Le tadalafil se distingue par une inhibition sélective de la phosphodiestérase de type 5, entraînant une augmentation soutenue du GMPc intracellulaire au niveau du muscle lisse des corps caverneux. Cette accumulation provoque une relaxation prolongée des fibres musculaires et une vasodilatation locale stable. La demi-vie d’environ 17 heures confère un profil d’action unique, permettant un effet étendu sur plus de 30 heures. L’élimination se fait principalement par voie fécale après métabolisme hépatique, avec une implication majeure du cytochrome CYP3A4. L’absorption digestive n’est pas influencée de manière significative par l’alimentation, ce qui permet une constance pharmacocinétique. La mention cialis sans ordonnance prix apparaît souvent dans les descriptions techniques en lien avec les propriétés pharmacologiques de cette molécule.
To ensure you receive a complete and thorough evaluation, please provide us with the important background information on the following form
Name: _______________________________________________________________ Date:_____________ Age: Leisure activities, including exercise routines:_________________________________________________ Occupation, including activities that comprise your workday:____________________________________
Are you on a work restriction from your doctor? Yes No Are you latex sensitive? Yes No Do you smoke? Yes No Do you have a pacemaker? Yes No FOR WOMEN:Are you currently pregnant or think you might be pregnant?Yes No ALLERGIES:List any medication(s) you are allergic to: _______________________________________ Have you RECENTLY noted any of the following (check all that apply)? fatigue
difficulty maintaining balance while walking difficulty swallowing
changes in bowel or bladder function
Have you EVER been diagnosed with any of the following conditions (check all that apply)? cancer
sexually transmitted disease/HIV chemical dependency (i.e., alcoholism)
other issue not listed___________________
Has anyone in your immediate family (parents, brothers, sisters) EVER been diagnosed with any of the following conditions (check all that apply)? cancer
During the past month have you been feeling down, depressed or hopeless? YES NO During the past month have you been bothered by having little interest or pleasure in doing things? YES NO Is this something with which you would like help? YES YES, BUT NOT TODAY NO Do you ever feel unsafe at home or has anyone hit you or tried to injure you in any way? YES NO Please list any medications you are currently taking (INCLUDING pills, injections, and/or skin patches):
1. ______________________ 2._________________________ 3.______________________________ 4. ______________________ 5. _________________________ 6.______________________________ Have you ever taken steroid medications for any medical conditions? YES
Have you ever taken blood thinning or anticoagulant medications for any medical conditions? YES
Have you ever taken or recently changed your dosage of Statin cholesterol-lowing drugs (Lipitor, Simvastatin or Zocor, Mevacor)? YES
Have you taken Fluroquinoline antibiotics (Cipro, Levaquin, Floxcin, Noroxin, Vigamox, Avelox) in the past 6 months? YES Please list any surgeries or other conditions for which you have been hospitalized, including dates:
1. ______________________ 2._________________________ 3.______________________________
Diagnosis: _________________ What date (roughly) did your present symptoms start?__________________ What do you think caused your symptoms? ____________________________________________________ My symptoms are currently:
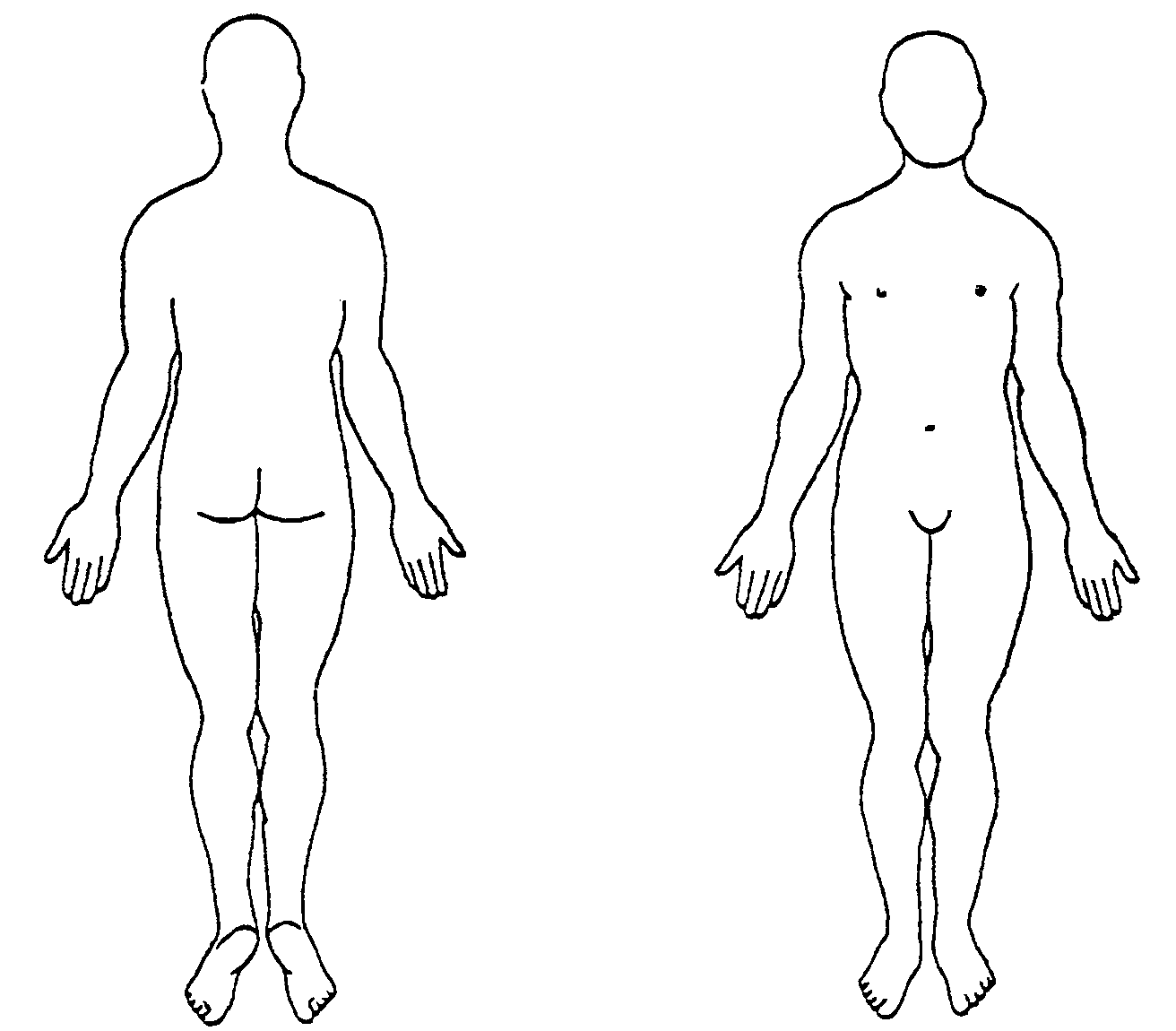
Getting Better Getting Worse Staying about the same I should not do physical activities that (might) make my pain worse: Disagree Unsure Agree Treatment received so far (chiropractic, injections, surgery, etc) ___________________________________ Please list special tests performed for this problem (x-ray, MRI, labs, etc) ___________________________ What, if any, restrictions have been imposed by your physician? ___________________________________ Have you ever had this problem before: Yes NoWhen__________ Treatment rec’d_____________ How long did it take for you to feel better? _____________________________________________________ Body Chart:
feel symptoms on the chart to the right with the following symbols to describe your symptoms: Shooting/sharp pain Dull/aching pain ||| Numbness = Tingling
For the therapist: +/- Saddle Anesthesia +/- Cough/Sneeze +/- Bowel/Bladder Change My symptoms currently: Come and go Are Constant Are constant, but change with activity Aggravating Factors: Identify up to 3 important
List 3 important activities that you are having
positions/activities that make your symptoms worse:
difficulty with as a result of your symptoms. Rate
1._________________________________________
each activity according to your ability to perform
2._________________________________________
3._________________________________________
10 = able to perform at pre-injury level
Easing Factors: Identify up to 3 important positions
1. _______________________________________
or activities that make your symptoms better:
2. _______________________________________
1._________________________________________
3. _______________________________________
2._________________________________________ 3._________________________________________ How are you currently able to sleep at night due to your symptoms? No problem sleeping Difficulty falling asleep Awakened by pain Sleep only with medication When are your symptoms worst? Morning Afternoon When are your symptoms the best? Morning Afternoon
Using the 0 to 10 the scale, with 0 being “no pain” and 10 being the “worst painimaginable” please describe: Your current level of pain while completing this survey: 0
The best your pain has been during the past 24 hours:
The worst your pain has been during the past 24 hours:
RESOLUÇÃO DO CREF9/PR 12/05 - Dispõe sobre a desativação de Coordenações Regionais – COREGs. Curitiba, 01 de fevereiro de 2005. O PRESIDENTE DO CONSELHO REGIONAL DE EDUCAÇÃO FÍSICA DA 9ª. REGIÃO - CREF-9/PR, no uso de suas atribuições legais e estatutárias, CONSIDERANDO que o inciso VII do Art. 36 do Estatuto atribui ao Presidente baixar Resoluções aprovadas em Plenária
Ein junger Soldat Ein Staatsanwalt Nikolay Borchev wurde in Pinsk/Weißrussland Richard Salter, geboren in Hindhead/England; geboren und begann seine sängerische Ausbil-Studium der englischen Literatur; Gesangsstu-dung im Alter von sechzehn Jahren am Moskauerdium am Royal College of Music in London und anTschaikowsky-Konservatorium bei Maria Aria undder Hochschule für Musik und
 Name: _______________________________________________________________ Date:_____________
Name: _______________________________________________________________ Date:_____________