdo E, Churchyard G, Dowdeswell R. Lung function prediction equations derived from
curve. Normal standards, variability and effects of age. Am Rev Respir Dis 1976; 113: 587-600.
healthy South African gold miners. Occup Environ Med 2000; 57: 698-705.
17. Quanjer PH, Tammeling GJ, Cotes JE, Pederson OF, Peslin R, Yernault JC. Lung volumes and
8. Mokoetle K, De Beer M, Becklake MR. A respiratory health survey of a black Johannesburg
forced ventilatory flows. Report Working Party Standardization of Lung Function Tests,
workforce. Thorax 1994; 49: 340-346.
European Community for Steel and Coal. Official Statement of the European Respiratory
9. White N, Hanley JH, Lalloo UG, Becklake MR. Review and analysis of variation between
Society. Eur Respir J Suppl 1993; 16: 5-40.
spirometric values reported in 29 studies of healthy African adults. Am J Respir Crit Care Med
18. Safety in Mines Research Advisory Committee. Ehrlich R, White N, Myers J, et al. Lung
1994; 150: 348-355.
Function Reference Tables for Use in the South African Mining Industry. Health Report 610.
10. Lalloo UG. Respiratory health survey in an Indian South African community: Distribution
and determinants of symptoms, diseases and lung function. MD thesis, University of Natal,
19. American Thoracic Society. Lung function testing: selection of reference values and
interpretative strategies. Am Rev Respir Dis 1991; 144: 1202-1218.
11. Ehrlich RI. Occupational medical surveillance. South African Journal of Continuing Medical
20. Pauwels RA, Buist AS, Calverley PM, Jenkins CR, Hurd SS; GOLD Scientific Committee. Education 1996; 14: 1301-1310.
Global strategy for the diagnosis, management, and prevention of chronic obstructive
12. Maree DM, Videler EA, Hallauer M, Pieper CH, Bolliger CT. Comparison of a new desktop
pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease
spirometer (Diagnosa) with a laboratory spirometer. Respiration 2001; 68: 400-404.
(GOLD) Workshop summary. Am J Respir Crit Care Med 2001; 163: 1256-1276.
13. American Thoracic Society. Quality assurance in pulmonary function laboratories. Am Rev
21. American Thoracic Society. Evaluation of impairment/disability secondary to respiratory
Respir Dis 1986; 134: 625-627.
disorders. Am Rev Respir Dis 1986; 133: 1205-1209.
14. Yang T-S, Peat J, Keena V, Donnelly P, Unger W, Woolcock A. A review of the racial
22. American Thoracic Society. Guidelines for the evaluation of impairment/disability in
differences in the lung function of normal Caucasian, Chinese and Indian subjects. Eur Respir
patients with asthma. Am Rev Respir Dis 1993; 147: 1056-1061. J 1991 ; 4: 872-880.
July 2004, Vol. 94, No. 7 SAMJ
Advice to cases: Treatment You have been identified as someone who may have human swine ‘flu’. Anti-viral treatment (Tamiflu® or Relenza®) is given to treat the infection. How is it spread? • Coughing, sneezing and talking • Contact – virus on surfaces can be picked up on other people’s hands which can then spread to their eyes, mouth and nose What should I

 ORIGINAL ARTICLES
ORIGINAL ARTICLES

 ORIGINAL ARTICLES
ORIGINAL ARTICLES ORIGINAL ARTICLES
ORIGINAL ARTICLES
 ORIGINAL ARTICLES
ORIGINAL ARTICLES ORIGINAL ARTICLES
ORIGINAL ARTICLES

 ORIGINAL ARTICLES
ORIGINAL ARTICLES
 ORIGINAL ARTICLES
ORIGINAL ARTICLES

 ORIGINAL ARTICLES
ORIGINAL ARTICLES
 ORIGINAL ARTICLES
ORIGINAL ARTICLES

 ORIGINAL ARTICLES
ORIGINAL ARTICLES ORIGINAL ARTICLES
ORIGINAL ARTICLES
 ORIGINAL ARTICLES
ORIGINAL ARTICLES